
Abstract
Background:
Knee injuries account for approximately one third of injuries in skiers. Researchers have proposed several mechanisms of knee injury in skiers. However, the frequencies of these mechanisms have varied in different studies.
Purpose:
To identify the most common knee injury mechanisms in recreational downhill skiers and to assess injury frequencies across several demographics.
Study Design:
Descriptive epidemiology study.
Methods:
Over 6 ski seasons, 541 patients with acute knee injuries completed a survey. Patients selected 1 of 6 injury classifications; age, sex, height, weight, years of experience, ability level, and ski binding release were also recorded.
Results:
The overall injury distribution was valgus–external rotation (32.9%), phantom foot (22.5%), hyperextension (19.0%), boot induced (7.8%), collision (2.2%), and other (15.6%). The phantom foot mechanism was most common in ages 30 to 40 years (36.3% of all injuries within this mechanism; P < .01). Children and adults showed no significant difference in distribution of injury mechanism. Of 80 youth skiers, valgus–external rotation was most common (35.4%), followed by phantom foot (25.3%). Adult and youth skiers who identified as “advanced” skiers had a higher prevalence of valgus–external rotation than did less experienced skiers (51.5% of total valgus injuries; P < .01). Bindings released in 19.3% in adults and 53.7% in youths (P < .01) during injury. Female skiers comprised 60.0% of total respondents, but only 39.7% of injuries occurred in female children (P < .01).
Conclusion:
Valgus–external rotation is the most common injury mechanism for recreational skiers in general. Previous studies have suggested that the phantom foot injury is the most common injury, but in this series, it was the second most common, representing 22.5% of injuries in this study. Individuals between the ages of 30 and 40 years showed an increased risk for the phantom foot mechanism, and the prevalence of injuries was significantly higher for females compared with males in this cohort (P < .01). Children and adults appear to have similar mechanisms for ski-related knee injuries, with valgus–external rotation being most common and advanced skiers having the highest frequency of this mechanism. Binding release was more likely to occur in youth skiers.
Over the past 40 years, there have been significant changes in ski boots, binding systems, and ski shapes. 5 During this time frame, there has been a reduction in the rates of ankle sprains and tibia fractures. While these injuries have decreased, the rates of serious knee ligament sprains and other knee injuries have increased. 9,16,17 In addition, there have been reports that have shown a decrease in anterior cruciate ligament (ACL) tears in skiers due to carving skis becoming more popular. 22 Knee injuries are common in both recreational and professional skiers; however, the rate of mechanism of injury varies. 2,4,9,12,14,19 A recent study by Rust et al 27 found that the 2 most common injuries in skiers were ACL tears and, in general, other knee sprain.
Previous research has identified 6 common mechanisms that can occur in recreational and professional skiers, including boot-induced anterior drawer, 9,10,12,28 flexion–internal rotation (phantom foot), 6,9,12,28,32 backward fall (similar to phantom foot), 6,7,31,34 valgus–external rotation, 12,25,32 isolated ACL/hyperextension–internal rotation, 6,31 and outside edge catch. 23 Other mechanisms of injury have been recently described by Bere et al 2 based on video analysis of high-speed knee injuries in World Cup ski racers. This analysis identified 3 mechanisms of ACL injury in this elite group: slip catch, landing back-weighted, and dynamic snowplow.
Injuries that occur in professional ski racers may be secondary to different biomechanical patterns because of higher speed, greater fitness level, different terrain, and specialized equipment. As most injuries in the skiing population occur in recreational skiers, research in this area may be valuable to identify common injury patterns and look for opportunities to reduce the risk of injury. The purpose of this study was to identify the most common knee injury patterns in a survey of injured recreational skiers and to compare these knee injury patterns across several demographics such as age, skiing ability, and sex. This survey was based on mechanisms of knee injury that have previously been reported in this skier population. 13,15,23
Materials and Methods
Institutional review board (IRB) approval for the study was obtained. A 10-item questionnaire was developed for the purpose of identifying the mechanisms of injury in recreational skiers. The surveys were given to the skiers under 2 circumstances: by the ski patrollers who evaluated the injured skier on the ski hill or when a patient was seen in an orthopaedic clinic and evaluated for a knee injury related to skiing that season.
In addition to basic demographic information, skiers were asked to classify their skill level. The skill levels were as follows: type I (ski conservatively: skier can ski only on well-maintained, easy or moderate slopes), type II (ski moderately: skier can control skis on properly conditioned slopes and has difficulty maintaining skis on a variety of terrains), or type III (ski aggressively: skier can control skis on any slope under any condition).
Four knee injury mechanisms were identified through a search of the published literature on knee injury in recreational skiers.
Valgus–External Rotation Mechanism
Valgus–external rotation 6,13,19,21,23,31 (Figure 1) has been reported in some studies as the most common injury among recreational skiers. 25,26,30 It begins with the skier losing his or her balance, with the center of gravity shifting forward over the knees. In this position, the inside edge of the ski tip is in contact with the ground. This contact causes an immediate abduction and external rotation of the tibia. The affected leg’s progress slows as the rest of the body is carried forward by the skier’s momentum, creating a valgus force about the knee. This may cause injury to the medial collateral ligament (MCL) and sometimes the ACL. 19,23 The ski acts as a lever arm, maximizing the external torque on the joint, a common theme in alpine ski injuries. Poor skiing technique has been cited as a common cause of this mechanism, 21 and it has been speculated that more effective bindings could prevent this type of injury 8,14,18,23 ; however, the connection between injury and ski bindings requires further investigation.
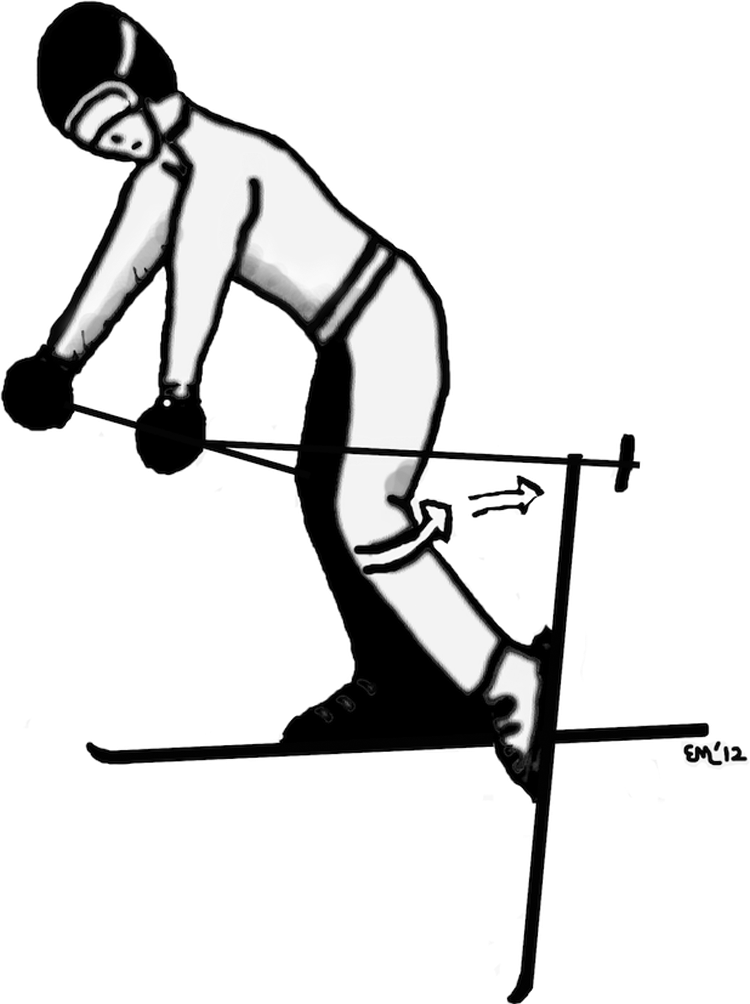
Valgus–external rotation: Forward fall with the inner edge of ski tip catching on snow.
Hyperextension or Hyperextension With Internal Rotation
Hyperextension–internal rotation 6,21,23,31 (Figure 2) commonly occurs in heavy snow. These conditions cause a sudden arrest of ski motion, causing the lower legs to remain stationary while the upper body continues forward progress. This mechanism is often accentuated by an unexpected crossing of the ski tips, creating an internal rotation and varus force on the knee. The result is generally injury to the ACL and sometimes damage to the lateral structures of the knee as well. 23

Hyperextension–internal rotation: Skis turn inward into snowplow position.
Boot-induced Mechanism
The boot-induced mechanism 6,9,10,12,13,19,21,23,24,28 (Figure 3) is unique from deceleration/change in direction injuries, both in mechanism as well as consequential injuries. 12 After a skier loses contact with the ground with both skis, such as while going off of a jump, the ski tails are often the first portions of the skis to contact the snow on landing. This causes a sudden shift of body weight backward, while the lower legs are bound to the skis. As the skier completes the landing, the ski tips are forced down, allowing the rear of the boot to apply an anterior force on the tibia. The anteriorly directed force on the tibia from the back of the ski boot is accentuated by an anterior pull on the proximal tibia by the quadriceps muscles, which is usually strongly activated to prevent the skier from falling backward. This creates a scenario in which the upper body is shifting backward and the lower leg is being forced anteriorly by the lever arm of the ski tail, isolating the ACL for injury. Because there is generally no valgus force involved, the MCL and lateral structures are usually left unharmed, unless additional damage is sustained in the ensuing fall. 6,24

Boot induced: Landing from a jump, the ski tail contacts the snow first.
Phantom Foot Mechanism
Phantom foot mechanism 6,12,13,19,23,24,28,31,32 (Figure 4), also referred to as flexion–internal rotation, has also been reported as the most common injury among recreational skiers. 19,23,31 It occurs when the skier loses his or her balance backward, causing him or her to “sit back” on the rear portion of the skis, placing the hips below the knees. The skier’s weight is shifted off of the uphill ski and placed on the downhill ski. The downhill ski internally rotates the hyperflexed knee. The downhill ski becomes fixed in the snow while the rest of the body continues forward, causing the other ski to accelerate along its inside edge. If the bindings do not release then a damaging force ensues. 13,19,23,24,31 This is another equipment-related injury, being amplified by boot rigidity and dependent on ski binding release. 13,24 Because of the valgus force as well as the internal rotation that can occur, this mechanism has the potential for damage to both the ACL and MCL. 24 Forceful contraction of the quadriceps on losing balance backward can also amplify the mechanism’s damaging effects. 21 Because of its similarity to the proposed “backward fall mechanism,” for the purposes of our study, the 2 mechanisms were combined into 1 injury category.

Phantom foot: Weight shifts backward placing the hips below the knees.
Previous research suggests that the “traditional skis” resulted in the most common mechanism to be a backward twisting fall (phantom foot). 9 Falling backward was one of the mechanisms in World Cup skiers. 2
Study Subjects
The survey used in this study collected information on the subject’s basic demographic information, ability level/experience, equipment type, and injury. Among other demographics, patient age was collected, and for the purpose of this study, we define “youth” skiers as being younger than 18 years. Because the study population was recreational alpine skiers, the mechanisms of injury on our survey were the mechanisms that have been identified as most common among this population. 13 The knee injury survey was given to consenting skiers that suffered a knee injury while skiing at 1 of the 4 participating ski resorts. The survey was administered either immediately at the time of injury under the supervision of trained ski patrol volunteers or by an orthopaedic clinician shortly after or during a clinic evaluation. Because of the guidelines of the IRB-approved protocol, we were unable to collect any clinical diagnostic information about the subjects.
Subjects were not included in the study if they did not have a knee injury or if their knee injury did not occur while participating in recreational alpine skiing. Individuals participating in Telemark skiing, snowboarding, or other snow sports were excluded.
Differences in frequencies were evaluated with P values obtained from analysis with the chi-square function. P < .05 was considered statistically significant.
Results
Over 6 ski seasons, a total of 542 patients with acute knee injuries completed the survey. Of responders, there were 459 adults and 79 youth skiers. The injury distribution patterns were valgus–external rotation (32.9%), phantom foot (22.5%), hyperextension (19.0%), boot induced (7.8%), collision (2.2%), and other/unsure (15.6%). The phantom foot mechanism proved to be more common in skiers aged 30 to 40 years (36.3% of all injuries) compared with the other age groups (20.7% of injuries in those aged 40-50 years; P < .01) (Table 1). For all skiers, self-identified type III skiers had a higher percentage of valgus–external rotation (51.5% of total valgus injuries) than did type I or II skiers (35.7% in type II skiers; P < .01) (Table 2). Female skiers comprised 60.0% of all respondents (Table 3). Binding release occurred in 23.8% of all skiers.
Injury Mechanism Distribution by Age a

a Values are expressed as n (%).
Injury Mechanism Distribution by Perceived Ability Level a
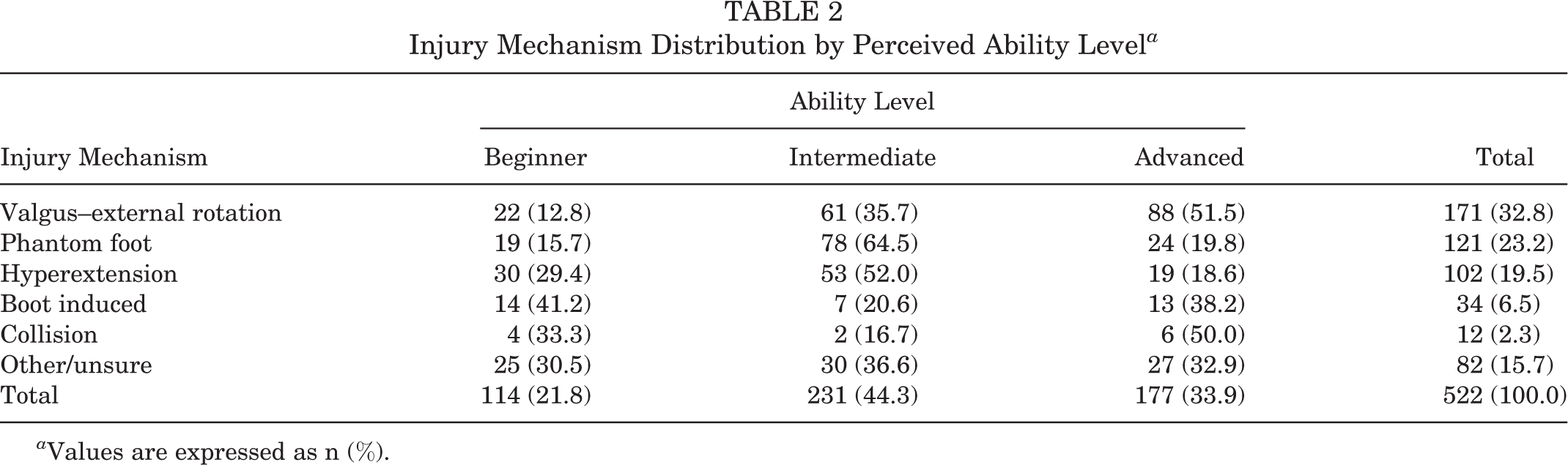
a Values are expressed as n (%).
Injury Mechanism Distribution by Sex a

a Values are expressed as n (%).
The relative injury distribution among children was similar to that of adult patients (Figure 5). Valgus–external rotation was the most common injury mechanism (35.4%), followed by phantom foot (25.3%), hyperextension (19.0%), boot induced (3.8%), and other/unsure (16.5%). There was no statistically significant difference among the different injury mechanisms between adults and children.

Injury mechanism distribution of children versus adults.
Of the 88 youth skiers, 39.7% were female and 60.3% were male. For the adult skiers, 60.0% of those with knee injuries were female and 40.0% were male. Binding release occurred in 19.3% of adults and 53.7% of youth skiers (P < .01).
Discussion
The prevalence of 4 common knee injury mechanisms was studied in injured skiers, with the addition of 2 mechanisms (collision and other), over 6 years at 4 Western ski resorts. The valgus–external rotation and phantom foot mechanisms were found to be the first and second most common, respectively, among both injured adult and youth skiers surveyed. The overall distribution of knee injury patterns was very similar in both adult and youth skiers. The youth skiers had a higher rate of ski binding release than adult skiers.
In recreational skiers, the most common injury pattern has been reported as the phantom foot mechanism. 6,19,23,31 Ettlinger et al 9 proposed that the phantom foot mechanism was the most common injury pattern in recreational skiers based on a video survey of approximately 13 subjects. Other researchers have found that the valgus–external rotation mechanism is most often responsible for knee injuries among recreational skiers. 25,26,30 The boot-induced mechanism may be a common cause of injury when a skier lands on the tails of the skis following a jump. 11,21,23 This mechanism is generally not the most frequently reported in recreational downhill skiers, 13 and this observation was confirmed in our study. While studies have reached different conclusions about the most common pattern of skier knee injury, the 2 most reported are the valgus–external rotation and the phantom foot mechanisms, a conclusion confirmed by our data. It should be noted that unlike similar studies, our survey was self-reported by the patients based on the injury descriptions provided.
Previous research has also identified populations that are more at risk of injury to their knee when skiing. Jarvinen et al 13 reported that female patients accounted for 74% of ACL and MCL ruptures. Although our study is limited because of a lack of denominators, more female patients reported knee injury than did males in this study.
Our study found that skier bindings released in only 24.6% of all injuries. In comparison with competitive skiers, Bere et al 2 reviewed video footage of 20 crashes of World Cup alpine ski racers. In 17 of the 20 crashes reviewed, the bindings did not release. In the 3 cases where bindings did release, this release was determined to occur after the identified crash. Releasable ski bindings have been designed based on DIN settings that consider height, weight, ski boot sole length, the skiing style of the skier (cautious, average, or aggressive), and age. These DIN settings emerged in an era when the main focus was on preventing ankle and tibia fractures rather than knee injuries. 15,29 A better understanding of the distribution of knee injuries in recreational skiers may provide information that could be used to improve binding release mechanisms and release settings that may reduce the risk of knee injury. 1,33 For example, the high frequency of knee injuries that occur when the center of gravity is behind the bindings supports the idea that further design work is needed for upward and diagonally releasing toe pieces of the bindings. Similarly, it is possible that the frequency of knee injuries that occur when the center of gravity shifts forward to the side of the bindings could be reduced with the development of more heel pieces with multidirectional release (eg, upward and laterally). Educational efforts to teach recreational skiers how to avoid vulnerable positions for the knee should take into account the skier’s age, sex, and ability level, as these all have an influence on injury mechanism.
Recent research on elite-level skiers using video analysis has provided some insight into mechanisms of injury. 2,3 Because of the high speeds and aggressive turning maneuvers, elite-level skiers sustain most of their injuries during skiing rather than during falls or accidents. 2 Bere et al 2 showed that the most common injury to ski racers occurred while turning in the “slip-catch” mechanism. This involves the skier losing balance/control and having the outer edge of the ski catch the snow, causing knee flexion, inward rotation, and valgus. The second most common injury was landing from a jump, with the skier losing balance toward the back and landing on the ski tails. This produced tibiofemoral compression and anterior translation of the tibia relative to the femur. The last type of injury identified was the “dynamic snowplow” in which the inner ski rolls to the inside edge, forcing the knee into valgus and inward rotation.
This study has several limitations. The survey did not collect identifiable information as outlined by the IRB-approved protocol, and thus, follow-up information was not obtained. Information on the type of injury sustained based on clinical and magnetic resonance imaging information would be valuable and may be a focus of future research. More adult skiers with knee injuries were surveyed than children or adolescents. This could be because of adults being more willing to complete the survey or because there are simply more adult skiers with knee injuries at the resorts. Studies that conduct retrospective surveys in general can produce participant recall bias, although the time interval between the injury event and collection of the data on the event was short. Krosshaug et al 20 reported that predefined mechanisms might mislead the athlete. Individual subjects may also have difficulties accurately describing the mechanism of injury. Qualitative video analysis could eliminate this potential bias, and future research could be done in this area. Video data are readily available on elite-level skiers based on multiple camera use for broadcast purposes. 2 However, collecting video data on recreational skiers may be challenging because of the lack of video equipment readily available for the recreational skier population. It was not possible to conduct surveys on all skiers at the resorts who sustained knee injuries, as some individuals do not present to ski patrol or our clinics. Finally, it was not possible to collect denominator data with numbers and demographic information on all skiers at the resorts.
An improved understanding of the most common injury mechanisms in recreational and elite skiers could provide a basis for future research to model knee injury. This study found the distribution of injury mechanisms comparable between both adult and youth skiers, despite differences in size and possibly technique. Despite similar injury mechanism distributions, the pattern of binding release was different between adults and children. Further studies in which clinical diagnoses are correlated with the injury mechanism could provide biomechanical insight into these injury patterns. Future research into binding design may consider these biomechanical patterns to reduce the risk of injury.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.