
Abstract
Background:
The Combined Quality Care Anterior Cruciate Ligament registry provides data for clinical research regarding primary anterior cruciate ligament (ACL) surgery.
Purpose:
To explore the data with regard to the clinical outcomes between sexes after ACL reconstruction in a Dutch population.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data involving patients diagnosed with an ACL tear and eligible for surgery were recorded. Isokinetic muscle strength, functional muscle performance, and anterior-posterior translation of the knee joint were documented preoperatively and at 3, 6, 9, and 12 months postoperatively. Patients completed the Knee Injury and Osteoarthritis Outcome Score (KOOS), Lysholm, and Tegner rating scales during each examination using a web-based questionnaire.
Results:
Approximately 90% of ACL injuries occurred during sport activities. The mean (SD) age at surgery was 28 (11) years for both men and women, and the majority of patients were treated with hamstring tendon autografts (94%). Four percent received bone–patellar tendon–bone autografts, and 2% of the patients received other grafts. Preoperatively, the KOOS, Lysholm, and Tegner scores were significantly higher in males. Twelve months postoperatively, both sexes showed comparable isokinetic strength (P = .336), knee laxity (P = .680), and hop test for distance (P = .122) when comparing the injured with the uninjured side. Self-reported knee function was comparable between sexes as assessed by the KOOS (P = .202), Lysholm (P = .872), and Tegner (P = .767) questionnaires during the 12-month follow-up.
Conclusion:
One year after ACL surgery, all patients had improved greatly, showing only minor differences between sexes. The male group showed slightly better results when evaluating self-reported knee questionnaires. Comparable outcomes and knee function between sexes can therefore be presumed with patients who are treated with hamstring tendon autografts in a Dutch population.
Clinical Relevance:
These results can be used during the clinical evaluation of patients who are eligible for ACL reconstruction.
Anterior cruciate ligament (ACL) tears occur frequently among young athletes during activities that include pivot maneuvers. 5,30 Repeated loading could cause the ACL to fail suddenly under routine landing conditions, especially when muscle fatigue occurs. 30 Diagnosis of ACL tears relies on injury history, clinical examination, magnetic resonance imaging, and arthroscopy. 11,15,31 The most common indication for reconstructive surgery is the desire of the athlete to return to sport, whereas the aim is to restore the mechanical stability of the knee. The primary goal is to achieve preinjury sport activity level and reduce the perception of instability in daily living. 27 However, only approximately 33% of patients will play a competitive sport at their preinjury level after ACL reconstruction, and only 67% will return to some form of sport participation at 12 months after surgery. 6 The timing of return to unrestricted sport activity and how level of performance could be affected due to ACL surgery are still major issues within the rehabilitation process. 55 The most frequently used evaluation methods for return to sport are measurements of knee laxity, range of motion, isokinetic muscle strength, and functional tests such as the 1-legged hop test for distance. 38,39,49 In addition, self-reported questionnaires such as the Knee Injury and Osteoarthritis Outcome Score (KOOS), Lysholm, and Tegner are used to evaluate subjective knee functionality when deciding to resume sport activities. 3,39,49 However, little is known about differences in clinical outcomes between males and females and whether sex differences influence rehabilitation. The majority of the studies focus on investigating risk factors that predict inferior outcomes between sexes. For instance, it is known that the incidence of ACL ruptures is higher in females because of anatomic factors such as the width of the intercondylar notch, as well as neuromuscular function, and physiological factors such as hormonal regulation. 14,46,50 Only a few studies 1,14,17,44,49 have critically analyzed sex differences in clinical outcomes following ACL reconstruction. To our knowledge, no studies have yet been conducted that evaluate possible differences between sexes at regular intervals during the first year after surgery. Our intention was not only to report on postoperative outcomes but also to report results of the course of recovery during the first year after ACL reconstruction. The primary aim of this study was to present pre- and postoperative measurements of patients who were eligible for primary ACL reconstruction with emphasis on differences between the sexes in a Dutch population. Patients were eligible for surgery when they were diagnosed with an ACL tear and experienced instability during daily living or sport activities. Furthermore, the secondary aim of this study is to report patient demographics and injury occurrence based on data collection from a relatively large cohort.
Methods
Research Design
A retrospective case series design was used to evaluate pre- and postoperative measurements of patients who were eligible for ACL reconstruction surgery. This study was approved by the medical ethical committee of Maastricht University Medical Centre, Maastricht, the Netherlands.
Data Collection
This retrospective study included men and women who were eligible for arthroscopic ACL reconstructive surgery. Data for analysis were acquired by the first author (X.M.T.) from the Combined Quality Care (CQC) Anterior Cruciate Ligament registry. This web-based registry collects outcome scores of the patient during pre- and postoperative measurements. Each patient’s health record was divided into 3 components containing personal information, including screening, surgery, and clinical measurements. In the screening section, information regarding age, smoking, ethnicity, the mechanism of injury, and the activity during which the injury occurred was documented. An orthopaedic surgeon registered the surgical information such as graft selection and duration of the surgical procedure. Isokinetic strength and knee laxity measurements were performed preoperatively by (sport) physical therapists and were repeated at 3, 6, 9, and 12 months after surgery. Patients also completed the KOOS, Lysholm, and Tegner questionnaires during each examination. The physical therapists who performed clinical measurements were required to attend special practical training courses provided by the CQC. During these courses, the therapists were taught the same techniques for all clinical measurements, thus enhancing intertester reliability and minimizing variability. All retrievable data were selected for analysis from patients undergoing ACL reconstruction between November 1, 2008, and February 28, 2013. A personal registration number was assigned to each patient for maintaining complete anonymity during data extraction.
Because of multiple measurements, there was a large group of patients who were not measured at all the intervals. Therefore, we chose to use and analyze all available data from each health record for evaluating preliminary results. ACL revisions could, however, not be identified separately in the register, and consequently, are included in the analyses of postoperative outcomes of primary ACL reconstruction. However, according to a recent systematic review, the expected revision rate after primary ACL reconstruction is approximately 5.8% at a minimum of 5 years of follow-up. 58 Because of this relatively low incidence of revision, it can be presumed that inclusion of these patients may not bias the results.
Outcome Measures
Isokinetic Muscle Strength
Bilateral isokinetic strength of the thigh muscles was measured with the Biodex Dynamometer System 3 and 4 (Biodex Medical Systems Inc). 23 The patient was seated with the hip flexed to 90°. This position was maintained during the test by straps secured around the chest, hip, and thigh. To determine the height of the chair, the lateral femoral condyle was aligned with the rotational axis of the dynamometer. The arm of the dynamometer was secured to the tibia approximately 2 cm above the malleoli. The quadriceps and hamstring peak torques were measured in newton meters (N·m), with knee angle velocities at 60 deg/s (5 repetitions) and 180 deg/s (20 repetitions) where the noninvolved side was tested first. The rest period between the velocities was 45 seconds for preventing muscle fatigue. Before each test, the patient was instructed to perform 2 practice repetitions. A standardized protocol was used during measurements for enhancing reproducibility and consistency. The peak torque of the involved side was divided by the noninvolved side and multiplied by 100 for calculating the side-to-side difference in percentages. A negative value indicates a strength deficit of the involved side. Isokinetic strength was tested during all follow-up measurements. Strength testing within the first year after surgery has been examined previously and has shown to be reliable and safe when evaluating quadriceps and hamstring muscle recovery. 33,56
Knee Laxity Measurement
The instrumented KT-2000 knee arthrometer (MEDmetric Co) was used during the clinical examination for measuring the anterior-posterior (AP) translation at a knee angle of 30° using a force of 132 N. 22,26,40,47 The patient was placed in a supine position where the arthrometer was secured to the tibia using 2 straps. 16 The instrument was calibrated to 0° before each displacement test. The noninvolved side was tested first and compared with the involved side, whereas side-to-side differences in millimeters were calculated.
One-Legged Hop for Distance
Functional muscle performance was tested using the 1-legged hop test for distance. Each subject performed 2 practice trials followed by 2 test trials. When the subject increased the distance of the second test trial, additional trials were performed until no improvement was seen. During each trial, patients were asked to maintain both hands on their lower back, and free swings of the contralateral leg were allowed. The uninvolved limb was tested first and the distance was measured in centimeters from the toe at the push-off line to the heel where the subject landed. 21,41 The limb symmetry index (LSI) score was calculated by dividing the result for the involved limb by that of the uninvolved limb and multiplied by 100. An LSI score of <90% is considered as abnormal and ≥90% as normal. Hop tests were not performed during the 3-month postoperative measurement because of the high likelihood of sustaining a second injury. The first postoperative evaluation of the 1-legged hop test was performed during the 6-month follow-up measurement, in accordance with the study of Gustavsson et al. 21
Knee Rating Scale Scores
The Knee Injury and Osteoarthritis Outcome Score (KOOS) was used to assess subjective knee function and consists of 5 different subscales: (1) pain, (2) symptoms, (3) function in daily living, (4) function in sport and recreation, and (5) knee-related quality of life. The score for each subscale was calculated, where 0 indicates severe knee problems and 100 indicates no knee problems. The KOOS questionnaire has been found to be useful and valid when evaluating clinical functionality after ACL reconstruction. 48 The Lysholm score was used for the evaluation of knee symptoms and functional impairments. 10,24,32,53 A score of 0 represents major disability or symptoms due to knee problems, and a score of 100 represents no limitations. The Tegner score was used for scoring a person’s activity level between 0 and 10, where 0 represents being on sick leave/disabled and 10 represents participation in competitive sports at the (inter)national elite level. The combination of Lysholm score and Tegner score has shown to be valid in the evaluation of the return of function after ACL reconstruction. 13
Statistical Analyses
Demographic characteristics and baseline variables were described using frequencies and percentages. Means ± SDs are reported for continuous variables and median (range) for ordinal variables. The Kolmogorov-Smirnov test was used for testing normality of the variances. Differences between groups were analyzed using the independent t test for parametric continuous variables, and the Mann-Whitney U test for nonparametric continuous variables. The Pearson χ2 was used for dichotomous variables. The total number of included patients in the analysis for each measurement was presented in the appropriate tables. Significance level was set at P < .05, and analyses were performed using SPSS version 20.0 (IBM Corp).
Results
Demographics
A total of 375 surgical records were identified. A summary of demographics and baseline values are presented in Table 1. The mean age at surgery was 28 ± 10 years for male patients and 28 ± 11 years for female patients, and the mean duration of surgery was 61.5 ± 23 minutes for men and 59.7 ± 19 minutes for women. The percentage of active smokers was significantly higher (P = .019) among men (24%) than among women (14%). The majority of the study population was white (93%). No significant differences were found in ethnicity between sexes (P = .333). The majority of the patients received hamstring tendon (HT) autografts (94%), 4% received bone–patellar tendon–bone (BPTB) autografts, and 2% received other grafts. No significant differences were noted between sexes when evaluating the prevalence of HT (P = .296) and BPTB (P = .427) autografts. The most common activity of injury occurrence was sports participation (89%) or daily activities (6%).
Demographic Characteristics and Baseline Epidemiology a

a Values are expressed as frequencies (%) unless otherwise indicated. P value in boldface indicates statistical significance (P < .05). ADL, activities of daily living; BPTB, bone–patellar tendon–bone; HT, hamstring tendon.
Isokinetic Muscle Strength
Isokinetic thigh muscle strength measurements were retrieved for 624 patients (61% male, 39% female). The pre- and postoperative side-to-side strength deficits are presented in Table 2. Significant differences were noted between sexes when evaluating quadriceps peak torque at 180 deg/s preoperative (P = .016) and 3 months postoperative (P = .010). No statistical differences in side-to-side strength deficits were found 12 months after surgery when comparing quadriceps peak torque at 60 deg/s (P = .621) and 180 deg/s (P = .336) and hamstring peak torque at 60 deg/s (P = .632) and 180 deg/s (P = .416).
Isokinetic Strength, Quadriceps and Hamstrings a
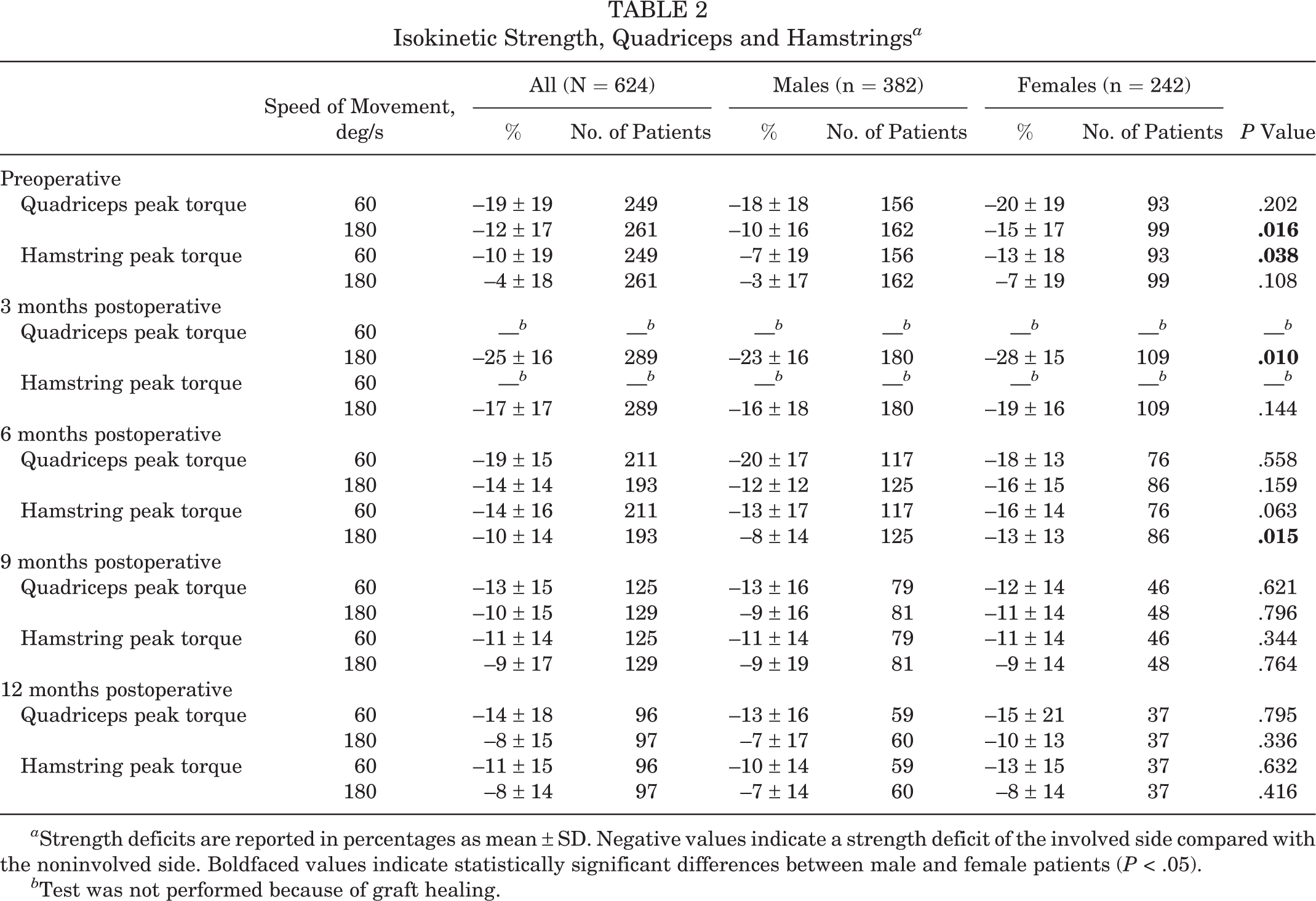
a Strength deficits are reported in percentages as mean ± SD. Negative values indicate a strength deficit of the involved side compared with the noninvolved side. Boldfaced values indicate statistically significant differences between male and female patients (P < .05).
b Test was not performed because of graft healing.
Knee Laxity
Knee laxity measurements were available for 493 patients (65% male, 35% female). The mean difference in AP translation of the knee joint was 3.9 mm preoperative and 1.8 mm postoperative when comparing the involved and noninvolved sides. We found no statistically significant differences between sexes in mean side-to-side differences during preoperative (P = .903) and postoperative (P = .680) measurements (Table 3). In addition, 26 of the 99 female patients (26%) and 35 of the 123 male patients (29%) had >3 mm side-to-side difference during postoperative measurements (P = .716).
Knee Laxity a
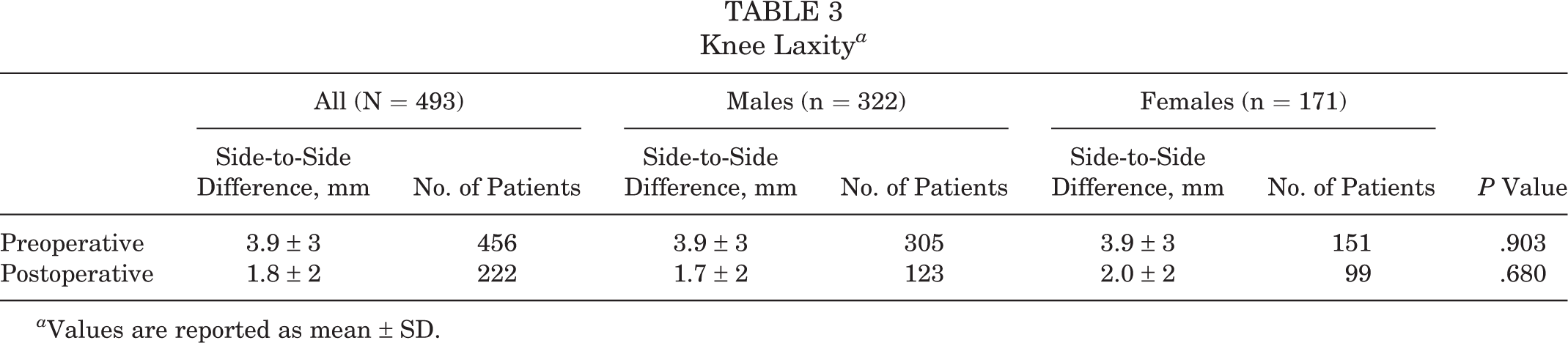
a Values are reported as mean ± SD.
One-Legged Hop Test for Distance
One-legged hop test data were available for 529 patients (58% male, 42% female). The LSI score of the pre- and postoperative measurements is presented in Figure 1. Preoperative, 6-, 9-, and 12-month measurements were available for 295 (59% male, 41% female), 217 (53% male, 47% female), 138 (62% male, 38% female), and 64 (63% male, 37% female) patients, respectively.
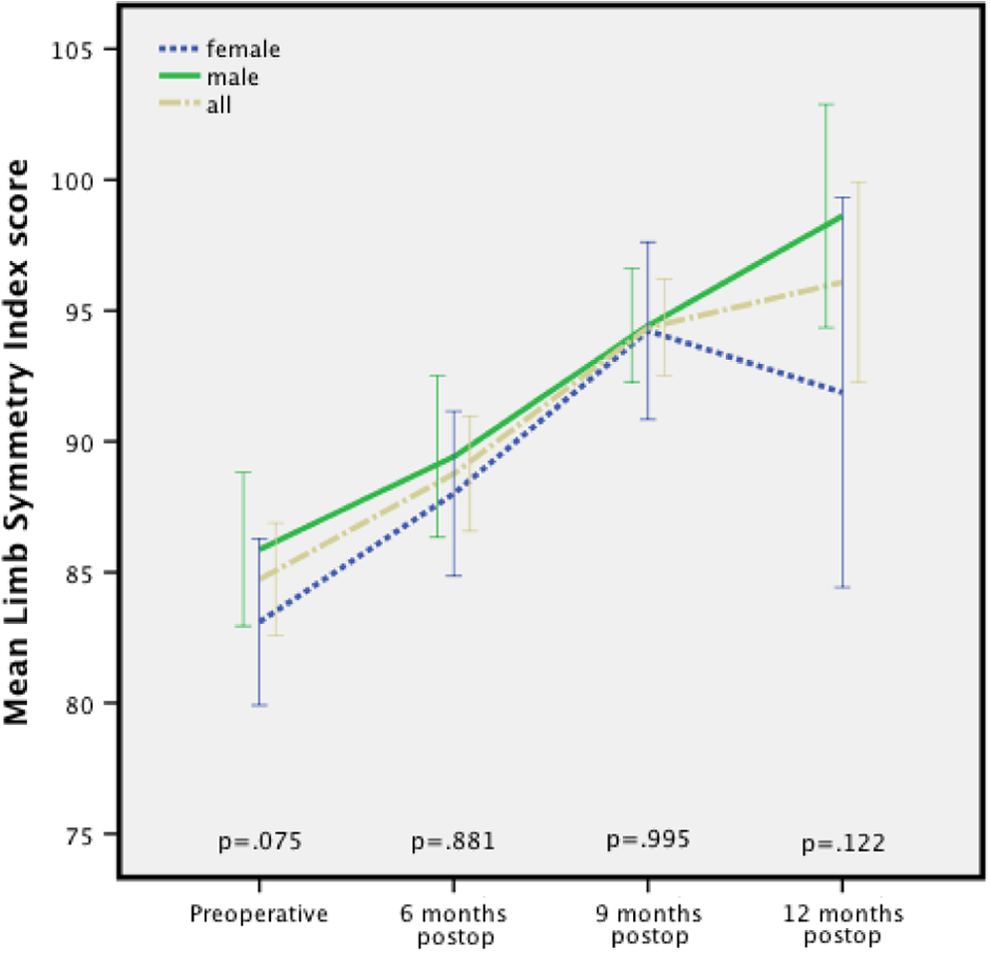
Mean limb symmetry index scores.
Knee Rating Scale Scores
Lysholm scores were available for 1052 patients (62% male, 38% female), Tegner scores were available for 790 patients (65% male, 35% female), and KOOS scores were available for 790 patients (64% male, 36% female). The mean scores for the Lysholm, Tegner, and KOOS questionnaires during all measurements are presented in Figures 2, 3, and 4, respectively. During the first 9 months, there were some minor differences between the sexes, where male patients tended to present higher outcome scores on the self-reported questionnaires. However, at 12 months after surgery, there were no differences between sexes in the KOOS (P = .202), Lysholm (P = .872), and Tegner scores (P = .767).

Mean Lysholm scores. Boldfaced P values indicate statistical significance.

Mean Tegner scores. Boldfaced P values indicate statistical significance.

Mean Knee Injury and Osteoarthritis Outcome Score (KOOS) for subscales (A) symptoms, (B) pain, (C) daily living, (D) sport/recreation, and (E) quality of life. Boldfaced P values indicate statistical significance.
Discussion
The CQC Anterior Cruciate Ligament registry provides epidemiological data of patients who were eligible and underwent primary ACL reconstructive surgery. The general conclusion of the present study is that 12 months after surgery, no significant differences were noted between sexes when evaluating isokinetic strength, knee laxity, 1-legged hop test for distance, and subjective knee function as measured by the KOOS, Tegner, and Lysholm questionnaires. These findings are in accordance with previous results. 3 However, this study differs from previous studies because, to our knowledge, no detailed results have yet been reported of clinical measurements that were obtained from a large cohort at regular intervals during the rehabilitation phase (<1 year). The aim of this study was not only to present results using the most commonly used health questionnaires but also to present overall scores of objective measurements such as isokinetic strength, knee laxity, and hop tests. The results of this study can be used during the rehabilitation following ACL reconstruction to evaluate overall knee function. These clinical measurements allow surgeons to monitor the health status of the patient more adequately. Significant differences were found between sexes during several intervals within the first 9 months after surgery when evaluating the KOOS, Lysholm, and Tegner questionnaires. These results indicate a higher subjective knee function of male patients, and this should be taken into account.
In terms of demographics such as age, ethnicity, and graft choice, both groups were comparable. In this study, the mean age at ACL reconstruction was 28 years, and 59.2% were male. The ratio of male to female corresponds to a Scandinavian registry (Danish 60%, Swedish 57.5%, and Norwegian 57.5%) 2,19,29 and a community-based registry in the United States (63.6%). 35
The mean age of patients in the Swedish, Danish, Norwegian, and US registries (25, 30, 27, and 29.5 years, respectively) is comparable with our results (mean ± SD, 28 ± 10 years). We would like to emphasize that when comparing sex differences after ACL reconstruction, age differences could cause bias presuming that younger athletes have a different desire to return to sports compared with relatively older athletes.
When analyzing results from previous studies it appears that the incidence of ACL tears is higher in female patients. However there has been very little published comparing the surgical success between the sexes. 20,25 Barber-Westin et al 9 and Ferrari et al 17 both analyzed objective measurements and subjective assessment of knee symptoms between men and women undergoing ACL reconstructive surgery and showed no statistical or clinical differences in their outcome analysis. These findings are in accordance with our results, although both studies differed from ours in several aspects. Barber-Westin et al 9 and Ferrari et al 17 included patients only with BPTB grafts. Our study included all patients who underwent ACL surgery for outcome score analysis. The main purpose of this study was to evaluate clinical measurements preoperatively and during relatively short intervals after surgery to detect possible differences between the sexes. Barber-Westin et al 9 and Ferrari et al 17 used longer follow-up intervals but included fewer patients in their analyses. An important feature of this study is that the analysis not only included objective measurements such as isokinetic strength, knee laxity, and functional muscle performance but also used subjective evaluation of knee function as measured by the KOOS, Lysholm, and Tegner score. Our aim was to evaluate the outcome scores that are currently used by some orthopaedic surgeons as return-to-sports criteria. To our knowledge, such detailed results from large numbers of measurements performed within the first year after surgery are not described in the present literature. This study presents results regarding the most commonly used measurements after ACL reconstructive surgery; the conclusions can then be used by physical therapists in clinical practices and orthopaedic surgeons when deciding whether the patient can return to sport.
In this study, 94% of reconstructions were performed using an HT autograft. Superior results were found for the HT grafts in clinical functionality during the rehabilitation. According to a recently published Cochrane review by Mohtadi et al, 37 there are no significant differences in static stability measurements, clinical outcome scores, range of motion, and isokinetic strength between BPTB and HT grafts. However, the general incidence of anterior knee symptomatology was significantly greater (rate ratio [RR], 1.45; 95% CI, 1.05-2.01) in the BPTB group. Kneeling discomfort occurrence was also almost 4.5 times greater (RR, 4.46; 95% CI, 2.97-6.69) in the BPTB group, resulting in inferior results compared with HT grafts when evaluating knee-associated symptoms. The same authors reported that patients with HT grafts are less likely to develop anterior knee pain, kneeling pain, and patellofemoral problems during the rehabilitation phase. There are, however, differences between HT and PT grafts in terms of revision rate. Previous studies reported a higher revision rate (>1.8 RR) for HT grafts after adjustment for age, sex, body mass index, and ethnicity. 34,45 A possible cause for this increased risk is the difference in fixation methods and fixation devices that have been introduced for HT grafts that have evolved in the past few years. 45 Future randomized controlled studies should address differences between fixation methods for the graft types to support this hypothesis.
For return-to-sport activities, surgeons mostly rely on static laxity tests 18 ; physical indicators, including the thigh muscle circumference and range of motion; and the thigh muscle peak torque. 54 Lephart et al 28 reported that isokinetic strength tests alone could not appropriately evaluate a patient’s ability to return to sport because peak torque has no direct correlation with functional performance. Barber et al 7 reported that the single-leg hop test and single-leg vertical jump test are more reliable tools than the isokinetic strength measurements for assessing functional recovery after ACL reconstruction. Assessment of return to sports depends on various factors such as muscle strength, neuromuscular control, psychosocial factors, 4,36,52 and knee laxity. 12,18 We believe that all these factors should be measured before allowing the athlete to resume sports activities. We therefore advise physicians to use multiple measurements when deciding to resume sports activities. Barber-Westin and Noyes 8 have suggested the following tests as criteria for returning to sport activities: less than 10% deficit in strength of the quadriceps/hamstrings and in single-leg hop testing (normal LSI score), less than 3-mm difference in AP translation between the reconstructed and healthy knee, no effusion or reactive knee, and a full range of motion. Based on our findings, we support this algorithm for preventing reinjury when deciding to return to unrestricted sports activities in a Dutch population. Besides these physical indicators of recovery, psychosocial aspects are also of significant value to achieve a successful outcome. It is important to understand and address factors such as cognition and behavior, which are related to the rehabilitation process and thus influence the final outcome after ACL reconstruction. 52
Increased knee laxity is suggested to be a risk factor for ACL injury 51 and should be taken into consideration during the evaluation of return to sports. Also, surgical success is often defined by evaluating side-to-side differences in AP knee laxity. 44 The most commonly used threshold for defining arthrometric failure of the reconstructed ACL graft is 3 to 5 mm of side-to-side difference, and this is widely accepted. 44 In the present study, there were no significant differences (P = .903) between sexes in knee laxity during the preoperative measurement. When evaluating the postoperative knee laxity, there were minor differences between men (1.7 ± 2.9 mm) and women (2.0 ± 2.4 mm), indicating a slightly greater AP knee translation in female patients. However, these differences were not significant (P = .680). A recent published systematic review 44 reported that females who undergo ACL reconstruction using hamstring grafts demonstrate increased AP knee laxity over time compared with males undergoing the same procedure. A possible explanation for this difference in comparison with our findings is the relatively short follow-up measurements of this study. Therefore, we strongly suggest the implementation of a national Dutch registry for monitoring the functional outcome of ACL reconstruction with longer follow-up intervals. The risk of sustaining a second ACL injury is highest during the first year after return to sports, 42,43,57 and differences between sexes should be emphasized more in future research for reducing injury incidence. Based on the results of previously published studies, it can be presumed that a nationwide ACL registry is of major value for deciding when to return to sport activities based on clear objective outcome parameters. Large cohorts are valuable for identifying possible risk and prognostic factors for superior functional outcomes after ACL reconstructive surgery.
Limitations
An important limitation of this study is a possible bias due to a large drop out in the follow-up. The patients in our study who were followed in the web-based registry lived in several regions within the Netherlands. A relatively large number of these patients were unable to attend all the follow-up measurements due to demographic considerations. Second, not all measurements were reimbursed by the patient’s health insurance, thus negatively influencing compliance of patients. Therefore, only a limited set of data could be retained and used for analysis. Due to these practical limitations, we focused on reporting descriptive statistics whereas the analyses were mainly exploratory. Another limitation of this study is the relatively short follow-up period compared with other national registries. The Dutch Combined Quality Care ACL registry has follow-ups at 3, 6, 9, and 12 months postoperatively. In Denmark, these follow-ups are done at 1, 5, and 10 years postoperatively. In Norway, they are done at 2, 5, and 10 years postoperatively, and in Sweden, they are done at 1, 2, 5, and 10 years postoperatively. 2 Long-term effects (>1 year) of ACL reconstructive surgery regarding clinical outcomes could therefore not be evaluated and compared with other registries. However, the follow-up of these Scandinavian registries mainly included questionnaires and not objective functional outcomes such as isokinetic strength, knee laxity, and hop tests. Our aim was not only to report on self-reported questionnaires but also to present clinical results of the commonly used objective measurements after ACL reconstruction.
Conclusion
Twelve months after ACL reconstruction surgery, there were no statistically significant differences between men and women in isokinetic muscle strength deficits, knee laxity, and hop test for distance when comparing with the contralateral limb. In addition, no differences were found 12 months after surgery for KOOS, Lysholm, and Tegner scores. However, during the first 9 months after ACL surgery, men showed slightly superior results in the evaluation of isokinetic strength and subjective knee questionnaires. However, the clinical relevance of our findings in relation to function and timing of return to sports after ACL reconstructive surgery requires further investigation.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the ONVZ Dutch health insurance company. The company does not benefit from the presented results and was not involved in the professional judgment of the contributors. Direct financial support (a 15,000 Euro grant) was given as compensation for hours worked by the contributors. This was a one-time grant for performing the analysis and writing the manuscript. The intention of ONVZ for supporting this study was the desire to gain a clear insight into the functional status of a large group of patients after anterior cruciate ligament surgery in a Dutch population.
Acknowledgment
This project was funded by a grant from ONVZ, for which the authors are extremely grateful. The authors thank Combined Quality Care for allowing them to use the data from their database. The authors also thank J.J. Caron, MD; C.H. Geerdink, MD, PhD; T. Sijbesma, MD, PhD; H.M. Schuller, MD, PhD; R. Krips, MD, PhD; E. Raven, MD; and J.A.C. Zijl, MD, who provided data for the registry.