
Abstract
Background:
Tumor-like distal femoral cortical irregularities (DFCIs) are a frequent incidental finding on knee magnetic resonance imaging (MRI) and are common in young competitive athletes.
Purpose:
To assess and compare the morphology and prevalence of DFCIs in competitive alpine skiers over 48 months during adolescence.
Study Design:
Case series; Level of evidence, 4.
Methods:
Adolescent competitive alpine skiers were prospectively recruited in 2018 and received bilateral 3-T MRI of the knee at baseline and after 48 months. All MRIs were evaluated for the presence and location of DFCIs, which were marked at 1 of 3 anatomic positions: (1) the femoral attachment of the medial head of the gastrocnemius muscle, (2) the lateral head of the gastrocnemius muscle, or (3) the attachment of the adductor magnus aponeurosis. The size of the DFCI was measured by 2 radiologists independently. The measurements were compared using the Wilcoxon signed-rank test, the interclass correlation coefficient (ICC), and Cohen Kappa.
Results:
A total of 63 athletes (mean age at follow-up, 19.6 ± 1.2 years; n = 25 female) were included in the study. At baseline, DFCIs were detected in 84 out of 126 knees (67%). At the 48-month follow-up, DFCIs were found in 88 out of 126 knees (70%), with multiple DFCIs in 3 knees and no significant difference between male and female patients (n = 24 male, n = 19 female; P = .71). No significant increase was detected for the number (P = .21) and size of the DFCIs between the baseline and the 48-month follow-up (mean size: baseline, 3.7 ± 0.8 mm; 48-month follow-up: 3.6 ± 0.9 mm; P = .66). The interrater agreement for the mean size measurements of DFCIs was good to excellent (ICC 0.88).
Conclusion:
DFCIs remain a frequent finding on knee MRI in competitive alpine skiers after skeletal maturation and do not disappear during adolescence. The DFCI size was constant in athletes aged between 15 and 19 years. Moreover, DFCIs should not be mistaken for a pathologic finding.
Distal femoral cortical irregularities (DFCIs) are benign fibro-osseous lesions frequently found on radiographs, computed tomography, or magnetic resonance imaging (MRI). 4 They are characterized by a cystic lesion with surrounding sclerosis on the cortical bone surface, most often found at the attachment site of the medial head of the gastrocnemius muscle (MHG) or the lateral head of the gastrocnemius muscle (LHG) as well as the attachment site of the adductor magnus (AM) aponeurosis. 11 The cause of DFCIs is not well understood; nonetheless, it has been suggested that they develop as secondary reactions to repetitive traction injuries or abnormal biomechanical stress (tug lesions).11,13,21 In the literature, several interchangeable descriptions have been used for DFCIs— including cortical desmoid, periosteal desmoid, nonossifying fibroma, and avulsive cortical irregularity.3,8,13 An important distinction should be made between DFCIs and the entities of desmoid tumors or aggressive fibromatosis, which are aggressive neoplasms with a tendency toward local recurrence.2,18,22
Previous studies have described DFCIs as mostly self-limiting lesions that disappear during the end of adolescence and do not require special treatment. However, these results were primarily based on case reports and small cohorts.4,8,11-13 No established therapeutic guidelines have been published to date. 13 Although often asymptomatic, DFCIs may be associated with knee pain or instability; especially in athletes and those with high physical demands, the reported prevalence ranges between 3.6% in the general population and 58% in competitive athletes.1,17 In recent case reports, nonoperative management—including rest, physical therapy, and anti-inflammatory medications—has been proposed. 20 Mester et al 12 recently observed that DFCIs are clinically relevant and may cause activity-limiting knee pain, predominantly in patients with high physical activity. They further noted that structured physical therapy led to significant pain relief, but the rate of complete remission after 12 months was low. However, the reported cohort was relatively small (n = 23), with an inhomogeneous age distribution (8-21 years), and no morphologic correlation of the DFCIs was performed. To date, no longitudinal observations of DFCI in high-risk groups such as competitive athletes have been performed. Therefore, this study aimed to assess whether DFCIs in adolescent competitive alpine skiers remain constant or resolve over 48 months.
Methods
Participant Selection
For this prospective study, adolescent competitive alpine skiers who participated in a certified regional performance center with >5 training units per week and >8 consecutive years of participation in competitive alpine sports were recruited between November 2018 and February 2019 (n = 108)
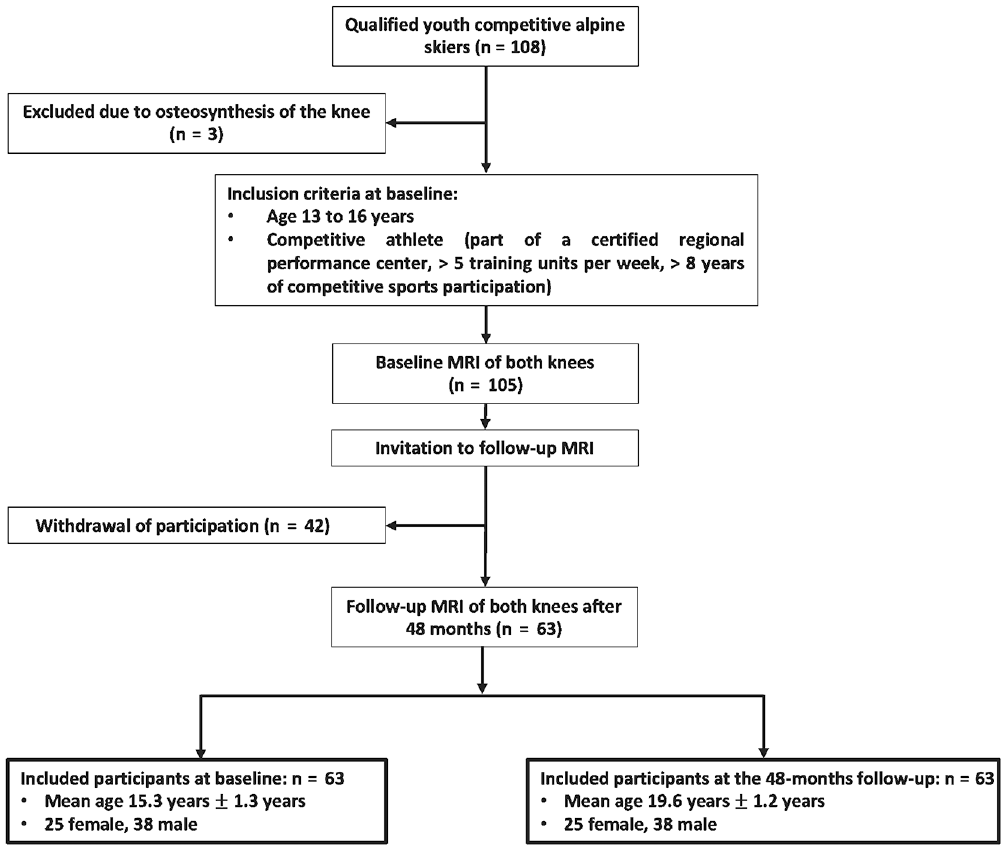
Patient selection flowchart. A bilateral knee MRI was performed for all participants. MRI, magnetic resonance imaging.
Before inclusion, written informed consent was obtained from all study participants or their legal guardians. The analyzed participants were part of a large observational sports medicine study focused on injury prevention in competitive alpine skiers. The study was approved by our institutional review board (Cantonal Ethics Committee Zurich).
Magnetic Resonance Imaging
Bilateral knee MRI was performed at baseline and the follow-up using a 3-T MRI scanner (MAGNETOM Prisma; Siemens Healthcare) with a dedicated 15-channel knee coil (Tx/Rx 15-Channel Knee Coil; Siemens Healthcare). An unenhanced isotropic fat-suppressed T2-weighted 3-dimensional sequence was used for acquisition at both time points. Scan parameters were set as follows: repetition time, 1000 msec; echo time, 108 msec; parallel imaging acceleration factor, 4; acquired slice thickness, 0.63 mm; field of view, 160 × 160; matrix, 256 × 256; receiver bandwidth; and 415 Hz per pixel, which led to an acquisition time of 4 minutes 42 seconds. 17
Image Analysis
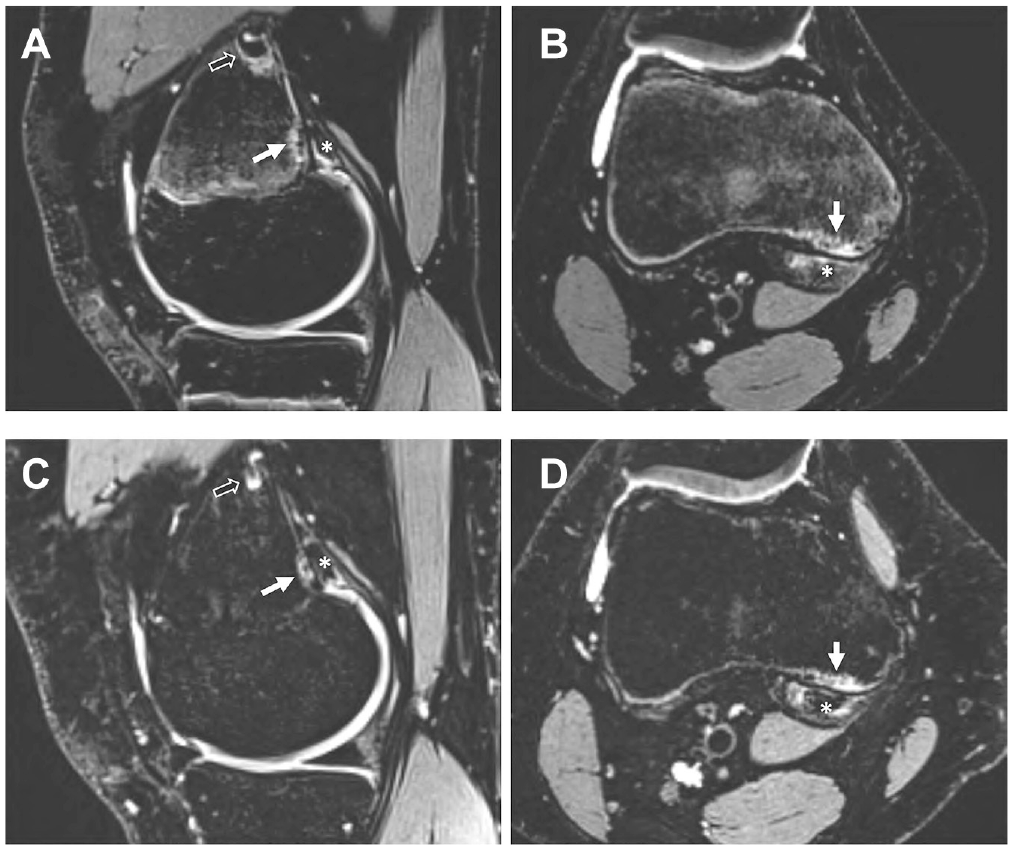
MRIs were evaluated for the presence and location of DFCIs, defined as a circumscribed high signal intensity area expanding into the bone on the T2-weighted images that is usually surrounded by a thin dark rim at the periphery, representing sclerosis. 17 DFCIs were located at 1 of 3 anatomic positions: the femoral attachment of the MHG (Figure 2), the LHG, or the attachment of the AM tendon. The size of the DFCIs was measured in sagittal orientation from anterior to posterior. Tendon reactive edema and/or cystic changes were defined as hyperintense signals on the T2-weighted images and evaluated for the tendons of the MHG, LHG, and the aponeurosis of the AM.
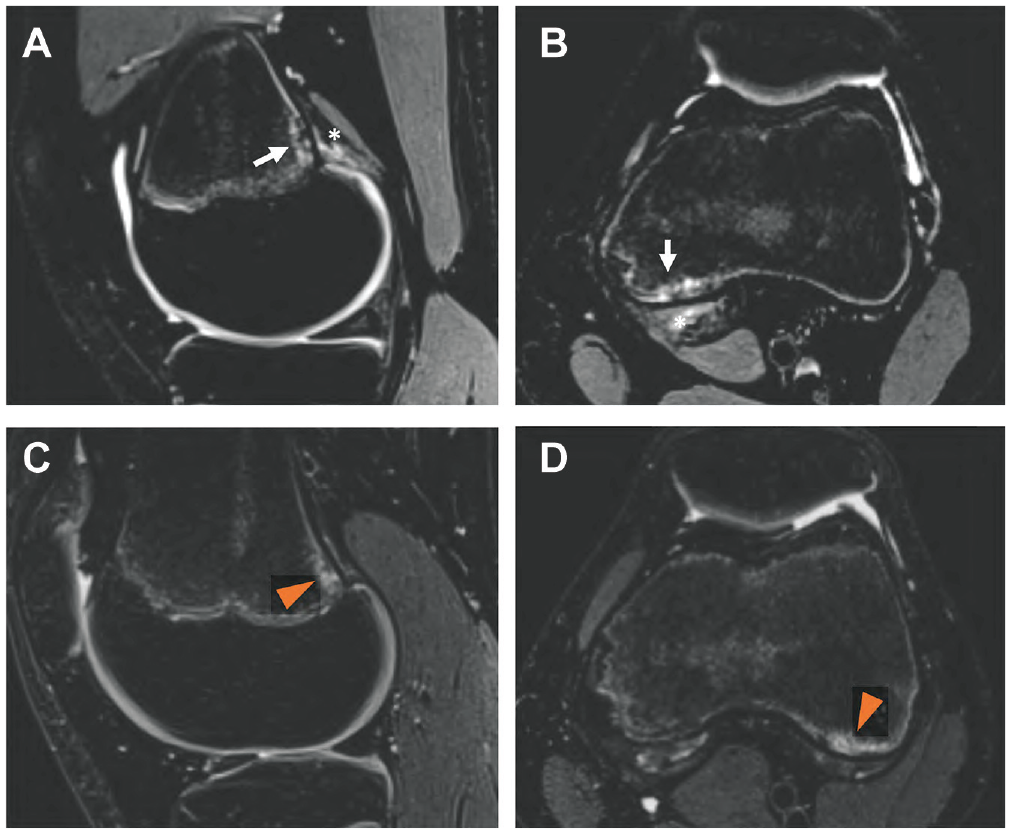
(A and B) Comparison of a baseline (sagittal and axial T2 fat-suppressed magnetic resonance imaging) distal femoral cortical irregularity (DFCI) (arrow) at the attachment site of the medial head of the gastrocnemius muscle (asterisk) in the left knee of an adolescent competitive alpine skier with (C and D) a baseline DFCI at the attachment site of the lateral head of the gastrocnemius muscle (arrowhead) in the left knee of a second athlete.
Furthermore, the status of the epiphyseal growth plate was assessed. MRIs were analyzed by 2 radiologists (C.S. and A.A.M.). Analysis was performed on a picture archiving and communication system workstation certified for clinical use (MERLIN 7.1.22; Phönix-PACS GmbH). The images were read independently in random order by the 2 radiologist, who were blinded to clinical information. Baseline and follow-up images were analyzed with ≥8 weeks apart to avoid recall bias.
Statistical Analysis
Statistical analyses were performed by 1 of the authors (G.C.F.) in SPSS Version 28.0 (IBM Corp). The prevalence and size of the DFCIs were compared between baseline and the 48-month follow-up. The measurements were compared using the Wilcoxon signed-rank test. Interrater reliability was assessed with the interclass correlation coefficient (ICC) for ordinal variables and the Cohen weighted Kappa for categorical variables. A significance level of α = .05 was used for all statistical analyses.
Results
In total, 63 athletes (mean age at follow-up, 19.6 years ± 1.2 years; n = 25 female) were included in the study. At baseline, DFCIs were detected in 84 out of 126 knees (67%), with multiple DFCIs in 3 knees with no significant difference between male and female participants (n = 23 male, n = 17 female; P = .68) (Table 1). At the 48-month follow-up, DFCIs were found in 88 out of 126 knees (70%). No significant increase was detected in the number of DFCIs between baseline and the 48-month follow-up (P = .21).
Patient Characteristics and Prevalence of DFCIs at Baseline and 48-Month Follow-up a
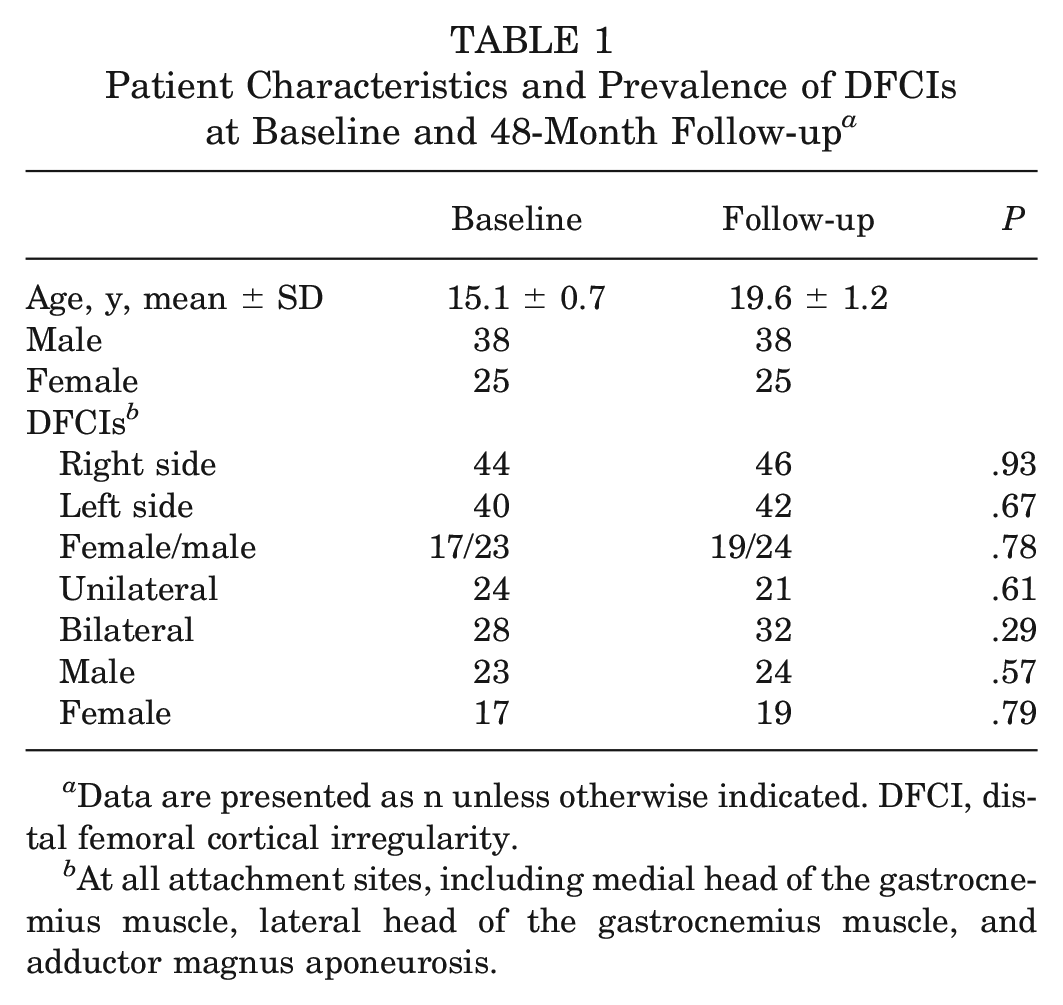
Data are presented as n unless otherwise indicated. DFCI, distal femoral cortical irregularity.
At all attachment sites, including medial head of the gastrocnemius muscle, lateral head of the gastrocnemius muscle, and adductor magnus aponeurosis.
The overall mean size of DFCIs did not change significantly between baseline and the follow-up (mean size: baseline, 3.7 ± 0.8 mm; 48-month follow-up, 3.6 ± 0.9 mm; P = .66) (Table 2). Looking at the size of DFCIs at the different locations, no significant difference was found between baseline and the 48-month follow-up (mean size MHG: baseline, 3.65 ± 0.71 mm; 48-month follow-up, 3.61 ± 0.94 mm [P = .55]; LHG: baseline, 3.86 ± 1.13 mm; 48-month follow-up, 3.71 ± 0.71 mm [P = .39]) (Figure 3). In only 1 participant was a DFCI found at the attachment site of the AM aponeurosis (baseline, 3.54 mm; follow-up, 3.61 mm). At the follow-up, no significant difference in the anterior to posterior size of DFCIs was found between the right- and left-side knees (mean right side, 3.63 ± 0.93 mm; mean left side, 3.60 ± 0.86 mm; P = .86).
Size of DFCIs at Baseline and 48-Month Follow-up a
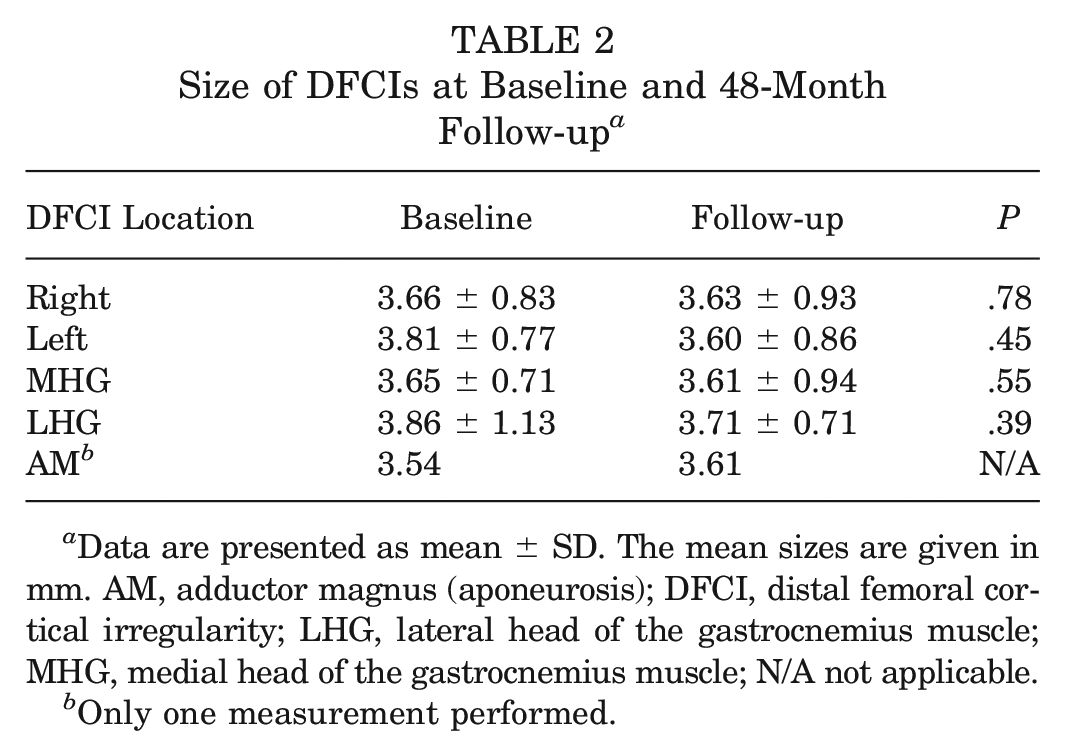
Data are presented as mean ± SD. The mean sizes are given in mm. AM, adductor magnus (aponeurosis); DFCI, distal femoral cortical irregularity; LHG, lateral head of the gastrocnemius muscle; MHG, medial head of the gastrocnemius muscle; N/A not applicable.
Only one measurement performed.
(A and B) Comparison of a baseline DFCI (solid arrow) at the proximal attachment site of the MHG (asterisk) and the distal attachment site of the MHG (outlined arrow) in the right knee of an adolescent competitive alpine skier (sagittal and axial T2 fat-suppressed magnetic resonance imaging) with the (C and D) 48-month follow-up. Note how the size of the DFCI does not change during skeletal maturation, while the epiphyseal growth plate is completely ossified at the 48-month follow-up. DFCI, distal femoral cortical irregularity; MHG, medial head of the gastrocnemius muscle.
At the 48-month follow-up, edema/cystic changes of the tendon attachment site were detected in 28 out of 63 cases (44%) at the MHG tendon, in 8 out of 63 cases (13%) at the LHG, and in zero cases (0%) at the aponeurosis at the AM. No significant differences were found between baseline and the 48-month follow-up (P > .05) (Table 3).
Reactive Edema/Cystic Changes of the Tendon Attachment Sites at Baseline and 48-Month Follow-up a
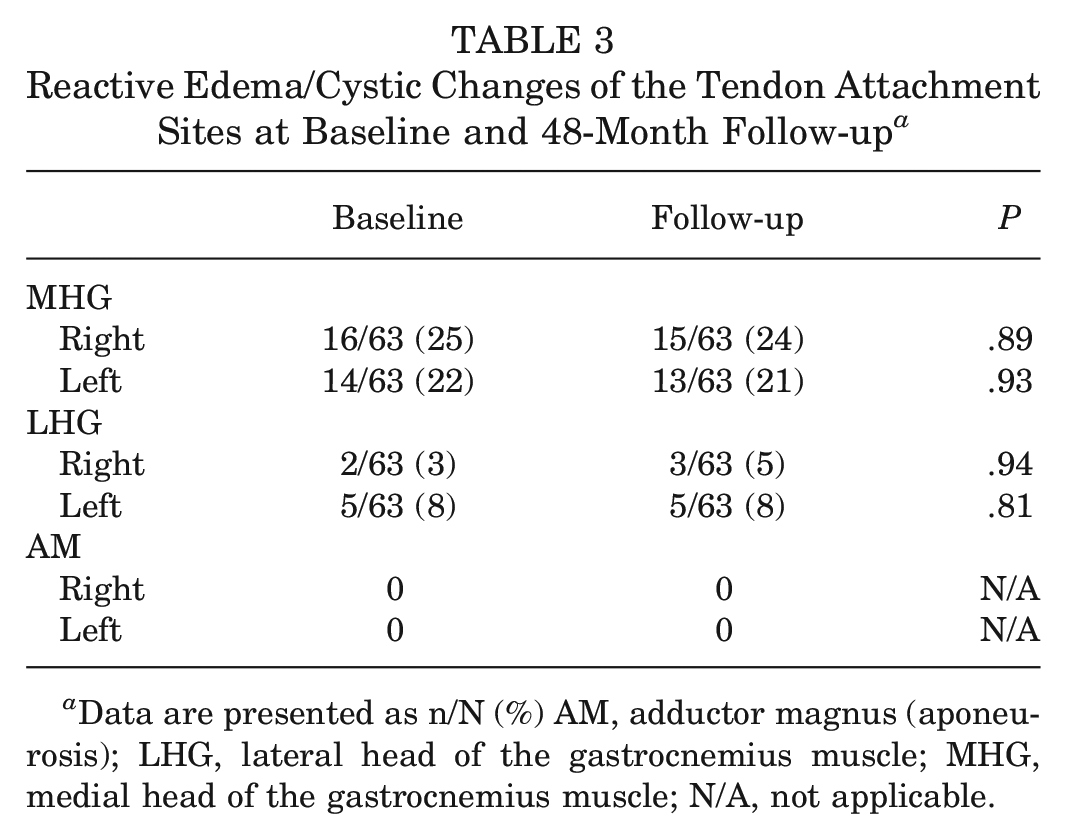
Data are presented as n/N (%) AM, adductor magnus (aponeurosis); LHG, lateral head of the gastrocnemius muscle; MHG, medial head of the gastrocnemius muscle; N/A, not applicable.
Concomitant Findings
Almost all athletes (n = 61 [97%]) demonstrated open epiphyseal growth plates at baseline. However, at the 48-month follow-up, 58 athletes (92%) showed fusion of epiphyseal growth plates, while 5 (8%) athletes had partial fusion of epiphyseal growth plates.
The number of focal periphyseal edema zones detected at the 48-month follow-up was significantly smaller compared with baseline (baseline, n = 21; 48-month follow-up, n = 1 [P < .001]).
Interrater Agreement
The agreement on the detection and location of DFCIs was perfect (κ, 1). The interrater agreement for the measurement of DFCIs was good to excellent (ICC, 0.88 [95% CI, 0.82-0.96]) as well as for the detection of edema in the adjacent tendons (ICC, 0.91 [95% CI, 0.86-0.98).
Discussion
In this study, a longitudinal assessment of DFCIs in adolescent competitive alpine skiers was performed over a 48-month follow-up. Even though it is described in the literature that DFCIs generally resolve during adolescence, our study revealed that the frequency and size of DFCIs remained constant in competitive alpine skiers even after skeletal maturation.
DFCIs were described several decades ago; nonetheless, there are still controversial discussions about the underlying pathophysiology of DFCIs and their clinical management.5,21 Resnick and Greenway 13 assessed the pathophysiology of DFCIs in a comprehensive review of 21 cases in the 1980s and described 2 types of lesions: (1) femoral cortical irregularities at the attachment site of the AM and (2) femoral cortical excavations at the attachment site of the MHG. They noted that these lesions might be caused by either shear stress or traumatic insult to the periosteum, resulting in reactive proliferation of fibrous and osseous tissue. On the other hand, it has been suggested that they may be the result of exaggerated physiologic changes that occur during skeletal maturation.1,6,13,14,25 The results of our longitudinal study support the assumption that DFCIs are based on chronic stress or repetitive trauma. Only highly active competitive athletes were recruited for this study, and a DFCI prevalence of 67% to 70% (baseline and 48-month follow-up) was observed in contrast to a prevalence of 3.6% to 11.5% described for the general population.8,15 In contrast to the study by Resnick and Greenway, in our study, DFCIs were predominantly observed at the attachment site of the MHG tendon and only in 1 case was it observed at the attachment site of the AM aponeurosis. These observations are consistent with those by Suh et al, 18 who found 58 DFCIs at the attachment of the MHG tendon in a study with 100 knees, and no cases at the AM location.
The generally high occurrence of DFCI and the predominance of the MHG tendon attachment site might also be explained by the unique motion patterns during alpine skiing. The forward flexed position of the knee during skiing, in combination with ankle dorsiflexion in the relatively rigid ski-binding-boot interface, is likely to put excessive stress on the femoral origin of the gastrocnemius muscle.7,9,10 During a carving turn, the hip is adducted and internally rotated, and the flexed knee of the outside ski undergoes a dynamic valgus moment, causing knee abduction and internal rotation. These forces further stress the MHG. 26 Furthermore, in competitive alpine skiing, loads of up to 1.75 times the body weight are exerted on the outer leg, creating extensive shear stress on the tendon attachment sites.16,19,24 Figure 4 illustrates the typical knee and ankle joint kinematics during alpine skiing and their relation to the tug on the gastrocnemius attachment sites on the distal femur.
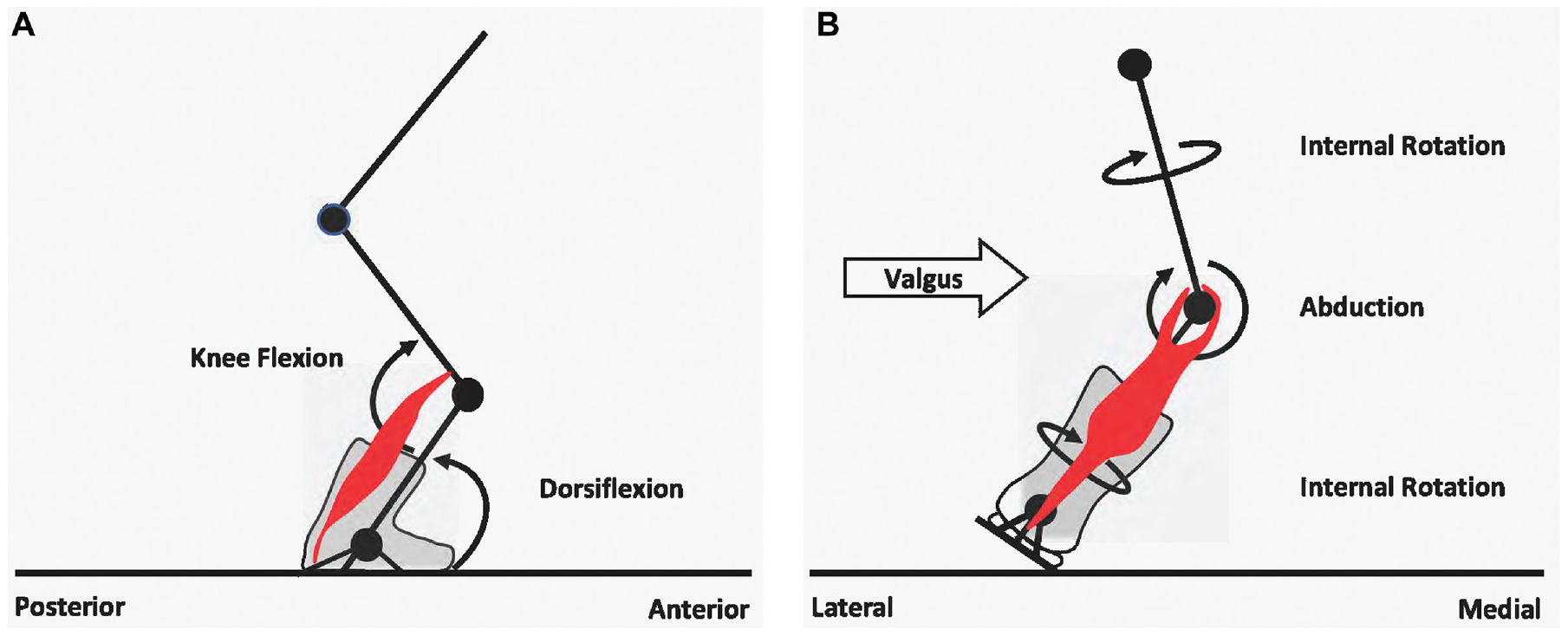
(A and B) Schematic drawing of the knee and ankle joint kinematics during alpine skiing. The knee and ankle are in persistent flexed positions, inducing extensive shear stress on the gastrocnemius muscle (red). (B) During a carving turn, the femur of the loaded outer leg is internally rotated while the knee is in valgus stress, inducing further loading on the MHG, which might explain the higher incidence of DFCI at the MHG attachment site. DFCI, distal femoral cortical irregularity; MHG, medial head of the gastrocnemius muscle.
In this study, skeletal maturation had no significant effect on the size and prevalence of DFCIs. At the 48-month follow-up imaging, almost all participants were physically full-grown (19.6 ± 1.2 years) with closed epiphyseal growth plates. However, neither the prevalence nor the size of DFCIs changed significantly between baseline and the 48-month follow-up (P > .05). In previous studies, DFCIs have often been described as self-limiting lesions that disappear throughout adolescence.4,8,11-13 In a case report by Tscholl et al, 20 the DFCIs of a female gymnast and a female judoka resolved over 2 years. However, there was no information on their level of physical activity during the follow-up period.
This was the first study that observed DFCIs longitudinally over 48 months in a homogeneous athletic cohort of active competitive skiing athletes. Contrary to previous studies, the results of this study suggest that DFCIs are a reaction to excessive shear stress that persists throughout skeletal maturation, especially in competitive athletes with high physical demands over a long period. Mester et al 12 recently assessed DFCIs in a cohort of 21 children and found an association with localized posteromedial knee pain in 53%. The patients were treated nonoperatively with structured physical therapy and rest from physically demanding sportive activities. However, after a follow-up period of approximately 12 months, complete remission was observed in only 38% of patients.
No longitudinal assessment of the DFCI morphology on MRI was performed, but the results of Mester et al 12 support the assumption that DFCIs are not solely self-limiting and that some might benefit from structured physical therapy. In our study, DFCIs were persistent, and it is important to note that invasive diagnostic procedures such as biopsies should generally be avoided. Previous histologic correlations of DFCI described them as reactive processes with increased osteoclastic activity and proliferating fibrous and osteocartilaginous tissues.8,17,21,23 DFCIs are solely benign lesions and should be regarded as “do not touch” lesions.
Our study was associated with some limitations that should be considered when interpreting the study findings: only competitive skiing athletes were enrolled. This might introduce a sport-specific selection bias and limit the applicability of these findings to other sports. Furthermore, no histopathologic examination was performed, and diagnosis of the DFCIs was based on the characteristic morphologic features on MRI. No information was available on clinical symptoms associated with DFCIs. In addition, there was a high rate of loss to follow-up after 48 months, which may be explained by a shift in personal focus from competitive sports to completion of higher education or simply a failure to maintain a high level of physical fitness for engaging in competitive sports.
Conclusion
DFCIs are common findings on knee MRI in adolescent alpine skiers, but they do not significantly change in size over time and they persist into skeletal maturity.
Footnotes
Acknowledgements
The authors thank Daniel Fitze, Jonas Hanimann, and Daniela Meyer for conducting the MRI studies and Sabine Schrimpf for critical proofreading. Special thanks go to the Swiss Center for Musculoskeletal Imaging, Balgrist Campus AG, Zurich, where the study was performed.
Submitted August 28, 2023; accepted February 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was received from the Balgrist Foundation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.