
Abstract
Background
The widespread use of antiretroviral therapy (ART) has significantly increased the life expectancy of people living with HIV (PLWHIV). However, this success is accompanied by a growing burden of non-communicable diseases, particularly hypertension, which has emerged as a leading contributor to morbidity and mortality in sub-Saharan Africa. Despite this growing concern, data on the burden and care cascade of hypertension among PLWHIV in routine care settings remain limited in Cameroon.
Objective
To assess the prevalence, associated factors, and care cascade of hypertension among PLWHIV receiving follow-up at Yaoundé Central Hospital in Cameroon in 2024.
Methods
We conducted a cross-sectional descriptive study at the Day Hospital of Yaounde Central Hospital, a national referral center for HIV care. PLWHIV aged ≥21 years and under active follow-up were included. Hypertension was defined as systolic and/or diastolic blood pressure ≥140/90 mm Hg or current use of antihypertensive medication. Logistic regression analyses were performed to identify factors associated with hypertension, including clinical and HIV-related parameters.
Results
A total of 554 participants were enrolled, of whom 74.0% were women, with a mean age of 50.9 years. The overall prevalence of hypertension was 36.8% (95% CI: 32.9-40.9) and was higher among men than women (45.1% vs 33.9%). Among hypertensive individuals (n = 204), 66.7% had initiated antihypertensive treatment, 45.6% were retained in care, and only 22.6% had controlled blood pressure. Factors independently associated with hypertension included longer ART duration (>16 years) (adjusted OR = 1.88; P = .036), WHO clinical stage II at HIV diagnosis (adjusted OR = 1.56; P = .033), and suppressed viral load (<1000 copies/mL), which was paradoxically associated with a higher risk of hypertension (adjusted OR = 0.42 for unsuppressed viral load; P = .041). No significant association was found with ART regimen lines.
Conclusion
Hypertension affects more than one-third of PLWHIV in this urban HIV referral center, yet important gaps persist in treatment initiation, retention, and control. These findings highlight the urgent need for integrated hypertension screening and management strategies within HIV care services in Cameroon to reduce long-term cardiovascular risks.
Plain Lanugage Summary
Why this study matters Thanks to antiretroviral therapy (ART), people living with HIV (PLHIV) are now living longer. However, this success has come with a new challenge: more and more PLHIV are developing chronic diseases like high blood pressure (hypertension) a leading cause of serious health problems in Africa. What the researchers wanted to find out This study aimed to understand how many PLHIV have hypertension, what factors increase the risk, and how well people with high blood pressure are being diagnosed, treated, and monitored. The study was conducted at the Yaoundé Central Hospital, a major HIV referral center in Cameroon. How the study was conducted The study included 554 PLHIV aged 21 years or older, all receiving regular follow-up care. Hypertension was defined as having blood pressure ≥140/90 mmHg or currently taking blood pressure medication. Researchers analyzed clinical and HIV-related data to identify factors linked to hypertension. What the study found About 1 in 3 participants (36.8%) had hypertension. Hypertension was more common in men (45.1%) than in women (33.9%). Among those with hypertension: 67% had started treatment, Only 46% remained engaged in care, And just 23% had their blood pressure under control. Those with hypertension tended to be: Older (average age: 55 vs. 40 years), On ART for longer periods (16 vs. 6 years), More likely to have had WHO clinical stage II at the time of HIV diagnosis. There was no significant link between hypertension and either ART regimen or viral load. Why this is important A large number of PLHIV also suffer from hypertension, but very few are successfully treated and controlled. This study highlights the urgent need to integrate routine hypertension screening and management into HIV care in Cameroon especially for older patients and those on long-term ART.
Introduction
The global fight against Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) remains a public health priority. In 2023, more than 38 million people living with HIV (PLWHIV) were recorded worldwide, with significant disparities between regions. Sub-Saharan Africa (SSA) remains the most affected, accounting for nearly 70% of all cases. 1 Thanks to advances in antiretroviral therapy (ART), the quality of life for PLWHIV has improved. Since 2005, HIV-related morbidity and mortality have decreased by 35% globally and by 39% in SSA. However, the increased life expectancy of PLWHIV has led to a rise in cardiovascular diseases, related to the chronicity of HIV, conventional risk factors for hypertension, the duration of ART, and challenges in hypertension prevention among PLWHIV in developing countries.2–8
Hypertension, the leading risk factor for mortality worldwide, is a growing problem among adults living with HIV.9–11 Adults living with HIV on ART have a higher prevalence of hypertension than those not living with HIV. 12 A recent meta-analysis of global data showed that 35% of all adults living with HIV on ART suffer from hypertension, compared to about 30% of HIV-negative adults. 13 Among those on ART over the age of 50, more than 50% have hypertension. 14
In Cameroon, hypertension prevention is not systematically integrated into HIV care programs. Nevertheless, several hypertension prevention initiatives are available. These include the LeDEA project (International epidemiology Databases to Evaluate AIDS), 15 and the VIHeillir Project (“VIHeillir” combines the French words for HIV (“VIH”) and aging (“vieillir”)) 16 which address interventions in certain areas of Cameroon. Care for PLWHIV is generally provided in specialized clinics, while patients with non-communicable diseases (NCDs) receive treatment in general medicine services. Unfortunately, there is little overlap in the management of HIV and NCDs, particularly regarding hypertension. This rigid separation limits the understanding of the true burden of NCDs among PLWHIV. Moreover, the lack of integration between HIV care services and those dedicated to NCDs results in a lack of data on access to hypertension treatment and outcomes among PLWHIV in Cameroon. Yet, this information is essential for effectively allocating resources and developing strategies and therapeutic programs that integrate HIV and hypertension management. Therefore, our study aims to establish the situation as far as hypertension management cascade (screening, diagnosis, initiation of treatment, retention, and control) and identify predictive factors among PLWHIV attending Yaoundé Central Hospital.
Materials and Methods
Study Design
This was a descriptive cross-sectional study, a study design particularly suited for determining the epidemiological distribution of a health problem at a specific point in time, especially in resource-limited settings.17,18 Data collection took place over a period of 5 months, from January to May 2024. Preliminary data were extracted from medical records and triangulated with clinical follow-up registers. These included: the clinical stage of HIV, the ART regimen, the patient's age, the duration of ART, treatment adherence, co-infections, the known hypertensive status, and use of anti-hypertensive medications. Blood pressure (BP) measurements were taken during HIV follow-up visits or at appointments for BP control. These BP values were collected over the past 3 months from medical records and clinical registers, reflecting a common time frame used to assess short-term BP control. Although this 3-month period provides a useful snapshot of hypertension management, it may not capture long-term variability or seasonal changes in BP. Patients typically attend appointments every 1 to 3 months depending on their clinical status, which aligns with the period during which BP measurements were recorded. This schedule allows regular monitoring of both HIV and hypertension. Adherence was assessed through triangulation of data from medical records, clinical follow-up registers, and self-reported responses regarding regular intake of antihypertensive medications. A pre-tested questionnaire was administered to each patient who provided informed consent. Hypertension control was defined based on these recorded BP measurements, with patients considered controlled if their systolic and diastolic BPs were below internationally accepted thresholds (commonly <140/90 mm Hg), according to local clinical protocols. A research assistant, a master's student in Public Health and Epidemiology, was responsible for data verification and data entry into KoboCollect. 19 Statistical analyses were performed using SPSS, and graphical illustrations were generated using Excel 2020. The reporting of this study conforms to the EQUATOR cross-sectional reporting guidelines 20 (Supplemental Material: Equator checklist).
The questionnaire used in this study underwent a 3-level validation process. First, it was peer-reviewed by the co-authors of the study. Second, it was evaluated by the academic faculty of the Faculty of Medicine at the University of Dschang during the protocol's academic approval. Finally, it was reviewed by the medical team at the Day Hospital and the Cardiology Department. In addition, a pilot test was conducted during the first week of data collection on a sample of 10 PLHIV. The results of this pretest allowed for adjustments to be made, particularly regarding questions on treatment adherence and hypertension control among PLWHIV.
Study Settings
The study took place at the Yaounde Central Hospital (YCH), a secondary-level hospital and a dedicated infectious diseases unit. YCH is an ANRS site, regularly hosting innovative research projects. The health unit involved in this study was the Day Hospital Service (DHS). Created in 1997 and inaugurated in 1998, the DHS was the first fully operational department of the Yaoundé Central Hospital. It is a pilot service in Cameroon, providing care for PLWHIV. It offers information and diagnosis-raising services (on STIs and HIV in particular), HIV screening, and various consultations (dermatology, STIs, general medicine, etc). It also offers support for medical students working on their theses. We chose this facility because it had the largest and longest-standing number of “treatment adherent” PLWHIV in Cameroon. There are currently more than 12 000 patients in the follow-up file.
Selection Criteria for Participants
All PLWHIV aged 21 years and older followed up at YCH were eligible for the study. Inclusion criteria included having an up-to-date medical record, giving informed consent, and being followed at the Day Hospital. Pregnant women were excluded due to the physiological changes and specific adaptations related to pregnancy, which can affect BP and hypertension management, making direct comparison with the general population difficult. Similarly, patients who had initiated ART less than 6 months prior to the study were excluded to avoid biases related to the initial treatment phase, during which BP effects and treatment adherence may not yet be stabilized. Excluded participants were pregnant women, those who withdrew consent during the study, those initiated on ART within 6 months prior to the study, and those without complete and updated medical records.
Sampling Method and Minimum Sample Size
PLWHIV/AIDS who were followed at the day hospital and who met the inclusion criteria were recruited by a consecutive sampling of PLWHIV and their medical records during the study period. It is a non-probabilistic method in which patients are selected based on their availability or accessibility. It is useful in our situation, as specific participants are difficult to access due to the dispersion of the population. To minimize selection bias inherent in consecutive sampling, we included all eligible participants presenting during the study period, regardless of clinical condition or ART duration. Equally, according to their follow-up calendar, most eligible patients visited the center once after every 1 or 2 months, from diverse areas. We ensured consistency in eligibility criteria and maintained a clear enrollment log.
The minimum required sample size for this study was estimated using the standard formula for calculating sample size when estimating a proportion in a population:

The minimum sample size required was therefore 289 participants. Considering a potential non-response or exclusion rate of 30%, the sample size was adjusted to 386 participants. To improve statistical power and increase the precision of our estimates, data was ultimately collected from 586 participants.
Blood Pressure Measurement
BP was measured during routine HIV care visits by trained epidemiological research assistants using validated automated monitors and following a standardized protocol. After a 5-min rest, BP was measured systematically. An OMRON M3 HEM-7131-E (Omron Healthcare Co Ltd, Kyoto, Japan) electronic BP monitor was used, following guidelines defined by the PanAfrican Society of Cardiology for achieving 25% hypertension control in Africa by 2025 23 (Figure 1).

PASCAR Recommendations for Blood Pressure Measurement, Thresholds, and Action Required Following Appropriate Office Measurement.
To ensure consistency and minimize measurement errors, we used a single validated automatic device for all BP measurements throughout the study. This approach reduced calibration differences and device-related variability that could arise from using multiple instruments. A standard operating procedure was available to guide BP measurement, and health personnel were uniformly trained to reduce inter-observer variability. Two BP readings were taken 1-2 min apart, and the average of the last 2 measurements was used in the analysis.
Body mass and height were measured using standardized equipment: body weight in light clothing was recorded to the nearest 100 g using a Medisina scale (Seca, Hamburg, Germany), and height to the nearest 0.1 cm with a stadiometer. Body Mass Index (BMI) was then calculated as weight (kg) divided by height squared (m²).
Definition of Outcomes
The outcome variable of interest in this study was hypertension. Hypertension was defined according to the Pan African Society of Cardiology (PASCAR) as (1) documented and confirmed hypertension, (2) current antihypertensive treatment, or (3) systolic BP ≥140 mm Hg and/or diastolic BP ≥90 mm Hg on at least 2 occasions 1 month apart, or documented use of antihypertensive medication or history of hypertension. HTN was further classified as follows : optimal (SBP <120 mm Hg and DBP <80 mm Hg), normal (SBP 120-129 mm Hg and/or DBP 80-84 mm Hg), high normal (SBP 130-139 mm Hg and/or DBP 85-89 mm Hg), grade 1 HTN (SBP 140-159 mm Hg and/or DBP 90-99 mm Hg), grade 2 HTN (SBP 160-179 mm Hg and/or DBP 100-109 mm Hg), grade 3 HTN (SBP ≥180 mm Hg and/or DBP ≥110 mm Hg), and isolated systolic hypertension (SBP ≥140 mm Hg and DBP <90 mm Hg). 23
In this study, for newly suspected cases, a second confirmatory measurement was taken 1 month later during a follow-up visit. When 2 separate measurements were not available, a single elevated value combined with ongoing treatment or a documented diagnosis in the medical record was considered sufficient.
Data Collection
In this study, data were collected using a digital form via KoboCollect. The collected data included the sociodemographic characteristics of participants (age, sex, employment status, marital status), weight, height, and general cardiovascular risk factors (alcohol and drug consumption, physical activity). After administering the questionnaire, a further review of medical records was conducted to complete the form with previous BP values from the past 3 months, the treatment regimen, viral load, HIV/AIDS diagnosis stage, specific ART regimens, viral load and the diagnosis and treatment initiation dates for both HIV/AIDS and hypertension, as well as hypertension treatment adherence.
Statistical Analysis
The crude prevalence of HTN was calculated among study participants with available BP measurements, while the proportion receiving treatment was calculated among all hypertensive participants, and the proportion with controlled BP was calculated among those receiving treatment.
Data was processed using Excel and analyzed with MS Excel and SPSS 23. Descriptive statistics were employed to describe participant characteristics. Categorical variables were reported as frequencies and percentages, while continuous data were summarized using appropriate measures of central tendency. Hypertension prevalence was calculated among participants with available BP measurements. Although the prevalence of hypertension was high in this population, a logistic regression model was used because the objective was to explore associations between predictors and the odds of hypertension, not to estimate risk ratios directly. However, we acknowledge that odds ratios may overestimate effect sizes in the case of common outcomes. Logistic regression models were applied to measure the association between predictors and hypertension, with odds ratios (OR) and 95% confidence intervals (CI). The significance level was set at P < .05. Multivariable models were adjusted for key confounders such as age, sex, and other relevant covariates to ensure robust estimates of association. Only variables with a P-value < .02 in the bivariate analysis or with strong biological plausibility were included in the multivariable model.
Results
Out of the 4865 patients who visited the Day Hospital during the study period, 586 participated in the study. Among these, 554 participants (94.6%) were included in the analysis, while 32 (5.4%) were not included due to incomplete data (Figure 2).
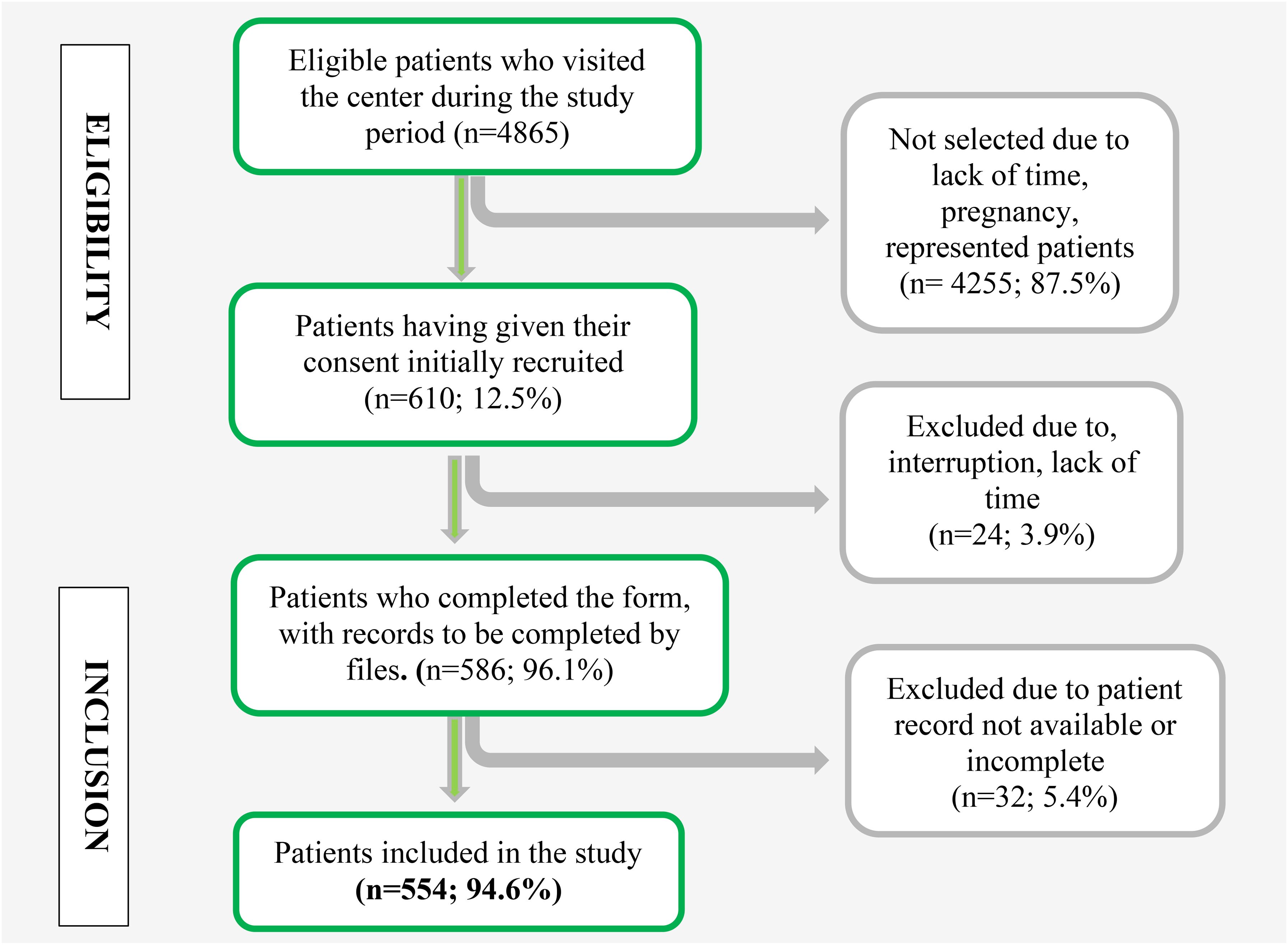
Enrolment Flow Chart of Participants in the Study at YCH, 2024.
Sample Description
Tables 2 and 3 present the distribution of participant characteristics according to hypertension status and are also stratified by sex (female vs male), to better capture potential gender-related differences. Among the 554 participants included in this study, majority were women (74%). The age ranged from 20 to 82 years, with an average of 50.9 years (P-value = 0.800) indicating a relatively older population. Table 1 presents the distribution of participants’ characteristics overall and according to hypertension status.
Socio-Demographical Characteristics of Participants.

Continuous variables are presented as means with standard deviations (SD) and were compared between groups using the Student's t-test for normally distributed data or the Mann–Whitney U test for non-normal distributions, based on the Shapiro–Wilk normality test. Categorical variables are presented as absolute counts and percentages and were compared using the Chi-square (χ²) test or Fisher's exact test when expected cell counts were less than 5. A 2-tailed P-value of less than .05 was considered statistically significant.
Abbreviations: n (%), frequency (percentage); SD, standard deviation; HTN, hypertension.
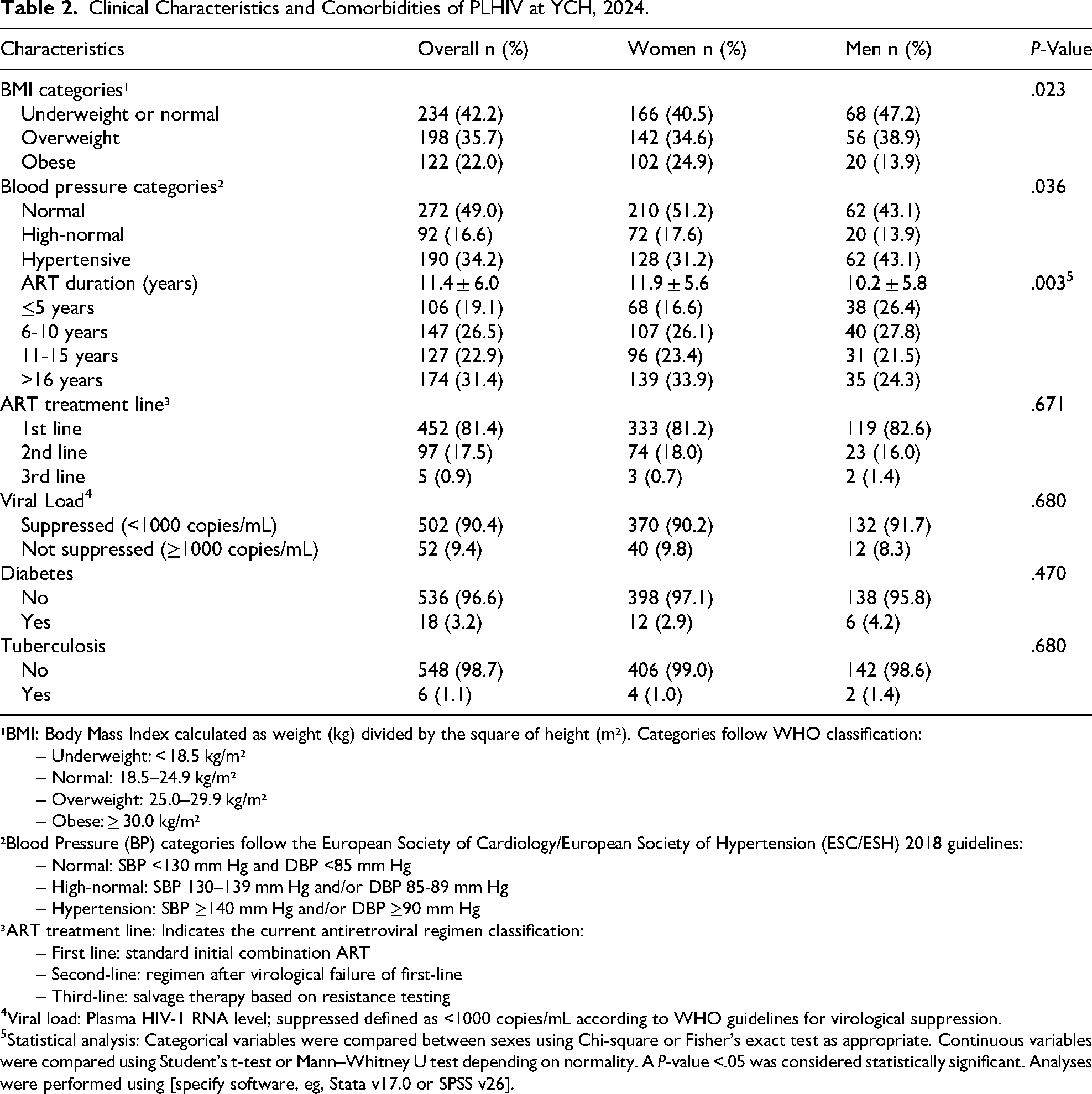
Clinical Characteristics and Comorbidities of PLHIV at YCH, 2024.
¹BMI: Body Mass Index calculated as weight (kg) divided by the square of height (m²). Categories follow WHO classification:
– Underweight: < 18.5 kg/m²
– Normal: 18.5–24.9 kg/m²
– Overweight: 25.0–29.9 kg/m²
– Obese: ≥ 30.0 kg/m²
²Blood Pressure (BP) categories follow the European Society of Cardiology/European Society of Hypertension (ESC/ESH) 2018 guidelines:
– Normal: SBP <130 mm Hg and DBP <85 mm Hg
– High-normal: SBP 130–139 mm Hg and/or DBP 85-89 mm Hg
– Hypertension: SBP ≥140 mm Hg and/or DBP ≥90 mm Hg
³ART treatment line: Indicates the current antiretroviral regimen classification:
– First line: standard initial combination ART
– Second-line: regimen after virological failure of first-line
– Third-line: salvage therapy based on resistance testing
4Viral load: Plasma HIV-1 RNA level; suppressed defined as <1000 copies/mL according to WHO guidelines for virological suppression.
5Statistical analysis: Categorical variables were compared between sexes using Chi-square or Fisher's exact test as appropriate. Continuous variables were compared using Student's t-test or Mann–Whitney U test depending on normality. A P-value <.05 was considered statistically significant. Analyses were performed using [specify software, eg, Stata v17.0 or SPSS v26].
Distribution of Patients at Stages I, II and III of HTN at YCH, 2024.

Among the participants, 35.74% had a high BMI, and 22% were classified as obese. More than half of the patients had been on ART for over 10 years, with 81.4% of them receiving the TDF/3TC/DTG, the only first line regimen available during the data collection period. After reviewing medical records, it was found that 3.25% of the participants had a history of diabetes, and 1.08% had a history of tuberculosis (Table 2).
Stages of Hypertension
The classification of BP among participants reveals that the majority had normal BP (52%, 95% CI: 44.95-52.89). A smaller proportion fell into the high-normal category (11%, 95% CI: 0.84-14.07). Regarding hypertension grades, Grade I was the most represented (19.49%, 95% CI: 18.77-25.81), followed by Grade II (13.8%, 95% CI: 10,61-16.06) and Grade III (4.15%, 95% CI: 2,78-6,15). These results indicate that most hypertensive participants were in the early stages of the disease, which underlines the importance of timely detection and management to prevent progression to more severe stages (Table 3).
Prevalence of Hypertension Among PLWHIV
The overall prevalence of hypertension was 36.8% (204) (<0.001). Of these, 21.57% did not respond affirmatively to the question “Are your hypertensive?” which means 1 person out of 5 was not aware they had hypertension. Among these cases the awareness rate was 78.4% meaning 1 out of 5 people were ignorant about their hypertension status. The frequency of hypertension was higher among men with 45.14% [95% CI: 36.8-53.6] as compared to women with 33.9% [95% CI: 61.4-70.2]. Many patients with hypertension were aged ˃40 years, representing overall 95.1% [81.1-109.3], which shows that older patients frequently had hypertension compared to the younger patients <40 years represented by 4.90% [2.4-8.8]. Also, the results indicate that over half of the cases 49.5% [42.2-56.8] were at Grade I of hypertension (Figures 2 and 3).
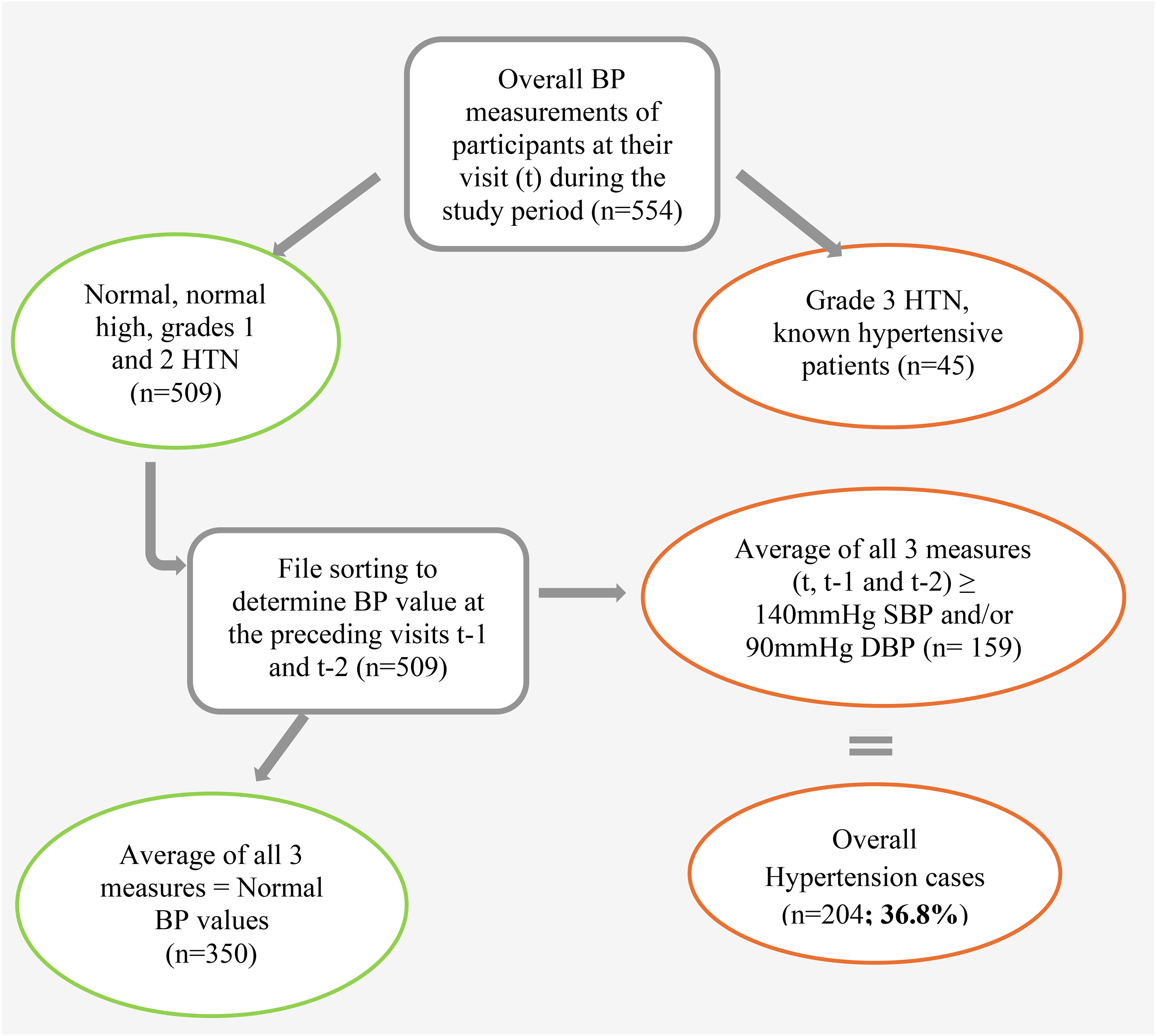
Flow Chart for Prevalence Determination of Hypertension Among PLHIV at YCH, 2024.
Hypertension Care Cascade of PLWHIV
The Hypertension Care Cascade (Figure 4) highlights the steps involved in managing hypertension among PLWHIV/AIDS. The cascade reveals a significant drop in care coverage at each stage.

Hypertension Care Cascade of PLHIV at YCH, 2024.
Risk Factors of Hypertension
In this study, duration on ART, viral load suppression status, and HIV clinical stage at diagnosis were independently associated with hypertension among PLHIV. Participants who had been on ART for more than 16 years had significantly higher odds of hypertension compared to those on ART for 5 years or less (adjusted OR [aOR] = 1.88; 95% CI: 1.04-3.38; P = .036), highlighting a cumulative effect of long-term ART exposure. Interestingly, having an unsuppressed viral load (≥1000 copies/mL) was associated with a significantly lower likelihood of hypertension (aOR = 0.42; 95% CI: 0.18-0.97; P = .041), which may reflect a lower cumulative exposure to ART, possible weight loss in advanced disease stages, or residual confounding. Additionally, participants diagnosed at WHO clinical stage II had higher odds of hypertension compared to those at stage I (aOR = 1.56; 95% CI: 1.04-2.33; P = .033), suggesting that intermediate-stage immunosuppression might be linked to increased cardiovascular stress. No significant associations were found between hypertension and ART regimen lines in the adjusted analysis. These findings underscore the importance of integrating cardiovascular risk screening into long-term HIV care, particularly for patients with sustained ART exposure and virologic suppression (Table 4).
Risk Factors for Hypertension Among PLHIV.

Abbreviations: n (%), frequency (percentage); OR, odds ratio; P-value, probability value; SD, standard deviation; ART, antiretroviral therapy.
- A P-value < .05 was considered statistically significant.
Discussion
This study was the first to be conducted in the oldest and largest care center for PLWHIV/AIDS in Cameroon. It aimed to describe the epidemiological distribution of hypertension prevalence, treatment, control, and associated risk factors. Our findings reveal a high hypertension prevalence (36.8%) in the studied population, aligning with existing literature, which reports prevalence rates ranging from 8% to 45.9% across Africa. 24 This result is also comparable to that of a single-site study conducted in the Northwest region of Cameroon in 2019, which found a prevalence of 36.4% (95% CI: 30.15%-43.10%). 25 However, our prevalence is notably higher than that reported in a more recent 2022 study in Cameroon, which found 23.9% (95% CI: 22.2-25.6%) among PLWHIV. 26 The disparity may primarily be attributed to differences in study populations, particularly ART duration, as the latter study included only participants with ART exposure of ≤4 years.
This monocentric study, conducted in a referral hospital, may introduce selection bias by overrepresenting patients with more severe disease, thus limiting the generalizability of the findings. Moreover, the cross-sectional design of the study prevents establishing causal relationships, particularly between the duration of ART and hypertension.
Nevertheless, other single-site studies conducted in Africa between 2021 and 2024 have reported lower hypertension prevalence, such as Uganda (24.3%), Tanzania (19.6%), Kenya (18.9%), Zambia (18.0%), and Ghana (17.4%)27–31. These discrepancies may be explained by variations in genetic predispositions, socioeconomic conditions, ART regimens, and, importantly, methodological differences across studies. Variability in inclusion criteria, BP measurement techniques, and study populations may significantly contribute to these variations.
Regarding the hypertension care cascade, while screening rates were relatively high (100%), a significant drop was observed in subsequent stages: 36.82% were diagnosed with hypertension, 66.67% of diagnosed cases-initiated treatment, 45.59% of those treated remained on therapy, and only 22.58% achieved BP control. A 2023 systematic review analyzing hypertension treatment and control among PLWHIV in SSA highlighted even lower awareness rates (1.3%-52.9%) compared to our study (78.4%). Like our findings, this review also reported a substantial variability in treatment initiation rates, ranging from 1.2% to 83.0%. Additionally, it emphasized the widespread challenge of suboptimal hypertension control, with control rates peaking at just 24.3%. 1 These findings underscore persistent barriers to effective NCD management among PLWHIV in resource-limited settings.
In multivariable analysis, ART duration and HIV clinical stage (stage II) emerged as significant predictors of hypertension, even after adjusting for confounding factors like age and gender. The association between longer ART exposure and increased hypertension risk aligns with prior research, which has demonstrated the long-term cardiovascular effects of ART.7,11,32,33 Interestingly, our study identified HIV clinical stage II as a significant predictor of hypertension, contrasting with findings from a study in Burundi that associated hypertension with clinical stages III and IV. 34 Our finding that WHO Stage II was positively associated with hypertension is unexpected, as more advanced stages typically indicate higher disease burden. One possible explanation is survivorship bias as those in advanced stages may have higher mortality and thus be underrepresented. Another possibility is that patients with earlier-stage disease-initiated ART sooner, allowing time for chronic NCDs to emerge. Also, we found no significant association between hypertension and ART regimen or viral load, a result consistent with previous systematic reviews and meta-analyses, which have also reported an absence of direct associations between these factors and hypertension.4,35–37 Dolutegravir, this integrase strand transfer inhibitor (INSTI)-based regimen, widely used in first-line ART regimens, has been associated with weight gain, a known risk factor for hypertension. Earlier research has suggested that prolonged use of Dolutegravir is associated with overweight due to altered fat distribution and metabolic changes, potentially elevating hypertension risk.27,38–41 Although we could not assess ART regimens directly, the predominance of Dolutegravir-based therapies in our setting suggests a potential contributory role in the hypertension burden, calling for further investigation.
Interpretation of our findings requires careful consideration of several limitations. Firstly, we encountered high levels of missing data for key parameters influencing hypertension status, such as WHO clinical stage, creatinine, and hemoglobin levels. Also, CD4 count data and specific ART regimen histories were not available for all participants. This limited our ability to fully assess immunosuppression and ART-related risk factors. However, previous studies have suggested that advanced HIV disease (WHO stages III/IV, low CD4 count, and anemia) may confer some level of protection against hypertension, making this a relevant area for further investigation. 4 Secondly, the single-site nature of our study limits generalizability as YCH is a single tertiary referral hospital, which may disproportionately serve patients with more advanced or complex health needs. This could bias the prevalence estimates of hypertension upward. However, given that our study center is the largest and oldest HIV care facility in Cameroon, serving patients from across the country, our findings remain highly relevant. Thirdly, given the cross-sectional nature of this study, we cannot infer causality between exposure variables (eg, duration on ART) and hypertension outcomes. Temporal relationships remain speculative and require longitudinal analysis. Also, hypertension screening rates in routine clinical settings could not be directly assessed, as all study participants underwent BP measured for prevalence determination. Additionally, reliance on self-reported data for certain variables may have introduced recall bias, particularly concerning treatment retention. Lastly, our study would have benefited from a comparative analysis with hypertension data from the general population to better contextualize the burden among PLWHIV.
Despite these limitations, our study has several strengths. The use of digital data collection tools enhanced accuracy and efficiency. Furthermore, by detailing the hypertension care cascade, we identified critical intervention points where targeted measured could improve outcomes. Lastly, our findings contribute to the growing body of literature on hypertension among PLWHIV in Cameroon, addressing an important research gap and providing valuable insights for public health decision-making.
Conclusion
This study reveals that one-third of PLWHIV had hypertension and those who had been on ART for more than 15 years were 1.9 times more at risk than others. Despite efforts at the screening step, the prevention of hypertension in this high-risk population is poorly organized. Among PLWHIV, the risk factors for hypertension include HIV-specific factors such as the stage of diagnosis for HIV/AIDS and the estimated duration of exposure to ART. Our findings equally highlight the need to fully integrate hypertension management into routine HIV care. Strategies may include training of nurses, the improvement on accessibility of integrated care protocols, and regular BP monitoring during ART follow-up visits in all HIV/AIDS care units to enhance early detection and management of hypertension. Therefore, it is imperative to collaborate with healthcare professionals to evaluate and address the elements responsible for insufficiency of hypertension care among PLWHIV with hypertension.
Limitations
This single-center, cross-sectional study has limited generalizability, as participants from Yaoundé Central Hospital may present more complex health profiles. The association observed between ART duration and hypertension cannot imply causality and may be influenced by confounding. Longitudinal studies are needed to confirm these findings.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251378538 - Supplemental material for Hypertension Burden and Care Cascade Gaps Among People Living With HIV in an Urban HIV Clinic in Cameroon 2024
Supplemental material, sj-docx-1-jia-10.1177_23259582251378538 for Hypertension Burden and Care Cascade Gaps Among People Living With HIV in an Urban HIV Clinic in Cameroon 2024 by Charles Kouanfack, Francis Duhamel Nang Nang, Rita Marie IFOUE NGUIMFACK, Liliane Kuate Mfeukeu, André Pascal Kengne, Paul Junior Chebo, Jean Pierre Junior Tchitetchoun, François Anicet Onana Akoa, Fabrice Djouma Nembot, Anastase Dzudie and Simeon Pierre Choukem in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251378538 - Supplemental material for Hypertension Burden and Care Cascade Gaps Among People Living With HIV in an Urban HIV Clinic in Cameroon 2024
Supplemental material, sj-docx-2-jia-10.1177_23259582251378538 for Hypertension Burden and Care Cascade Gaps Among People Living With HIV in an Urban HIV Clinic in Cameroon 2024 by Charles Kouanfack, Francis Duhamel Nang Nang, Rita Marie IFOUE NGUIMFACK, Liliane Kuate Mfeukeu, André Pascal Kengne, Paul Junior Chebo, Jean Pierre Junior Tchitetchoun, François Anicet Onana Akoa, Fabrice Djouma Nembot, Anastase Dzudie and Simeon Pierre Choukem in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We extend our sincere gratitude to all individuals who contributed, directly or indirectly, to the completion of this work. We are particularly grateful to the healthcare staff of the Day Hospital, where our study was conducted, for their guidance and encouragement. We also wish to acknowledge the people living with HIV who participated in the study without any financial compensation, as this research was conducted as a student project without external funding. Our appreciation goes to the teaching staff of the Faculty of Medicine and Pharmaceutical Sciences at the University of Douala for the knowledge and expertise they imparted, as well as to the non-teaching staff of the faculty for their unwavering support.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of the Regional Ethics Committee for Human Health Research in the Central Region (CRERSHC)
Author Contributions
FDNN, APK, JPJ T, CK, SPC, and AD designed the study. FDNN, JPJT, PJC, RMI, FAO, and FDN contributed to the overall study conduct and data collection. FDNN, FDN, FAO, CK, and APK idealized and performed data analysis. FDNN and APK drafted the manuscript. All coauthors had full access to the data, reviewed the final version of the manuscript, and accepted responsibility for submission for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The individual participant data underlying the findings of this article (including text, tables, figures, and supplemental materials), accompanied by a detailed data dictionary, are the intellectual property of the research team. This data will be made available at reasonable requests to researchers whose proposals have been approved by the study's principal investigators. The findings will be formally presented during the PhD thesis defense in Epidemiology at the University of Dschang. In addition, results have been communicated to the authorities of the Yaoundé Central Hospital, and key messages have been displayed in the Day Hospital unit as part of a preventive health initiative. Proposals should be directed to francduhamelnang@yahoo.com. Access to the data will require the signing of a data use agreement.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.