
Abstract
Background
HIV couple counseling (HIVCC) acceptance during antenatal care and associated transmission outcomes have not been evaluated.
Methods
A prospective study was conducted among pregnant women and their partners.
Results
Of the 139 participating couples, most (>90%) had good knowledge about HIV transmission prevention, 5% and 4% of pregnant women and their partners were categorized as moderate or high risk for HIV acquisition. These moderate or high-risk groups had a false perception of low HIV risk. The HIVCC acceptance rate was 85%. Independent factors associated with no HIVCC acceptance in pregnant women included lower HIV knowledge score (adjusted odds ratio [aOR 2.56; P = .003]), self-payment for medical expense (aOR 9.81; P = .008), and non-Thai nationality (aOR 3.60; P = .018). There was no HIV or syphilis acquisition among all pregnant women during pregnancy.
Conclusions
The interventions to improve HIVCC acceptance should include providing HIV education, coverage for medical expenses, and financial assistance for non-Thai couples.
Introduction
Human immunodeficiency virus (HIV) infection poses a significant public health challenge and contributes substantially to morbidity and mortality. Approximately 39.9 million people worldwide are living with HIV with 1.3 million new infections in 2023, 1 underscoring the ongoing urgency to end the global HIV epidemic. In Thailand, around 560,000 adults and children are currently living with HIV with 9,100 new cases reported in 2023. 2 Recent data from the Ministry of Public Health show that patterns of HIV transmission among Thai adults are diverse; 65% of transmissions are among men who have sex with men, 23% among heterosexual serodiscordant couples, 11% through casual sexual encounters, 3% via shared needles, and 1.6% through mother-to-child transmission. 3 These data suggest that targeted interventions within serodiscordant couples are essential and can significantly reduce the overall incidence of HIV infection. One of the interventions is HIV couple counseling (HIVCC), which presents a vital opportunity for couples to be tested together, to make informed decisions regarding their health, to prevent horizontal and vertical transmission of HIV and sexually transmitted infections (STIs), and to initiate antiretroviral therapy (ART) and STI treatment if indicated.
A study conducted in rural Malawi found that antenatal care (ANC) settings provide one of the most effective opportunities for accessing HIV counseling and testing among individuals of reproductive age. 4 In addition, previous studies in South Africa and Kenya demonstrated that voluntary HIVCC led to a significant reduction in HIV transmission among serodiscordant couples, STIs, and mother-to-child transmission.5,6 HIVCC in ANC settings has been associated with multiple benefits, including increased male involvement in care, enhanced communication between partners, and improved awareness of HIV status. However, despite these known benefits, maternal deaths and HIV infections in infants continue to occur, which are often linked to the low HIVCC during pregnancy. 6
In Thailand, while many healthcare facilities offer HIVCC, its utilization remains limited and is often confined to settings with adequate resources and specific groups at high risk for HIV acquisition. Moreover, there is a notable lack of comprehensive data on HIVCC acceptance, particularly among general couples in which both partners are unaware of their HIV status. This study aimed to assess the acceptance rate of HIVCC, identify factors associated with HIVCC non-acceptance, reasons for HIVCC acceptance and non-acceptance, evaluate the level of HIV knowledge among couples, and investigate HIV-related risks, risk perception, and transmission outcomes during pregnancy, defined as STI outcomes among pregnant women and their partners, in both the HIVCC acceptance and non-acceptance groups.
Methods
Study Design and Participants
This prospective cohort study was conducted among pregnant women and their partners receiving ANC at the Thammasat University Hospital (TUH) between May 9, 2024, and March 31, 2025. Inclusion criteria were pregnant women and their partners aged 18 or older who received their first ANC at TUH. Exclusion criteria comprised those who refused to participate, had incomplete questionnaire responses, or could not speak and understand Thai. The study protocol was reviewed and approved by the Human Research Ethics Committee on May 9, 2024. The study was conducted in accordance with the amended Declaration of Helsinki, the Belmont Report, the Council for International Organizations of Medical Sciences (CIOMS) Guidelines, and the International Conference on Harmonization-Good Clinical Practice (ICH-GCP). Informed consent was obtained from all participants prior to the study participation.
Study Protocol
Eligible pregnant women and their partners were approached and asked to participate in the study. Those who gave informed consent were asked to complete the study questionnaire independently. The questionnaire was developed based on expert input from board-certified infectious disease specialists and obstetrics and gynecology consultants, ensuring clinical appropriateness and contextual relevance. The questionnaire encompassed 5 key domains: (1) general sociodemographic and health information, (2) obstetric history (completed by pregnant women only), (3) HIV-related risk behaviors and risk perception, (4) HIV-related knowledge, and (5) acceptance of HIVCC and reasons for accepting and not accepting HIVCC. In addition to self-reported data, relevant laboratory results were obtained from participants’ medical records for subsequent analysis. For pregnant women, these included HIV, hepatitis B virus, and syphilis test results from the first ANC visit, and followed-up HIV and syphilis testing performed between 28 and 32 weeks of gestation. The HIV and syphilis test results of their partners were performed only at the initial ANC visit according to the national guidelines. Confidentiality and privacy of all participant data were maintained throughout the study. To minimize the missing data, the questionnaire completed by each study participant was reviewed for completeness by the on-site research assistants prior to submission, while data prospectively collected from participants’ medical records were reported as they were with information about the missing data.
To evaluate participants’ knowledge related to HIV and STIs testing and prevention, as well as HIVCC, the participants responded to 10 provided statements, whether they were true, false, or unknown. One point was given to each correct response, with a total score of 10. Regarding risk perception assessment, participants self-assessed their own HIV risk levels as “No risk at all,” “A little risk (low risk),” “More than a little (moderate risk),” or “A lot of risk (high risk)” through the questionnaire. The investigators classified participants into actual HIV risk levels as low, moderate, or high using pre-specified risk characteristics and behaviors reported in the previous study (Supplemental Table 1). 7 Only one characteristic or behavior that met a certain risk level was required to classify the participants into that risk level. Of note, couples who reported having only one sexual partner and not using condoms during sexual intercourse were categorized as low risk. False perception of low HIV risk was defined as perceiving self as no or low risk despite having actual moderate or high risk based on the study categorization tool.
The primary outcome of the study was HIVCC acceptance rate among pregnant women and their partners. This outcome was measured by dividing the number of couples who accepted HIVCC by the total number of couples participating in the study and multiplying by 100. Secondary outcomes included factors associated with HIVCC non-acceptance, determined by comparing characteristics between the participants who accept and did not accept HIVCC, reasons for accepting or refusing HIVCC, measured as percentage of each reason provided, HIV and HIVCC-related knowledge, calculated into a score based on the number of correct responses to the provided statements, HIV risks, risk behaviors, and risk perception, measured as percentage of each risk, risk behavior, and risk perception category, and HIV and syphilis transmission during pregnancy, determined by the number of pregnant women who had acquired HIV and/or syphilis evidenced by the conversion for anti-HIV and/or Venereal Disease Research Laboratory test from a negative result at baseline to a positive result at the follow-up.
Statistical Analysis
Given no previous study on the HIVCC acceptance rate, the sample size for this study was determined based on the HIVCC acceptance rate of 90% observed at the ANC of TUH in the previous year, prior to study enrollment. With a margin of error of 5% and a significance level of 0.05, the required sample size was 139. Descriptive data were reported in numbers (percentage) and median (interquartile range, IQR). Categorical variables were compared between groups using Chi-square or Fisher's exact tests as appropriate, while continuous variables were compared using the Mann–Whitney U-test. A P-value of less than .05 was considered statistically significant. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were calculated through multivariable logistic regression analysis to identify independent factors associated with HIVCC non-acceptance. Primary outcome and all of the secondary outcomes, except for the transmission outcomes, were collected at enrollment using the questionnaire. All data analyses were conducted using SPSS version 29 (Chicago, IL, USA). 8
Results
Demographic, Health, and Obstetrics Characteristics of All Study Participants
A total of 139 pregnant women were enrolled in this study and categorized into 2 groups based on their acceptance or refusal of HIVCC (Table 1). The median age of the pregnant women was 30 years (IQR 26-34 years). Most participants were Thai (59%). Notably, 74% of the pregnant women self-paid for ANC. The median gestational age at the first ANC visit was 12 weeks, and 42% were in their first pregnancy. Among the 139 partners of pregnant women, the median age was 32 years (IQR 28-36 years). Most were Thai (59%), and 54% self-paid for medical services (Table 2).
Demographic, Health and Obstetrics Characteristics of Pregnant Women Participants Categorized by HIV Couple Counseling Acceptance.

Data are in numbers (%) unless indicated otherwise.
Abbreviations: ANC, antenatal care; HIV, human immunodeficiency virus; HIVCC, HIV couple counseling; IQR, Interquartile range.
Comparison between participants who accepted and did not accept HIVCC.
For those with the previous pregnancy.
Demographic, Health and Obstetrics Characteristic of Partners of Pregnant Women Participants Categorized by HIV Couple Counseling Acceptance.

Data are in numbers (%) unless indicated otherwise.
Abbreviations: HIV, human immunodeficiency virus; HIVCC, HIV couple counseling; IQR, Interquartile range.
Comparison between participants who accepted and did not accept HIVCC.
HIV Risk, Risk Behaviors, and Risk Perception of All Study Participants Categorized by HIVCC Acceptance
HIV risk and risk behaviors among the participating pregnant women and their partners are shown in Tables 3 and 4, respectively. All of the 139 couples (100%) perceived themselves as having no HIV risk. However, based on the risk stratification tool (Supplemental Table 1), 95% of pregnant women (Table 3) and 96% of their partners (Table 4) were classified as low risk. Among pregnant women, 6 (4%) were classified as high risk and 1 (1%) as moderate risk. The moderate-risk individual reported using alcohol during sex within the past 30 days. Six partners of the pregnant women (4%) were classified as high risk due to recent STIs or having a partner with an STI history. Notably, all of the participants who were classified as moderate or high risk perceived themselves as having no risk of HIV infection, resulting in a false perception of low HIV risk of 5% in pregnant women and 4% in their partners (Tables 3 and 4).
HIV Risk, Risk Behaviors and Risk Perception of Pregnant Women Participants Categorized by HIV Couple Counseling Acceptance.

Data are in numbers (%) unless indicated otherwise.
Abbreviations: HIV, human immunodeficiency virus; HIVCC, HIV couple counseling; IQR, interquartile range; PID, pelvic inflammatory disease; STIs, sexually transmitted infections.
Comparison between participants who accepted and did not accept HIVCC.
HIV Risk, Risk Behaviors and Risk Perception of Partners of Pregnant Women Participants Categorized by HIV Couple Counseling Acceptance.
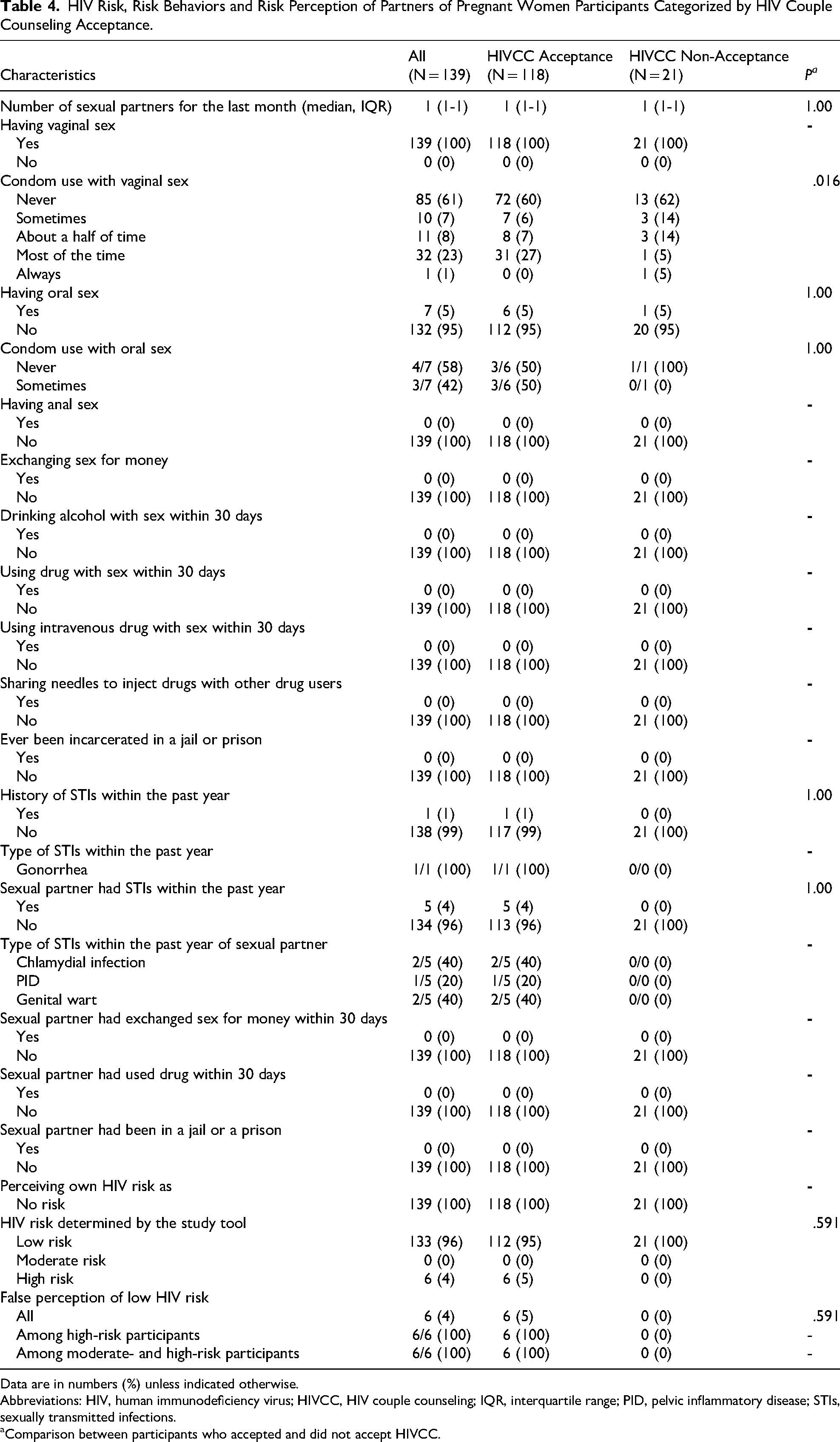
Data are in numbers (%) unless indicated otherwise.
Abbreviations: HIV, human immunodeficiency virus; HIVCC, HIV couple counseling; IQR, interquartile range; PID, pelvic inflammatory disease; STIs, sexually transmitted infections.
Comparison between participants who accepted and did not accept HIVCC.
Knowledge About HIV Infection Among All Study Participants Categorized by Couple Counseling Acceptance
Most pregnant women had a high level of HIV-related knowledge (Supplemental Table 2), with over 90% responding correctly on statements related to ART, mother-to-child transmission, routine STI screening, HIVCC recommendations, and their role in facilitating disclosure and care. However, the knowledge level was lowest for the recommendation about HIV testing twice during pregnancy (77%). Pregnant women who declined HIVCC were less knowledgeable about the recommendation for HIV testing twice during pregnancy (P = .024), the importance of partner's HIV testing during pregnancy (P = .03), and the routine of HIV, syphilis, and hepatitis B screening for ANC (P = .025). Among their partners, the overall knowledge level was high (>90%) (Supplemental Table 3). However, less than 90% recognized that HIVCC supports disclosure and care coordination, and understood the importance of early ART initiation during pregnancy. For both statements, those who declined HIVCC were significantly less knowledgeable than those accepting HIVCC (P < .001).
HIV Couple Counseling Acceptance
Of the 139 couples who participated in the study, 118 couples (85%) accepted HIVCC. The most common reason for HIVCC acceptance was the belief that HIVCC improves disclosure and care for couples with differing test results (99% of pregnant women and 96% of their partners), followed by knowing HIV status of themselves and their partners (95% of pregnant women and 94% of their partners) and prompt treatment can be initiated to prevent infection transmission (78% of pregnant women and 95% of their partners). Conversely, the major reason for the declining HIVCC among pregnant women was inability to come for follow-up blood tests during pregnancy (67%), followed by not wanting their partners to know their HIV test results (58%), and not wanting to know their own HIV status (48%), while the most common reason for declining HIVCC among their partners was not wanting their partners to know their HIV test results (86%), inability to come for follow-up blood tests (67%), and not wanting to know their own HIV status (52%). By multivariable logistic regression analysis, the independent factors associated with HIVCC non-acceptance among pregnant women were lower HIV knowledge score (aOR 2.56, 95% CI 1.37-4.78; P = .003), self-payment for medical expenses (aOR 9.81, 95% CI 1.27-75.51; P = .008), and non-Thai nationality (aOR 3.60, 95% CI 1.24-10.45; P = .02), while the independent factors associated with HIVCC non-acceptance among their partners were lower HIV knowledge score (aOR 27.78, 95% CI 6.25-125.00; P < .001) and self-payment for medical expenses (aOR 381.37, 95% CI 9.18-15851.96; P = .002) (Table 5).
Univariable and Multivariable Analyses for Factors Associated With No HIV Couple Counseling Acceptance.

Abbreviations: CI, confidence interval; HIV, human immunodeficiency virus; OR, odds ratio.
Not selected in the final model due to being covariated with lower HIV couple counseling knowledge score.
HIV and STI Testing Results and Transmission Outcomes Among All Study Participants
At the initial ANC visit, baseline testing identified 1 pregnant woman with HIV infection, 1 with hepatitis B, and 1 with syphilis. All of the 3 pregnant women were in the HIVCC acceptance group and received treatment according to their infections. Follow-up testing for HIV and syphilis between 28 and 34 weeks of gestation revealed no new HIV infections and syphilis among those with initial negative tests in both HIVCC acceptance and non-acceptance groups. However, 4 women did not return for this follow-up testing (2 in each group). Their partners were tested at baseline, with no HIV infection or syphilis detected. No other new development and transmission of HIV and STIs occurred and were reported among all couples, including those with discordant baseline results of HIV infection, hepatitis B, and syphilis.
Discussion
This study demonstrated a high acceptance rate of HIVCC among pregnant women and their partners (85%), aligning with the 86% acceptance rate reported previously. 9 This finding highlights that HIVCC is highly acceptable when strategically promoted during pregnancy care. In this study, trained nurses encouraged all pregnant women and invited attending male partners to participate in HIVCC without formally embedding it into routine ANC services, while the previous study 9 incorporated HIVCC into standard ANC workflows using healthcare provider training. Both studies underscore the critical role of trained healthcare providers, early engagement, and clear communication of the benefits of HIVCC. To further optimize HIVCC uptake, future programs should strengthen early counselling by trained providers, integrate HIVCC into ANC services where feasible, promote male partner involvement, and ensure prompt access to ART.
One of the key reasons for HIVCC acceptance in this study was the desire to know a partner's HIV status and the belief that counselling would help with disclosure and managing discordant results. A literature review found no earlier studies that directly asked participants about their reasons for accepting HIVCC,5,10 making this study the first to explore this area systematically. This finding highlights the importance of assessing and properly managing couples’ unmet needs and promoting mutual disclosure to increase HIVCC acceptance. In contrast, the primary reasons for HIVCC non-acceptance included a lack of interest in knowing the HIV status, concern about the disclosure of test results to the partner, and inability to attend blood tests during pregnancy check-ups. These factors are consistent with findings from previous studies,4,5 which have shown that lack of awareness or fear of stigma often prevents individuals from participating in HIV testing and counseling. Given these insights, future interventions should emphasize the critical importance of mutual HIV status awareness to allow timely access to ART and other preventive measures. Additionally, education should be provided about the need for repeat HIV testing during pregnancy, particularly given the possibility of seroconversion during gestation. Pregnant women should be well prepared since their first ANC visit about the timeline and importance of follow-up testing.
This study also identified some key factors that might influence the HIVCC acceptance. Notably, a lower level of HIV knowledge was a significant factor associated with the non-acceptance of HIVCC. This finding is consistent with a previous study, which reported that low awareness and knowledge about HIV transmission contributed to reduced acceptance of HIV counseling 5 and underscores the importance of education and awareness programs targeted at pregnant women and their partners. Another significant associated factor was self-payment for the ANC, which may limit access to HIVCC services. This result corresponds with those reported by Aarnio et al, 4 which identified economic barriers as a major impediment to HIV testing and counseling in low-resource settings. Interventions, such as reducing the cost of laboratory testing during ANC or making the tests as essential items that can be covered for all under the national medical coverage scheme, should be considered to be implemented to reduce this economic burden. Having non-Thai nationality was also significantly associated with HIVCC non-acceptance. The reasons were likely due to inequitable access to essential HIV services among migrants, structural barriers, such as language barriers and cultural differences, and low socioeconomic status. 4 Together, these findings may underscore the need for inclusive migrant HIV prevention strategies, particularly within ANC services.
A notable finding from this study was the disconnection between actual and perceived HIV risk among pregnant women and their partners. Although the rates of false perception of low risk were low, these findings highlight a significant gap in awareness of HIV risk and undermine the impact on preventive strategies implementation during pregnancy. This misperception can lead to a lack of engagement with preventive services, delayed diagnosis, and increased risk of HIV transmission. Previous studies found that participants who tested positive for HIV or other STIs and engaged in risk behaviors reported scoring low on perceived risk assessments.11,12 In addition, having a false perception of low HIV risk was demonstrated as an independent factor associated with HIV positivity and no interest in PrEP among at-risk populations.8,13 A study by Machemedze et al 14 revealed that individuals who endorsed stigmatizing beliefs toward people with HIV were significantly more likely to perceive themselves as not being at risk, despite engaging in high-risk behaviors. Altogether, these findings suggest that self-assessment alone may be insufficient to identify those who can benefit from HIV preventive services, and there is a need for enhanced, evidence-based risk communication strategies in HIV counseling strategies that directly address the psychological and sociocultural drivers of inaccurate risk perception. The integration of validated risk assessment tools and stigma-reduction messaging into ANC could possibly improve individuals’ capacity to accurately assess their HIV risk and subsequently increase uptake of HIVCC.
This study has some limitations. First, the results were from a single center and might have limited generalizability to other settings with different populations, management protocols and polices. Second, most data were collected through self-administered questionnaires, which might be subject to response bias, particularly due to misinterpretation and underreporting of sensitive behaviors. Similar concerns were raised by Rosenberg et al 15 who noted that participants may overreport condom use and underreport sexual risk behaviors following HIV testing and counseling. Third, the HIV risk categorization was adapted from a previous study developed in a U.S. population with a limited number of Asian population and has not been validated in our antenatal population in Thailand. Fourth, the HIV knowledge questionnaires were newly developed and not formally validated, which may limit the interpretability of the knowledge scores. Fifth, due to the small number of discordant couples in the study, analysis of HIV transmission within discordant couples was difficult. We were unable to elaborate further on the transmission outcome among serodiscordant couples. Additional data collections are required to assess the transmission outcome among serodiscordant couples. Lastly, since most participants were categorized as low risk for HIV, we did not observe the different outcomes for HIV and other STI transmission among couples who accepted and did not accept HIVCC. This finding may not be applicable to other settings with higher-risk populations.
Conclusions
The findings suggest the need for further improvement of HIVCC acceptance among pregnant women and their partners in our setting. The interventions should include providing education and campaigns about HIV and transmission prevention, while among those who had no coverage for their medical expenses and were non-Thai couples, strategies to reduce their financial burden should be considered and may include expanding access to affordable, comprehensive healthcare systems and improving healthcare access for foreigners.
Supplemental Material
sj-doc-1-jia-10.1177_23259582261446449 - Supplemental material for Acceptance of HIV Couple Counseling and Transmission Outcomes Among Pregnant Women and Their Partners
Supplemental material, sj-doc-1-jia-10.1177_23259582261446449 for Acceptance of HIV Couple Counseling and Transmission Outcomes Among Pregnant Women and Their Partners by Dareena Yamoh, Supapen Lertvutivivat and Thana Khawcharoenporn in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-doc-2-jia-10.1177_23259582261446449 - Supplemental material for Acceptance of HIV Couple Counseling and Transmission Outcomes Among Pregnant Women and Their Partners
Supplemental material, sj-doc-2-jia-10.1177_23259582261446449 for Acceptance of HIV Couple Counseling and Transmission Outcomes Among Pregnant Women and Their Partners by Dareena Yamoh, Supapen Lertvutivivat and Thana Khawcharoenporn in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-doc-3-jia-10.1177_23259582261446449 - Supplemental material for Acceptance of HIV Couple Counseling and Transmission Outcomes Among Pregnant Women and Their Partners
Supplemental material, sj-doc-3-jia-10.1177_23259582261446449 for Acceptance of HIV Couple Counseling and Transmission Outcomes Among Pregnant Women and Their Partners by Dareena Yamoh, Supapen Lertvutivivat and Thana Khawcharoenporn in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We would like to thank the Obstetrics-Gynecology and antenatal care clinic personnel and all study participants for their great contribution to this study.
Ethical Statement
The study protocol was reviewed and approved by the Human Research Ethics Committee of Thammasat University (approval number 127/2567) on May 9, 2024. The study was conducted in accordance with the amended Declaration of Helsinki, the Belmont Report, the Council for International Organizations of Medical Sciences (CIOMS) Guidelines, and the International Conference on Harmonization-Good Clinical Practice (ICH-GCP).
Informed Consent/Patient Consent
All participants provided written informed consent prior to participating.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.