
Abstract
Introduction
Hypertension has emerged as a significant comorbidity among people living with Human Immunodeficiency Virus (HIV). However, the prevalence and determinants of hypertension in Ethiopia remain inconsistent across studies.
Methods
A systematic search of PubMed, Science Direct, Cochrane Library, Hinari, and Google Scholar was conducted following PRISMA 2020 guidelines. Both published and grey literature conducted in Ethiopia were included. The Newcastle Ottawa scale was used to assess the quality of included studies.
Results
Pooled prevalence of hypertension among people living with HIV in Ethiopia was 22% (95% CI: 17.0-28.0). Factors significantly associated with hypertension among people living with HIV included physical inactivity (AOR=2.73; 95% CI: 2.05-3.41), excessive alcohol drinking (AOR=3.01; 95% CI: 1.41-4.61), and ART duration ≥5 years (AOR=2.50; 95% CI: 1.46-3.54).
Conclusion
Hypertension affects approximately one in five people living with HIV in Ethiopia. Physical inactivity, alcohol use and long-term ART were significantly associated with Hypertension.
Introduction
Hypertension has emerged as one of the most significant non-communicable comorbid condition among people living with HIV, particularly in low- and middle-income countries where both HIV and non-communicable disease (NCD) burdens are high. Globally, over 1.28 billion adults live with hypertension, with two-thirds residing in low and middle income countries.1,2 In sub-Saharan Africa, a region heavily affected by HIV, the intersection of HIV infection and cardiovascular disease represents a growing public health challenge. 3
There was significant regional variation, with the highest prevalence in Western/Central Europe and North America (28.1%) and the lowest in Asia-Pacific (16.5%), according to a larger global review of 194 studies conducted in 61 countries. The pooled prevalence was 23.6% (95% CI: 21.6%–25.5%), and there were correlations with antiretroviral therapy (ART) exposure, ageing, and rising trends over time. 4 Region-specific estimates from East Africa point to a pooled prevalence of 19.75% (95% CI: 16.07%–23.42%) among PLHIV. 5
People living with HIV (PLHIV) have a high and increasing prevalence of hypertension worldwide. Based on a meta-analysis of 194 studies including 396,776 PLHIV from 61 countries, the pooled global prevalence of hypertension was 23.6%, with rates being higher in high-income areas and among those who had previously used ART. 4 A systematic review covering sub-Saharan Africa (SSA) (150,886 PLHIV) reported a pooled hypertension prevalence of 19.6%, but low awareness (28.4%) and control rates (13.4%). Older age (> 45 years) and BMI > 25 kg/m2 were significant correlates. 6
In many low-and middle-income nations, including Ethiopia, routine hypertension screening and therapy are not systematically incorporated into HIV care services, despite the growing dual burden of HIV and hypertension. 5 Evidence at the national level summarizing the prevalence and contributing factors of hypertension among people living with HIV is still lacking. In order to improve integrated chronic illness care systems, distribute resources efficiently, and influence health policy, it is imperative to comprehend these trends.
The high and increasing prevalence of hypertension among PLHIV is highlighted by these findings, which are caused by both HIV-specific factors (ART exposure, CD4 count, duration of infection) and traditional determinants (age, obesity, and lifestyle). Estimates at the national level are obviously needed in Ethiopia or comparable contexts to guide integrated HIV care platforms’ screening, management, and prevention initiatives for hypertension. Hypertension can be classified primary or secondary, but most studies among people living with HIV do not differentiate these types. Therefore, this systematic review and meta-analysis examine the overall prevalence of hypertension, regardless of subtypes, and its associated factors in this population. The primary objective was to determine the pooled prevalence of hypertension among PLHIV in Ethiopia. Secondary objectives were to identify factors associated with hypertension among PLHIV and assess regional variations in hypertension prevalence among PLHIV in Ethiopia.
Methods
Protocol Registration
The protocol was registered with the international registration of systems review (PROSPERO) under protocol number CRD420251121364 in order to prevent repeating the same review, to increase transparency, and to reduce reporting bias in the current study. 7 The completed PRISMA checklist is provided as Supplementary File (SF1).
Study Design
Systematic review and meta-analysis
Study Setting
The included primary studies were conducted among HIV infected patients in Ethiopia.
Search Approach and Appraisal of Studies
For our review procedure, we used the most recent version of the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist. Two authors independently conducted separate searches for relevant studies to include in this meta-analysis and systematic review. All research involving human participants carried out before the search date was taken into account. Our method, which was based on the CoCo PoP mnemonic principle, included doing sensitive searches that used Boolean operators to join text words. The following were the criteria: Condition- hypertension; Context- Ethiopia; Population- HIV patients.
The databases PubMed, Cochrane Library, Hinari, and Science Direct were searched extensively, and documents were retrieved in order to locate potentially pertinent published and unpublished papers. Additionally, all included articles’ reference lists will be examined and searched. For grey literature, a manual search and a Google Scholar search were performed. “Prevalence,” “hypertension,” “risk factors,” “predictors,” “HIV,” “HAART,” and “Ethiopia” were the search terms that were used in the entire electronic search strategy. The right Boolean operators (AND, OR) were combined with truncation.
Study Selection
After conducting an online search, two independent reviewers evaluated the abstracts of all the papers that were found. Those that are thought to meet the requirements for inclusion in a systematic review were retrieved in full text for the reviewers’ thorough assessment. At any point during the article selection process, conflicts between reviewers were settled by discussion or, if necessary, by consulting a third reviewer. The reasons for the exclusion of studies at each stage were documented throughout the full-text review.
Condition
Hypertension
Context
In Ethiopia
Population
HIV infected patients
Outcomes
The primary outcomes were the pooled prevalence of hypertension among HIV infected patients and the second variable was factors associated with hypertensive patients.
Data Extraction Process and Main Data Items
We used a pre-piloted, consistent data extraction format to obtain the necessary data from the included papers. Using the Newcastle Ottawa Scale (NOS) data extraction form (SF2), the three reviewers separately extracted the data. 8 During the data extraction process, disagreements were settled by consensus and debate. The following study characteristics were extracted from the included studies: names of the first authors, region, study year, publication year, study design, study setting, participants, sample size, data collection method, response rate, and outcome measures (hypertensive or not and its associated factor).
Inclusion and Exclusion Criteria
The studies included in this review were selected according to predefined criteria, focusing on the study population, exposure, and outcomes of interest. The inclusion criteria for this study were the following: Studies have been performed on HIV patients; Study designs were observational, adult patients whose age greater than 18 years old and ART experience, both published and unpublished articles were included. The exclusion criteria of the study were the following: (1) Studies were conducted on populations other than HIV patients. Studies not conducted in Ethiopia, case reports, commentaries, editorials, reviews, studies not reporting on outcomes of interest, studies with insufficient data for extraction and studies conducted in languages other than English were excluded. All published and grey literature, freely accessible full-text human studies done in Ethiopia, was included.
Three expert appraisers were rigorously evaluated for each study selected for inclusion in the systematic review and meta-analysis to assess its methodology and examine how effectively it addresses potential biases in design, implementation, and analysis. The methodological quality and risk of bias of each included article were assessed by three authors independently using the NOS critical appraisal checklist. 9 Any disagreements during the quality assessment were resolved through discussion involving other co-authors. Studies that scored > 60% on the quality scores were considered good quality scores and were included in the final systematic review and meta-analysis.
Outcome Measurements
Hypertension definitions varied across studies with respect to diagnostic thresholds and measurement procedures. Owing to inconsistent reporting, standardization, or stratified analysis by measurement methods were not feasible, and definitions as reported in the original studies were used.
Statistical Analysis
Data from each original study was extracted using an Excel spreadsheet and subsequently imported into STATA version 17.1 for comprehensive analysis. These meta-analyses were performed for the pooled prevalence of hypertension among people living with HIV and its associated factor in Ethiopia. The meta-analyses were conducted in accordance with PRISMA 2020 guideline methodological recommendation from the Cochrane Handbook of systematic review. 7 A summary table was used to provide a concise description of each primary study. STATA version 17 was used to calculate the pooled prevalence of hypertension among people living with HIV. The fixed-effect model used for pooling prevalence estimates reflects the assumption of common underlying prevalence among ART-treated people living with HIV in Ethiopia, rather than being based solely on statistical tests for heterogeneity. In contrast, random-effects models were applied for pooled association due to substantial clinical and methodological variability across studies in the measurement and reporting of risk factors.
I2 was used to identify heterogeneity between the studies, and the results were displayed graphically as a forest plot with a 95% CI.
The weighted Egger's regression test and funnel plot were used to check for evidence of publication bias, with a p-value of less than 0.05 serving as a cutoff point to declare the presence of publication bias.
Results
Selection Result
Overall, 5906 articles were retrieved from the online database. After being exported to EndNote seven citation manager, 1516 duplications were removed, and 4335 were excluded after title and abstract screening. A total of 55 full articles were assessed for eligibility; 36 were excluded because of outcomes of interest and quality. Finally, 18 articles were included in this systematic review and meta-analysis (Figure 1).

PRISMA flow diagram of study selection for prevalence of hypertension among HIV infected patients in Ethiopia, 2025.
Characteristics of the Included Studies
Eighteen cross-sectional studies with a total of 7828 HIV patients were involved in this review. Among those, five studies were from the Amhara region,10–13 two studies were from Harar,14,15 two were from Addis Ababa, 2 and nine were from the Southern Nations, Nationalities, and Peoples’ Region of Ethiopia,16–22 respectively (Table 1).
Characteristics of Studies Included in the Systematic Review and Meta-Analysis of Hypertension Among People Living with HIV in Ethiopia.

*SNNPE; South Nation Nationality of Ethiopia.
Pooled Prevalence of Hypertension Among People Living with HIV
The pooled prevalence of hypertension among people living with HIV in Ethiopia is 22% (17.0, 28.0). A fixed-effects model was employed to estimate the pooled prevalence, due to the absence of significant heterogeneity observed among the included studies (I2 = 0.00%, p = 0.089) (Figure 2).

Forest plot showing the pooled prevalence of hypertension on people living with HIV in Ethiopia.
Publication Bias and Heterogeneity Test
Publication bias was assessed using a funnel plot and Egger's test for analysis of hypertension among HIV-infected patients in Ethiopia. The funnel plot showed some asymmetry; which could not be suggested strong evidence of publication bias. 23 Despite the statistical significance of Eggers test (p = 0.04), no missing studies were imputed using the non-parametric trim-and-fill procedures. This implies that rather than publication bias, the observed funnel plot asymmetry is probably caused by the significant clinical and methodological variability among studies (Figure 3).

Funnel plot for the prevalence of hypertension on people living with HIV in Ethiopia.
Sensitivity Analysis
We also conducted a sensitivity analysis by removing one study at a time to examine the influence of each study on the pooled result, but no single study influenced the overall pooled prevalence. Removing any single study did not significantly alter the overall pooled prevalence. This confirms that these meta-analysis results are highly stable and not driven by any outlier study (Figure 4).
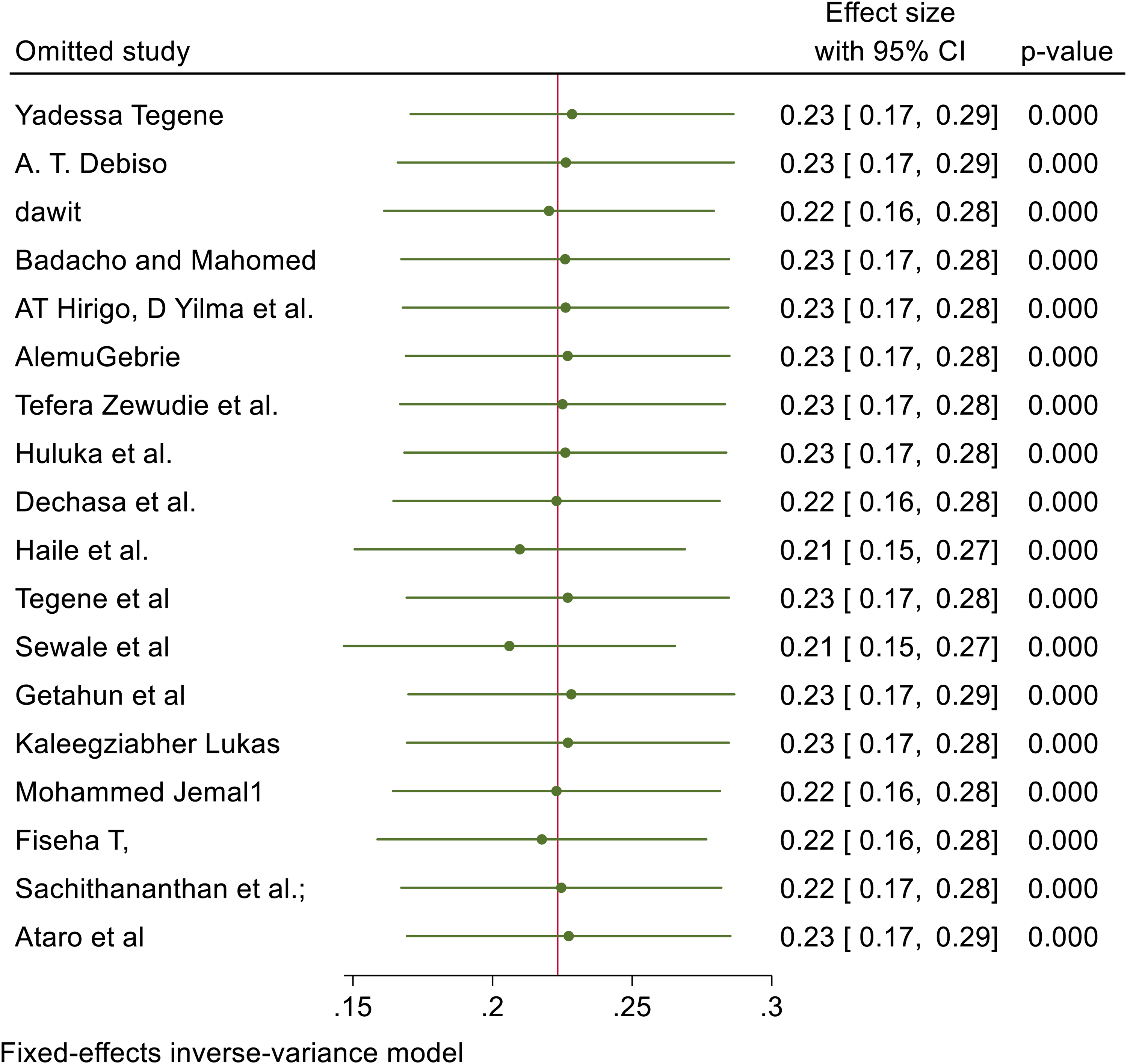
Sensitivity analysis for the study on prevalence of hypertension among HIV infected patients.
Factors Associated with Hypertension on HIV Patients
Patients with physical inactivity had nearly 2.73 times higher odd of having hypertension compared to those who do physical exercise, and this was statistical significant (AOR; 2.73, 95% CI(2.054-4.08)). Eggers test p = 0.0680 suggests no significant publication bias.
Excessive alcohol use was significantly associated with hypertension among patients with HIV; alcohol user more than three times more likely to be hypertensive compared to non-user, AOR (95% CI): 3.012(1.411-4.613). Although a non-parametric trim-and-fill analysis did not impute any missing studies, Egger's test suggested possible publication bias (p < 0.001), indicating that other factors, such as the high heterogeneity (I 2 = 65.68%) among the included studies, may be more responsible for the observed asymmetry (Table 2).
Pooled Factors Associated with Prevalence of Hypertension Among People Living with HIV in Ethiopia.

Meta-Regression for Factors
We conducted meta-regression for factors. Region was the major source of heterogeneity (p = 0.0002) in the association between hypertension and alcohol consumption. Sample size was the source of heterogeneity in the association between physical inactivity and hypertension among people living with HIV (P = 0.01).
Certainty of Evidence (GRADE)
The certainty of evidence for hypertension prevalence among people living with HIV in Ethiopia was rated as moderate, as all included studies were cross-sectional. Study quality, heterogeneity in hypertension definition, and potential publication bias further affects confidence. The certainty of evidence for associated factors including physical inactivity, alcohol use, and ART duration was rated as low, downgraded due to serious risk of bias, heterogeneity, and potential publication bias in some analyses (SF3).
Discussion
This meta-analysis aimed to estimate the pooled prevalence of hypertension among people living with HIV in Ethiopia, and to identify factors associated with it in this population. The pooled prevalence of hypertension was found to be 22% (95% CI: 17.0-28.0), indicating a significant burden of hypertension among people living with HIV in Ethiopia. According to GRADE assessment, the certainty of evidence for prevalence was rated as moderate, primarily downgrading due to cross-sectional design of included studies. The absence of significant statistical heterogeneity increases confidence in the stability of the pooled prevalence estimate. When compared with national estimates in the general Ethiopian adult population, the pooled prevalence of hypertension among people living with HIV (22%) is slightly higher but similar magnitude. Meta-analysis of population studies in Ethiopia report overall hypertension prevalence around 19.6%. 24 People living with HIV may experience an equal to modestly elevated burden, potentially due to combination of HIV related factors (e.g., long-term ART exposure and chronic inflammation) and shared risk factors such as physical inactivity and alcohol use. 25
These findings align with similar studies conducted in sub-Saharan Africa 21.9% and 19.6%3,6 and East Africa 19.75% 5 of people with HIV had hypertension. However, it is lower than studies on systematic review and meta-analysis of hypertension among HIV infected patients in South Africa in 2023 which is 25.5%, 26 globally 25.2%, 27 23.6% 4 and studies on older individuals in South Africa in 2022 50%. 28 These differences may be explained by urbanization, sample size difference, sociodemographic difference, obesity and better detection system of hypertension in South Africa, while life style, demographic, genetic difference, difference ART regimes, dietary pattern, and healthcare access difference might be the reason of discrepancy among the globes.
The funnel plot showed some asymmetry, which was confirmed by statistically significant Egger's test (p = 0.04). This indicates the presence of small study effects. However, the nonparametric trim-and fill method did not impute any missing studies, suggesting that the observed asymmetry may not be solely due to publication bias.
In this meta-analysis excessive alcohol drinking, long duration of ART use and limited physical exercise increase the odds of hypertension among people living with HIV in Ethiopia. In this meta-analysis physical inactivity increases the odds of hypertension among people living with HIV by 2.73; studies carried out in South Africa support this. 5 Lifestyle shifting, urbanization, and limited infrastructure for exercise might be the reason for physical inactivity. Therefore, individuals who do not do regular exercise attributed to the buildup of fat in the tissue and organ, which affects hemodynamic pathway and lead to hypertension. Because of the heterogeneity across the studies, meta-regression and subgroup analysis were performed.
The use of alcohol increases the odds of hypertension among people living with HIV in Ethiopia. Those individuals who drink alcohol are three times more likely to have hypertension than those who do not drink. These findings are in line with other studies.5,29–31 Alcohol raises the body's overall cholesterol levels. Additionally, alcohol lowers nitric oxide, which is crucial for vasodilation, and raises the risk of hypertension.32,33 Alcohol consumption may be linked to cultural practice and a higher prevalence of hazardous use. Another study showed that drinking alcohol doubles the risk of hypertension. 34 Alcohol consumption also affects central nervous system, leading to increase cardiac output, and influence the peripheral vascular system, contributing to elevated blood pressure and hypertension risk. 35 Due to heterogeneity, a meta-regression was performed. The analysis demonstrated that region significantly explains heterogeneity in the association between alcohol use and hypertension among people living with HIV (coefficient=0.84, p = 0.002).
ART duration is substantially associated with hypertension. People who had been undergoing ART for 5 or more years had 2.5-fold higher odds of hypertension among HIV-infected patients. It is supported by similar systematic and meta-analysis studies conducted in East Africa. 5 ART duration effects may reflect specifically the cumulative metabolic effects of ART regimens used locally (eg, older drugs with more pronounced metabolic side effects) or disparities in monitoring and lifestyle, yet it highlights the need for more high-quality longitudinal studies on ART-related cardiovascular risk in Ethiopian PLHIV.
Physical inactivity was significantly associated with hypertension among people living with HIV, with inactive individuals having 2.7 times higher odds. This aligns with studies in Sub-Saharan Africa, where sedentary lifestyle increases arterial stiffens, adiposity, and vascular resistance.36,37 Urbanization and lifestyle changes may contribute inactivity, highlighting the need for integrating regular physical activity into HIV care to reduce hypertension. Due to observed heterogeneity, a meta-regression was performed, which identifies sample size as a significant source of heterogeneity (p = 0.01).
The certainty of evidence for associated factors including physical activity, alcohol consumption and longer ART duration was rated as low. This reflects limitations related to observational design, substantial heterogeneity, and potential publication bias. Therefore, while these associations appear statistically significant, the strengths of evidence supporting causal inference remain limited.
Implications
The Ministry of Health and other stakeholders should create and distribute national guidelines for the management of hypertension in PLHIV. This includes updating clinical protocols, guaranteeing the consistent availability of antihypertensive medications in ART clinics, and allocating resources for integrated service delivery. For clinical practice, there is an urgent need to shift the paradigm in HIV care from a single infectious disease model to a comprehensive chronic care model that addresses non-communicable diseases like hypertension. Healthcare providers must be trained to manage this dual disease burden.
Addressing the rising tide of hypertension among PLHIV is critical for reducing the overall burden of cardiovascular disease and improving the health outcomes and quality of life for this population. Success in this area will contribute to achieving broader national and global health goals related to both HIV and non-communicable diseases.
Conclusions
The study identifies key modifiable risk factors significantly associated with hypertension in this population, including physical inactivity, excessive alcohol consumption, and prolonged duration of antiretroviral therapy (ART) of 5 years or more. This meta-analysis confirms that hypertension is a significant comorbidity among people living with HIV (PLHIV) in Ethiopia, with a pooled prevalence of 22%. The burden is not uniform throughout the country, with higher prevalence seen in urban settings like Addis Ababa and the Amhara region.
Recommendations
Reduce alcohol consumption: Provide counseling and intervention targeting excessive alcohol use among PLHI.
Monitoring long-term ART users: Closely monitor patients on ART for>= 5 years for hypertension.
Limitation of the Study
Establishing causal links between the listed factors and hypertension is limited by the use of cross-sectional research only. The funnel plot asymmetry may also result from clinical or methodological variations among research, even though tests revealed some publication bias. Additionally, estimates for some places were imprecise since they were based on a limited number of studies. Furthermore, certain related factors might have gone unaccounted for because it was unable to account for all possible confounders, such as dietary habits or particular medication regimes.
Supplemental Material
sj-docx-1-jia-10.1177_23259582261444131 - Supplemental material for Prevalence of Hypertension and Associated Factors Among People Living with HIV in Ethiopia: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jia-10.1177_23259582261444131 for Prevalence of Hypertension and Associated Factors Among People Living with HIV in Ethiopia: A Systematic Review and Meta-Analysis by Addisu Simachew Asgai, Tsegaamlak Kumelachew Derse, Desalegn Mitiku Kidie, Yideg Abinew, Tadios Lidetu, Moges Tadesse Abebe and Jenberu Mekurianew Kelkay in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-doc-2-jia-10.1177_23259582261444131 - Supplemental material for Prevalence of Hypertension and Associated Factors Among People Living with HIV in Ethiopia: A Systematic Review and Meta-Analysis
Supplemental material, sj-doc-2-jia-10.1177_23259582261444131 for Prevalence of Hypertension and Associated Factors Among People Living with HIV in Ethiopia: A Systematic Review and Meta-Analysis by Addisu Simachew Asgai, Tsegaamlak Kumelachew Derse, Desalegn Mitiku Kidie, Yideg Abinew, Tadios Lidetu, Moges Tadesse Abebe and Jenberu Mekurianew Kelkay in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-3-jia-10.1177_23259582261444131 - Supplemental material for Prevalence of Hypertension and Associated Factors Among People Living with HIV in Ethiopia: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-jia-10.1177_23259582261444131 for Prevalence of Hypertension and Associated Factors Among People Living with HIV in Ethiopia: A Systematic Review and Meta-Analysis by Addisu Simachew Asgai, Tsegaamlak Kumelachew Derse, Desalegn Mitiku Kidie, Yideg Abinew, Tadios Lidetu, Moges Tadesse Abebe and Jenberu Mekurianew Kelkay in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Abbreviations
Acknowledgements
We would like to thank all the authors of the studies included in this systematic review and meta-analysis.
ORCID iDs
Ethics Approval and Consent to Participate
Ethical approval was not required because this study was a systematic review and meta-analysis based exclusively on previously published data.
Consent for Publication
This was a systematic review and meta-analysis; therefore, consent for publication was not applicable.
Authors’ Contributions
Conceptualization: ASA. Data curation: ASA, DMK. Formal analysis: ASA. Investigation: ASA, TKD. Methodology: ASA, TL. Project administration: MTA, TKD. Software: ASA. Supervision: MTA. Validation: MTA, YA. Visualization: AS, Writing original draft: AS, MTA, DMK, TKD, Writing review & editing: ASA, YA and JMK.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data is provided within the manuscript or supplementary information files.
Supplemental Material
Supplemental material for this article is available online.