
Abstract
Background:
Female patients tend to suffer a greater risk of reinjury and worse patient-reported outcome measures (PROMs) after anterior cruciate ligament reconstruction (ACLR) than male patients, regardless of the graft type used.
Purpose/Hypothesis:
This study explored the role of donor-recipient sex mismatching to help explain these sex-based disparities in outcomes after ACLR with an allograft. The hypothesis was that allograft donor-recipient sex mismatch would adversely affect surgical outcomes at a 2-year follow-up, with male-to-female graft donations yielding the lowest rates of success.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent primary ACLR with an allograft between 2012 and 2022 were eligible for recruitment. The following PROMs were collected from baseline through a 2-year follow-up: Knee injury and Osteoarthritis Outcome Score subscales, Marx activity rating scale, visual analog scale for pain, and Veterans RAND 12-Item Health Survey. Demographic and graft-specific variables were also collected. Sex-matched cases were compared with sex-mismatched cases and an identical subgroup analysis was performed for female patients only.
Results:
Of the 112 included patients (N = 70 women), 59 (52.7%) were sex mismatched. The mean patient age was 40.7 ± 10.9 years, and the mean body mass index was 26.8 ± 4.7 kg/m2. Most reconstructions (89.3%) used a semitendinosus tendon graft, with a mean implanted graft diameter of 9.7 ± 0.5 mm (quadrupled). Of the mismatched cases, 96.6% involved a male allograft donated to female recipients. Overall, the matched group demonstrated higher PROM scores across all time points compared with the mismatched group, although statistical significance was only reached for the Marx score at baseline (P = .012) and 1 year postoperatively (P = .022). In the female-only subgroup analysis, a larger graft diameter was measured in the mismatched cases (receiving male allografts) compared with the matched female cases (9.7 ± 0.6 vs 9.2 ± 0.4 mm, respectively; P = .002). Moreover, the mismatched cases tended to report better postoperative PROM scores, although this trend was not statistically significant.
Conclusion:
The study findings indicated that male donors provided larger allografts than female donors, and that donor-recipient allograft sex matching did not contribute significantly to ACLR outcomes. Other factors may be more important to outcomes in female patients.
Keywords
The anterior cruciate ligament (ACL) is a commonly injured ligament with an annual incidence of rupture that has been growing over the past 20 years.4,13,36 Consequently, outpatient ACL reconstructions (ACLRs) have seen a corresponding rise in incidence, with 1 recent study 13 reporting a 19% increase in procedures from 2002 to 2014. In 2016, the incidence of isolated ACL tears in the United States was reported at 68.6 per 100,000 person-years with worldwide estimates climbing as high as 78 per 100,000 person-years. 36 When stratified by subgroup, there is an abundance of literature supporting a positive association between an increased risk of ACL rupture and participation in cutting/pivoting sports, increasing levels of athletic competition, and female sex. § Most notably, it is widely recognized2,4,13,15,31,33,35 that the risk of ACL injuries peaks among young female athletes, with female-to-male ACL tear ratios ranging from 3-to-1 to 9-to-1.These injuries pose significant concerns for female athletes because of the physical, psychological, temporal, and financial challenges they face in returning to play after surgery. Moreover, the uneven risk of rerupture, lower self-reported outcomes, and the established association between ACLR and posttraumatic osteoarthritis underscore the importance of identifying specific variables predisposing women to worse postoperative outcomes.7,13,22,29,35,40
The risk factors implicated in the male-female disparity of ACL injuries and ACLR outcomes include intrinsic and extrinsic variables—such as intercondylar notch width, native ACL size, shoe-surface interaction, dynamic knee valgus, and female quadriceps dominance.15,21,22,33,40 In addition, since most ACL tears2,15 (~70%) occur in noncontact settings, significant efforts have been allocated to managing modifiable risk factors, from incorporating neuromuscular training and promoting proper biomechanics2,14-16,28,33,46 to the use of a larger graft size in ACLRs with an allograft. 22 These are compelling elements for surgeons to consider when performing ACLRs on women compared to men; however, they alone have not yet proven to be causative of the observed sex discrepancy in outcomes. This would suggest that there are still more factors to consider.
Other such considerations that have not been well studied are allograft- and donor-related characteristics in ACLR. While graft data—such as size, age, storage methods, sterilization techniques, and tissue type—have proven relevant to ACLR outcomes,5,12,17,19,34,41,42 recent work has explored donor characteristics further in osteochondral allograft (OCA) transplantation. A 2022 study by Merkely et al 27 found that a sex mismatch between OCA donor and recipient had a significantly negative effect on 5-year survivorship of the grafts and surgical outcomes. Importantly, grafts failed more often when a sex mismatch was present (63% vs 92%; P = .02) and outcomes were worse when male donor tissue was transplanted into a female recipient 27 (P < .04). These results correspond with conventional knowledge about the role of donor-recipient sex mismatch in solid organ transplantation as a source of adverse outcomes. Such findings have been reported in lung, heart, pancreas, kidney, and liver transplantation, and there are data to support a similar role of sex mismatch in orthopaedic surgery. 27
While the pathophysiological mechanism through which donor-recipient sex mismatch leads to failures of OCA transplants is not well understood, numerous theories exist. Potential catalysts for an adverse autoimmune reaction in transplantation include histocompatibility disagreement, increased immunologic expression during pregnancy, differing hormonal profiles, and gross anatomic differences. 27 In the case of OCA transplantation, anti-human leukocyte antigen antibodies have also been shown to develop after implantation.9,18,27,39 Ultimately, the nature of the sex disparity in ACLR outcomes is multifactorial and given the evidence demonstrating that a donor-recipient sex mismatch can affect the outcomes of various procedures in transplantation medicine, we believe this may also be relevant to ACL allografts.
This study aimed to explore the potential role of donor-recipient sex mismatching in allografts used for ACLR and to offer descriptive data on the donor allografts used in patients who had ACLR. We hypothesized that the presence of a donor-recipient sex mismatch would adversely affect surgical outcomes at a minimum follow-up of 2 years, with male-to-female graft donations yielding the lowest rates of success.
Methods
Patient Recruitment and Variable Collection
This retrospective study of prospectively collected data was performed after receiving approval for the study protocol from our institutional review board. The hospital information technology-approved and Health Information Portability and Accountability Act–compliant Surgical Outcome System database was used for all electronic consenting and data collection. The Surgical Outcome System database (Arthrex), a global registry database, provided complete preoperative baseline data for all patients who underwent ACLR with our senior author (E.G.M.), a sport-medicine fellowship-trained surgeon, between 2012 and 2022. All patients who had undergone ACLR with an allograft and had a minimum follow-up of 2 years were initially considered eligible for inclusion. Patients were excluded in the case of ACLR revision, combined ligament injuries requiring additional ligament reconstruction, or coronal malalignment of the lower limb (eg, varus or valgus deformity exceeding 3° as assessed by long-leg standing radiographs) that required corrective osteotomy. Subsequently, patients with missing responses on patient-reported outcome measures (PROMs) were also excluded.
Demographic variables collected for each patient included age, sex, body mass index (BMI), limb laterality, presence of concomitant injuries, and concomitant procedures performed. PROMs— including the Knee injury and Osteoarthritis Outcome Score (KOOS) subscales, Marx activity rating scale, visual analog scale (VAS) for pain, and Veterans RAND 12-Item Health Survey (VR-12)—were collected preoperatively and at 1 and 2 years postoperatively.
A total of 175 patients underwent ACLR using allografts during the specified time frame. Of these, 62 were excluded because of incomplete PROMs at either the pre- or postoperative timepoints. Consequently, 112 patients were eligible for analysis (65% follow-up) (Figure 1).

A flowchart of the included patients. ACLR, anterior cruciate ligament reconstruction; PROMs, patient-reported outcome measures.
Graft- and Donor-Specific Variables
The serial number and expiration date of each allograft used in the included ACLRs were collected from patient records and used to obtain all donor- and graft-specific variables, which were provided by our institution’s graft suppliers LifeNet Transplant Services and Joint Restoration Foundation. Graft-specific variables that were collected included tissue type, harvested allograft diameter, harvested allograft length, aseptic preparation, date harvested, and expiration date. The implanted allograft diameter was also recorded in our data collection system. Donor-specific variables included sex, age, race, height, and weight. Other variables, including the medical comorbidities of donors, were unavailable upon request.
Statistical Analysis
While all prospective data collection was completed before this investigation was conceived, an a priori power analysis was performed before its initiation to determine the minimum number of patients required to achieve a power of 80% (G*Power software; Version 3.1.9.6). Using an alpha of .05, the projected sample size needed to detect a moderate effect from donor-recipient sex mismatch was found to be 74 patients (37 per group), considering the minimal clinically important difference for the KOOS subscales of 10 points, 44 with a standard deviation of 15 points. The overall cohort was then separated into 2 groups—same donor-recipient sex versus sex mismatched—and compared.
Continuous variables—such as age, graft length, and graft diameter—were reported using means and standard deviations, while categorical variables—such as sex, race, and aseptic preparation—were reported with frequencies and percentages. A Shapiro-Wilk test was used to assess the normality of the numerical variables. All patients were then stratified into matched (man-to-man, woman-to-woman) and mismatched (man-to-woman, woman-to-man) donor-recipient sex groups; and the groups were compared across demographic characteristics, PROM scores, and graft-specific variables using independent-samples t tests or Mann-Whitney U tests, as indicated. An identical subgroup analysis of only female patients was also performed. Statistical significance was considered as P < .05. SPSS Version 28.0 (IBM Corp) was used to perform all statistical analyses.
Results
Of the 112 patients included in the analysis, 62.5% (N = 70) were women. The mean age of patients was 40.7 ± 10.9 years (range, 16-66 years), with a mean BMI of 26.8 ± 4.7 kg/m2 (range, 19.4-46.5 kg/m2). The mean age of donors was 45.7 ± 10.2 years (range, 14-62 years). Of note, 8 (7.1%) patients were smokers, and 1 (0.9%) had diabetes. When comparing demographic profiles, the mean BMI of the matched group was greater (P = .003) and included more male patients (P < .001) than the mismatched group (Table 1).
Pooled Patient Characteristics Overall and by Study Group a

Data are presented as mean ± SD or n (%) unless otherwise indicated. Bold P values indicate statistically significant differences between the matched and mismatched groups (P < .05). BMI, body mass index.
Pooled Allograft Data
For the original 175 patients who met the inclusion criteria, LifeNet Transplant Services provided data for 170 of the grafts, while the Joint Restoration Foundation provided data for the remaining 5 grafts. Among those from LifeNet, 150 (88.2%) were harvested from male donors, with a mean age of 45.9 ± 9.8 years (range, 14-65 years), a mean height of 5.87 ± 0.3 feet/178.92 ± 9.14 cm (range, 5.08-6.75 feet/154.84−205.74 cm), and a mean weight of 213.1 ± 48.4 pounds/96.66 kg ± 21.95 kg (range, 119-351 pounds/53.98−159.21 kg). Within those 170 tendons, 150 (88.2%) were semitendinosus tendons, 13 (7.6%) anterior tibialis tendons, 4 (2.4%) posterior tibialis tendons, 2 (1.2%) gracilis tendons, and 1 (0.6%) was a bisected patellar tendon. With regard to race, 131 (77.1%) donors identified as White, 32 (18.8%) as Black, 4 (0.02%) as Hispanic, and 3 (1.8%) as other. All allografts were terminally sterilized using low-dose gamma irradiation. Among the grafts provided by the Joint Restoration Foundation, all 5 were a semitendinosus tendon harvested from male donors, with a mean age of 54.2 ± 2.8 years (range, 51-57 years). Height, weight, race, and sterilization techniques were not provided for these grafts.
Implanted Allografts in the Final Patient Cohort
In the final cohort (N = 112), most reconstructions used a semitendinosus tendon allograft (100; 89.3%), while the remaining 11 (9.8%) used a posterior tibial tendon allograft. This relationship did not change from the matched to the mismatch groups. Among those implanted, the harvested allograft diameter was 6.8 ± 0.7 mm; the harvested allograft diameter was significantly larger in male donors (6.9 ± 0.7 mm) compared with female donors (6.6 ± 0.7 mm) (P < .026). The harvested allograft length was 279.5 ± 16.7 mm (range, 240-330 mm) and did not vary significantly between male (280.2 ± 16.0 mm) and female (270 ± 18.1 mm) donors. The mean implanted (quadrupled) graft diameter was 9.7 ± 0.5 mm (range, 9-11 mm), and there were no significant differences in the size used for donor-recipient sex-matched versus mismatched patients (9.6 ± 0.5 vs 9.7 ± 0.4 mm, respectively; P = .166). The mean time to implant (harvest date to surgical date) was 263 days. Overall, 59 (52.7%) cases included donor-recipient allograft sex mismatch, 57 (96.6%) of which involved a male allograft donated to female recipients. Only 2 cases (3.4%) involved a female donor to a male recipient. A summary of donor allograft characteristics is found in Table 2.
Allograft Characteristics Before Surgery a

Data are presented as mean ± SD. The bold P value indicates a statistically significant difference between sexes (P < .05).
Women-Only Subgroup Analysis
The subgroup analysis captured 70 female patients with a mean age of 42.3 ± 11.7 years (range, 16-66 years) and a mean BMI of 25.7 ± 4.3 kg/m2 (range, 19.4-37.7 kg/m2). Among the female patients, 2 (2.9%) smoked, and none had diabetes. As in the pooled cohort, the demographic profiles of matched versus mismatched patients were similar. Most reconstructions again used a semitendinosus tendon allograft (63; 90%), while the remaining 7 (10%) used a posterior tibial tendon allograft. This relationship did not change from the matched to the mismatched groups. Most cases in this cohort involved a donor-recipient allograft sex mismatch (57; 81.4%), and the mean implanted (quadrupled) graft diameter was 9.7 ± 0.5 mm (range, 9-10 mm), which was significantly larger in the mismatched group versus the matched group (9.2 ± 0.4 vs 9.7 ± 0.6 mm; P = .002). The patient and graft characteristics are summarized in Table 3.
Patient and Graft Characteristics for the Women-Only Cohort a
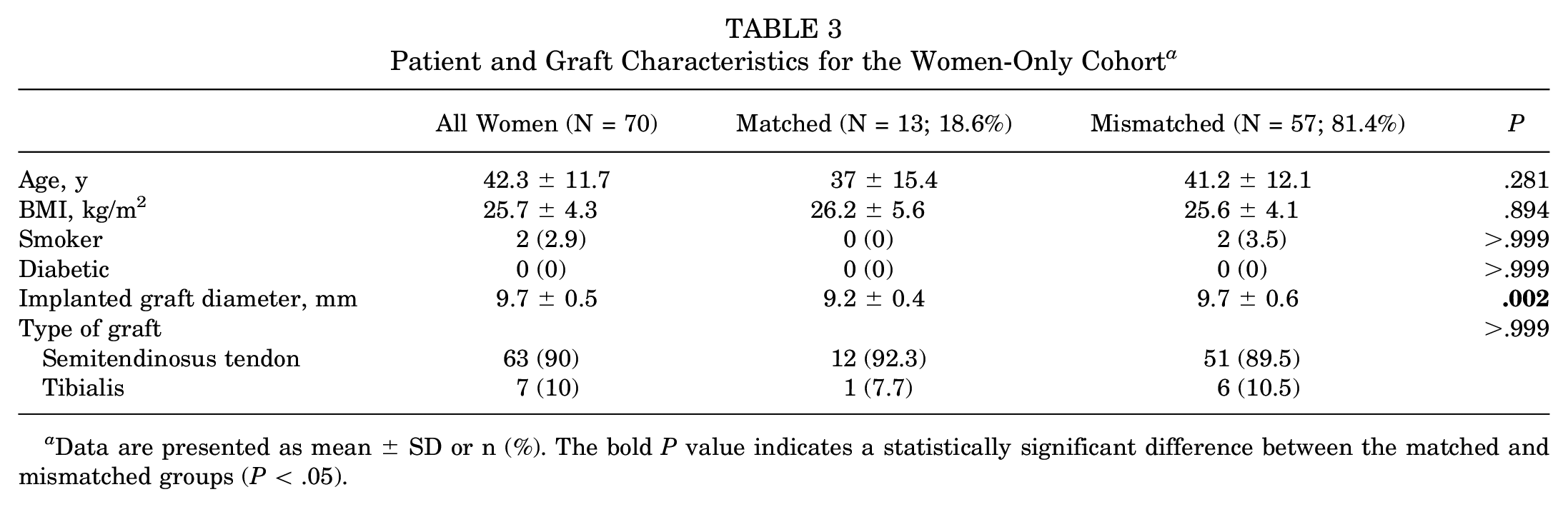
Data are presented as mean ± SD or n (%). The bold P value indicates a statistically significant difference between the matched and mismatched groups (P < .05).
Patient-Reported Outcome Measures
Compared with the mismatched group, the Marx score was significantly higher in the matched group at baseline (P = .012) and at 1-year postoperatively (P = .022). PROM scores overall also tended to be better at all time points in the matched group, but not significantly (Figure 2 and Table 4). No other statistically significant differences were noted through 2 years postoperative. In the female-only subgroup analysis, those who received male allografts (mismatched) tended to have better postoperative PROM scores, but without statistical significance (Table 5). Interestingly, this was also the group whose implanted allograft diameter was larger on average.
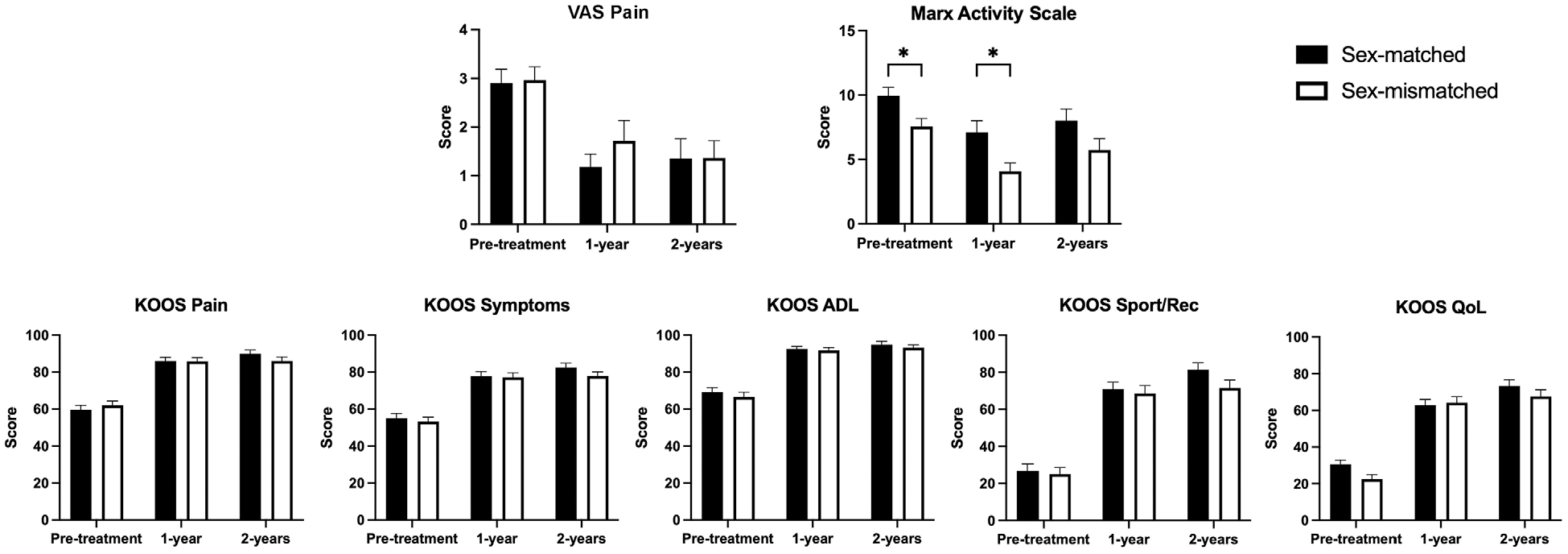
Visual representation of PROM scores between the matched and mismatched groups. *Significantly better Marx scores were seen in the matched group versus the mismatched group at baseline and 1 year postoperatively. ADL, activities of daily living; KOOS, Knee injury and Osteoarthritis Outcome Score; PROM, patient-reported outcome measure; QoL, quality of life; Rec, recreation; VAS, visual analog scale.
Results of PROM Overall and by Study Group a

Data are presented as mean ± SD or n (%). Bold P values indicate statistically significant differences between the matched and mismatched groups (P < .05). ADL, activities of daily living; KOOS, Knee injury and Osteoarthritis Outcome Score; postop, postoperative; preop, preoperative; PROM, patient-reported outcome measure; QoL, quality of life; Rec, recreation; VAS, visual analog scale; VR, Veterans RAND.
Results of PROM for the Women-Only Cohort a

Data are presented as mean ± SD or n (%). The bold P value indicates a statistically significant difference between the matched and mismatched groups (P < .05). ADL, activities of daily living; KOOS, Knee injury and Osteoarthritis Outcome Score; postop, postoperative; preop, preoperative; PROM, patient-reported outcome measure; QoL, quality of life; Rec, recreation; VAS, visual analog scale; VR, Veterans RAND.
Complications
Two episodes of graft failure (1.8%) occurred during the follow-up period. Furthermore, 3 cases of arthrofibrosis were reported, with 2 of them necessitating arthroscopic debridement for scar tissue lysis.
Discussion
The primary findings of this study demonstrated that donor-recipient sex matching of allografts in ACLR did not significantly affect surgical outcomes over a 2-year interval. While mean Marx scores were greater at baseline and at 1 year postoperatively in the sex-matched group (P < .05 for both), there were no statistically significant differences on any other PROMs between the matched and mismatched cohorts. In contrast, results of the women-only subgroup analysis demonstrated that the mismatched group who received male allografts had generally better PROM scores postoperatively, although the difference was not statistically significant. Despite previous studies in transplant medicine identifying poorer outcomes in donor-recipient sex mismatched cases27,32,37,45 this investigation demonstrated that sex mismatching of allografts in ACLR did not significantly affect the surgical outcomes of male or female patients when compared with sex matching, thereby contradicting our initial hypothesis that a difference would manifest.
In contrast to a recent study demonstrating inferior outcomes in sex-mismatched OCA transplant cases, 27 the results of this analysis have shown this not to be the case for allografts in ACLR using allografts. Not only did 4 out of the 5 included PROMs fail to demonstrate a significant difference in the matched versus mismatched groups, but the 2 significant observations that did manifest in the Marx scores of the pooled cohort did not remain at 2 years postoperatively. This may have been the result of a baseline difference persisting through the 1-year postoperative mark until progress made through individual healing and physical rehabilitation leveled out across patients at 2 years postoperatively. In addition, the Marx is scored on a 5-point Likert scale (range, 0-4, with 4 being the highest) and assesses only 4 items—running, cutting, deceleration, and pivoting. 25 Therefore, a 1-point difference equates to a 20% change in score and could explain why Marx was more likely to produce a significant difference compared with other multidimensional PROMs that were used, such as the 42-item KOOS subscales.
Meanwhile, in the analysis of female patients, most of the cases involved a donor-recipient sex mismatch. Our allografts were ordered based on diameter size and length supported by previous evidence, demonstrating that an increased hamstring tendon autograft size results in improved PROMs and lower revision rates in primary ACLR,6,8,23,24,30 with 1 study finding a 0.82 times lower likelihood of revision with every 0.5-mm incremental increase in graft diameter from 7 to 9 mm. 38 Upon examination of the grafts we received, most that met this criterion were harvested from male donors (155/175; 88.6%), which helps to explain the high rate of mismatch in women. This analysis demonstrated that in the mismatched (man-to-woman) cases, a significantly larger graft diameter was used compared with grafts in the matched female (woman-to-woman) cases. In other words, the female patients who received male allografts received a significantly more robust graft on average (9.2 vs 9.7 mm; P = .002). Furthermore, the mismatched female cases involving the implantation of a larger male allograft yielded generally better PROM scores postoperatively, which is consistent with the literature on hamstring tendon autograft size presented above. While this result did not achieve statistical significance, it was an unexpected contrast to the outcomes of the pooled cohort, in which the matched cases demonstrated generally better PROM scores. In addition, this finding is noteworthy because it suggests that despite uniform quadrupling, a male graft origin offered a more robust final graft diameter compared with a graft of a female origin. Of note, donor sex has been shown to have minimal effect on the biomechanical properties of graft tissue; thus, a difference in tissue quality is unlikely to have contributed to the observed outcome. 1 Therefore, when considered in the context that a larger graft diameter confers better surgical outcomes after ACLR, ostensibly due to increased tensile strength against shearing forces,3,6,8,11,23,24,38 this size difference could have played a role in the superior outcomes of the mismatched female cases. While previous studies have found significant benefits to using ACL grafts ≥8 versus <8 mm,3,8,23,24,30,38 these results suggest that diameter differences are still relevant at ≥9 mm. Further research should continue to elucidate what the minimum threshold for ACL allograft diameter is or if it is instead a continuous variable between 2 endpoints.
Ultimately, the lack of a difference in ACLR outcomes due to sex mismatch is reassuring and indicates that ACL allografts, regardless of donor sex, continue to be a safe option for patients. While the results of our women-only subgroup analysis reinforced that graft diameter has an important role in ACLR outcomes of women, it is more important to note that a disparity between male and female ACLR patients still exists and that there are still undiscovered factors contributing to this disparity. It is therefore crucial for knee surgeons to be aware of the current differences in female versus male ACLR outcomes to improve care and rehabilitation strategies. Being mindful of the functional and anatomical differences between male and female knees (smaller intercondylar notch width, smaller native ACL size, increased Q angle, quadriceps dominance, and increased tibial slope in women)15,21,22,33,40 is also key to achieving optimal ACLR technique. While this investigation has taken a novel approach to an ongoing issue, future research—including in vivo motion analysis, immunogenicity in graft healing, and allograft size thresholds—should seek to identify other potential risk factors for ACL tears and retears in women. For now, allografts should continue to be used in ACLR regardless of donor sex as part of the current standard of care.
Limitations
This study is not without limitations. Our analysis takes a unique approach to the current disparity in male versus female ACLR outcomes by investigating the effects of donor-recipient sex mismatch and provides useful allograft data supplied by 2 major tissue donation services. While these data are limited by the scope of our single-site investigation and the inherent selection bias of our graft orders, we believe this information is generalizable to a broader audience of orthopaedic surgeons and institutions. Second, this study design was limited to a 2-year follow-up and would have benefited from additional data about graft donor comorbidities, which were unavailable upon request. While the effects of tissue sex have been shown to be of little consequence to an ACL graft’s biomechanical properties, medical comorbidities could potentially introduce random variation to graft performance. From the information provided, however, we were able to obtain smoking and diabetic statuses, which were both low in the donor population. Another notable limitation of our study is the relatively high number of patients (35%) excluded from the analysis due to incomplete PROMs data, primarily resulting from loss to follow-up or incomplete data collection. We acknowledge that this may introduce potential bias to the reported results. Finally, this study did not include a discussion of the role of immunogenicity in outcomes. For example, the robust immunogenicity of histocompatibility antigen H-Y in men has been implicated in the development of more robust immune responses and has been shown to affect tissue transplantation outcomes. 27 However, this discussion is more relevant to fresh tissue donation and likely of little consequence to the frozen cadaveric allografts used for ACLR. Furthermore, the processing of allografts from cadaveric donors involves several steps while serologic tests are conducted, culminating in freezing. While frozen grafts can remain viable for years, cells do not survive this process, potentially reducing the immune responses, including major or minor histocompatibility complex antigen expression.
Conclusion
ACLR with an allograft continues to be a safe and reliable procedure in older and less active patients. The study findings indicated that male donors allow for the preparation of larger allografts than female donors and that donor-recipient allograft sex matching does not significantly contribute to ACLR outcomes. Other factors may be more important to outcomes in female patients and should continue to be studied.
Footnotes
Final revision submitted June 11, 2024; accepted July 17, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.L. has received consulting fees from Anika Therapeutics, Vericel, and Flexion Therapeutics; nonconsulting fees from Vericel, Aesculap Biologics, and Arthrosurface; and honoraria from JRF Ortho. E.G.M. has received education payments and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mass General Brigham (reference No. 2011P002663).