
Abstract
Objectives
To explore the association between family relationships and quality of life (QoL), and the mediating role of resilience among people living with HIV (PLWH) and their family members (FMs).
Methods
Baseline data were drawn from an ongoing study in Guangxi, China, including 783 PLWH-FM dyads. The actor-partner interdependence mediation model examined how individuals’ family relationships/cohesion affect their own (actor effects) and their partners’ QoL (partner effects), and the mediating role of resilience.
Results
A significant actor-direct effect was observed for FMs’ family relationships on their own mental QoL (β = 0.136, P < 0.001), while no such effect was found for PLWH. Resilience functioned as a mediator between PLWH's family cohesion and PLWH's QoL (physical: β = 0.109, mental: β = 0.089, P < 0.001) and between FMs’ family relationships and FMs’ QoL (physical: β = 0.062, mental: β = 0.075, P < 0.001). Regarding partner effects, FMs’ resilience mediated the association between PLWH's family cohesion and FMs’ QoL (physical: β = 0.036, mental: β = 0.044, P < 0.01).
Conclusion
Findings underscore that future interventions should target the family as a unit to strengthen family ties and improve the cross-dyadic role of resilience, particularly that of FMs.
Plain Language Summary
Families play a central role in the lives of people living with HIV (PLWH). Supportive family relationships can help individuals cope with stress, stay healthy, and maintain a good quality of life. However, we still have limited understanding of how family relationships shape the well-being of both PLWH and their family members, and whether resilience—the ability to adapt and stay strong during challenges—helps explain these connections.
In this study, we adopted the baseline data of an ongoing cohort study including 783 pairs of PLWH and one of their family members in Guangxi, China. We wanted to better understand how each person's perception of their family relationships or cohesion was linked to their own well-being, and also whether it affected their partner's well-being. We also examined whether resilience played an important role in these relationships.
Our results showed that family members who felt they had strong, positive family relationships tended to report better mental and physical well-being. We also found that resilience helped explain how good family relationships led to better physical and mental health for both PLWH and their family members. Additionally, the resilience of family members played a role in connecting PLWH's family relationships to the family members' own well-being.
These findings show that HIV affects not just individuals, but entire families. Strengthening family relationships and helping both PLWH and their family members build resilience may improve their overall well-being. Interventions that focus on the family as a unit—not just the individual living with HIV—may be especially helpful in supporting long-term health and quality of life in HIV-affected families.
Introduction
The global HIV epidemic remains a significant public health concern, not only due to its physiological consequences but also because of its profound psychological impact on people living with HIV (PLWH) and their families. 1 With the success of antiretroviral therapy (ART) in prolonging the lives of PLWH, the focus of HIV care has also expanded to their quality of life (QoL). QoL, encompassing physical, psychological, and social well-being dimensions, has been regarded as an important indicator for assessing the impact of disease diagnosis and subsequent treatments. 2 Improving QoL is now a major priority for researchers and a key component of UNAIDS's 2030 Global AIDS Strategy.3–5 Romijnders et al interviewed 29 PLWH and 13 participants without HIV from key populations (ie, men who have sex with men [MSM]) and found that PLWH reported a lower level of QoL than those without HIV. 6 This finding is supported by cross-sectional and prospective longitudinal studies that consistently show reduced QoL among PLWH.4,7 QoL of PLWH is not only influenced by PLWH themselves, but also by their family members (FMs). Determining QoL-associated factors is therefore essential for understanding the lived experiences of PLWH and their families and for informing interventions aimed at improving well-being in the context of chronic HIV management. 8
FMs play an essential role in disease management for PLWH by providing daily care and emotional support to PLWH.9,10 This caregiving role, coupled with fear of HIV transmission and the ongoing burden of care, may disturb FMs’ daily routines and further contribute to poor life satisfaction and worsen QoL among FMs. 11 Given the interdependent nature of mental health within HIV-affected families, the diagnosis of HIV and subsequent therapies have been viewed as stressful experiences that diminish life satisfaction and negatively affect the QoL of PLWH and their FMs.1,12 Studies with dyads data that include both PLWH and their FM could provide a comprehensive perspective to inform family-centered interventions that can effectively enhance QoL of HIV-affected families.
Existing studies emphasize that HIV infection, as a shared familial experience, reciprocally affects both PLWH and FMs’ perceived family relationships and QoL.1,13 As a crucial dimension of family relationships, family cohesion refers to the emotional bonding and togetherness that FMs have toward one another. 14 According to current research, the HIV/AIDS epidemic has profoundly affected the composition and dynamics of families,15,16 which has a detrimental effect on family cohesion, leading to poor QoL in both PLWH and their FMs.17,18 Previous studies conducted in China examined the association between family-related factors and QoL and found that lower QoL among PLWH was due to their limited social networks and family support.19,20 In addition, long-term caregiving burden and social discrimination caused FMs of PLWH to have poor family bonding and intensive family relationships, which further influenced their psychological and physical well-being. 21 Although existing studies individually focus on the impact of family relationships on PLWH and FMs’ QoL, limited attention has been paid to its impact on both PLWH and their FMs, and the potential mechanism behind these relationships from a dyadic perspective.
The dyadic relationship between family cohesion/relationship and QoL among PLWH and their FMs could be mediated by individual/family coping strategies, such as resilience. As a modifiable individual psychological capacity, resilience is defined as a dynamic process wherein an individual presents a positive adaptation to stress, crisis, and adversity. 22 Within PLWH, Xu et al found that increased family support was positively associated with QoL through improving resilience among older PLWH. 19 However, this study only included PLWH, ignoring the effect from FMs. According to the Circumplex model of marital and family systems, the process of coping with stressors and adversity is not a simple process in which individuals leverage their own advantages in isolation; rather, it is a process involving the adaptation of the entire family system.23,24 This theory assumes that low levels of cohesion and flexibility are associated with dysfunctional family systems functioning. 24 Thus, it is possible that a cohesive family could increase the resilience of both PLWH and their FMs, which further contributes to enhanced QoL for both parties. According to the literature review, however, the majority of HIV resilience research defines resilience only at the individual (ie, psychological) level and limits interpersonal resilience (eg, social support), such as resilience from FMs. 25 Although resilience may serve as a mediator in the relationships between family cohesion and QoL among patients and their FMs, little is known about how resilience works in dyadic relationships, specifically between PLWH and their family caregivers.
According to the interdependence theory, interactions between individuals in a close relationship have an effect on their respective partners’ outcomes. 26 This theory directly provided a theoretical foundation of the actor-partner interdependence mediation model (APIMeM), an extension of the actor-partner interdependence model (APIM). APIMeM is designed to examine both intrapersonal (actor) and interpersonal (partner) effects as well as the potential mediators in dyadic relationships. 27 This model provides a more comprehensive framework than traditional methods by capturing the reciprocal influences within dyads, making it particularly useful in studying patient-caregiver dynamics. Despite a growing number of applications in the context of various chronic diseases, such as heart failure, 28 breast cancer,29,30 disability, 31 and lung cancer, 2 only a few studies have employed this model to examine dyadic interdependence in the context of HIV. 32 Therefore, the current study applies APIMeM to investigate 1) the dyadic association between family relationships and QoL, and 2) the potential mediating effect of resilience in these relationships in the dyads of PLWH and their FMs. We hypothesized that good family relationships could lead to higher QoL among PWH and their families and the resilience mediated these associations.
Methods
Study Design and Participants
This study utilized cross-sectional dyadic baseline data from an ongoing stepped wedge cluster randomized intervention trial in Guangxi, China, which aims to improve PLWH's suboptimal clinical outcomes. 33 The baseline data was collected prior to the implementation of the intervention. With the assistance and collaboration of the Guangxi Center for Disease Control and Prevention (CDC), two cities and nine rural counties, which have the largest number of reported HIV cases in Guangxi, were selected. This baseline data provided a pristine, naturalistic dyadic status, unconfounded by any variation in intervention exposure. Among the selected districts and townships, 40 HIV clinics or community treatment centers were randomly selected as study sites stratified by urban and rural regions, which ensured sample representativeness and external validity. This sampling approach ensured the sample reflected diverse socioeconomic and healthcare access contexts, which may shape caregiving responsibilities, social support networks, and family stress dynamics. Eligibility criteria of PLWH in this study encompassed the following: 1) aged 18 years or older; 2) have been diagnosed with HIV in the past 2 years or with suboptimal clinical outcomes (eg, detectable viral load or viral rebound). These criteria ensured the sample captured individuals at critical and potentially vulnerable stages of the HIV care continuum; 3) willing to refer one of their adult FMs either of origin (eg, parents, spouse or child) or of choice (eg, close friends, or extended FMs) to participate; 4) willing to provide a hair sample for testing hair cortisol and antiretroviral concentration; 5) willing to consent for the retrieval of viral load and CD4 count data from their medical records; and 6) willing to receive intervention at different timepoints in the stepped wedge trial. Exclusion criteria for PWH included 1) having cognitive or physical inability to respond to assessment questions or to participate in intervention; 2) currently incarcerated or institutionalized for drug use or sex work; 3) participating in other intervention projects during the study period; and 4) planning to permanently relocate outside of Guangxi within a year. FMs were eligible to participate if they: 1) were 18 years of age or older; 2) were referred by a participating PLWH; 3) either a FM of origin or a FM of choice was identified by the PLWH as a primary source of support in managing their HIV after diagnosis; 4) agreed to be randomly assigned to an intervention condition alongside the corresponding PLWH. The exclusion criteria for FMs were the same as for PWH. These dyads were clearly distinguishable by their roles (caregiving recipient vs caregiving provider), which met the dyadic interdependence assumption in APIMeM 34 and allowed us to model distinct actor and partner effects for each role. 35 All participants were enrolled as matched PLWH-FM pairs, linked by a unique Dyad ID. After obtaining informed written consent, a total of 800 PLWH and 800 FMs were recruited and completed the baseline questionnaire survey between October 2023 and December 2023. After handling missing data, the final sample size of 783 complete dyads provides sufficient statistical power for the APIMeM analysis, substantially exceeding the range of dyads recommended for well-powered studies of distinguishable dyads. 35 The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement 36 (see supplementary files). The research protocol was approved by the Institutional Review Boards at all collaborating institutes.
Data Collection Procedure
Both PLWH and FMs were asked to respond independently to questionnaires that took about 45 min to complete. To protect participants’ privacy and ensure the quality of data collection, the survey took place in a private room (eg, doctor's office). The confidential procedures were strictly implemented by trained research team members across all 40 study sites. The research team members (eg, CDC healthcare providers, local community health workers) were available onsite to provide clarification or other assistance as needed, including suggestions of a short break for participants to reduce survey fatigue. To ensure consistency and equity, each participant was provided with 100 Chinese Yuan (equivalent to $13.50 USD at the time of the survey) as a monetary incentive.
Measurements
Demographic Characteristics
The questionnaire for PLWH and FMs collected participants’ demographic characteristics, encompassing age, biological sex (male or female), education levels (lower than high school, high school, college and above), marital status (single, married or cohabited with a partner, divorced/separated or widowed), employment status (employed, unemployed including retired and students), and income level relative to their neighbors or villagers (lower than an average, average, and higher than an average). We also collected FMs’ HIV status (positive or negative).
Family Relationships/Cohesion
We used the Family Adaptability and Cohesion Evaluation Scales II (FACES II) and the Brief Family Relationship Scale (BFRS) to assess family relationships or cohesion. These two scales have established validity in Chinese populations.37,38 Family cohesion for PLWH was measured using eight items from the FACES II. 38 Each item is rated on a 5-point scale from 0 (never) to 4 (all the time). The higher scores indicate greater family cohesion and closer family bonds. Cronbach's α for this 8-item scale in this study was 0.96 for PLWH. Family relationships for FMs were measured using 15 items of the BFRS, which includes cohesion, expressiveness, and conflict. 39 These items were rated on a 3-point scale from 1 (never) to 3 (always). Among these, nine items reflect positive aspects of the family relationship (eg, mutual support, communication), while six items reflect negative aspects (eg, conflict, anger) and were reversely coded. A higher total score indicates a closer perceived family relationship. Cronbach's α for this scale in this study was 0.86 for FMs.
Resilience
Resilience of PLWH and FMs was measured by the Connor-Davidson Resilience Scale, 40 which has been demonstrated to have high reliability and validity in the Chinese population. This scale comprises 10 items, and each item is rated on a 5-point scale from 0 (not true at all) to 4 (true nearly all the time). The higher scores indicate higher resilience. Cronbach's α for this scale in this study was 0.97 for PLWH and 0.95 for FMs, showing good internal consistency.
Quality of Life
The QoL of PLWH and FMs was measured by the 12-item Short Form Health Survey (SF-12), 41 which has been validated in the Chinese population. 42 This scale comprises two components (Physical QoL and mental QoL) to define an individual's positive and negative state of physical and mental health through eight dimensions, including physical function, physical role, body pain, mental health, general health, vitality, social function, and emotional role. There are two to six response options (depending on the item) that evaluate the intensity and/or frequency of health status. The items were scored using the standard norm-based scoring algorithm developed by Ware et al. 41 The total score ranges from 0 to 100, where a higher sum of physical QoL or mental QoL scores implies better corresponding physical or mental QoL. In this study, the Cronbach's α for physical QoL and mental QoL were 0.90 and 0.77 for PLWH, and 0.74 and 0.68 for FMs, respectively.
Data Analysis
Demographic characteristics were described using mean and standard deviation (M ± SD) for continuous variables, and frequency and proportion (n, %) for categorical variables. After assessing the normality assumption of key variables by Q-Q plot, the Pearson correlation coefficients were utilized to evaluate the correlations among PLWH and FMs’ family relationships or family cohesion, resilience, and QoL (including physical and mental QoL). In this study, APIMeM was used to examine whether the PLWHs’ and their FMs’ family cohesion impacted on their own (actor-direct effect) and their partners’ QoL (partner-direct effect) directly and indirectly through the mediator of their own resilience (actor-indirect effect) and their partners’ resilience (partner-indirect effect) at the dyadic level. Based on existing literature,43,44 gender and FMs’ HIV status were included as covariates in the model. However, the model with FMs’ HIV status has resulted in reduced model fit while producing similar path coefficients among key study variables. Therefore, we excluded FMs’ HIV status in the final models to ensure model parsimony and align with our study objectives. Additionally, we considered to force the corresponding pathway as equal (eg, equal actor effects or equal partner effects) to simplify the model without reducing the model fit and changing findings’ interpretability. We considered the chi-squared difference (Δχ2) test as well as model goodness-of-fit indices difference to examine the extent to which these equality constraints significantly impair the model fit. 45 Model fit was evaluated by goodness-of-fit indices, which included the Root Mean Square Error of Approximation (RMSEA, acceptable fit ≤ 0.08), the Comparative Fit Index (CFI, acceptable fit ≥ 0.90), the Tucker-Lewis index (TLI, acceptable fit ≥ 0.90), and standardized root mean square residual (SRMR, acceptable fit ≤ 0.08).28,46 The effect size was estimated using the maximum likelihood method and a 5000-sample bootstrapping approach with a 95% percentile bootstrap confidence interval. Due to minimal missing data (<2% across all key variables), we excluded missingness and used complete data in the APIMeM analyses, resulting in a final sample size of 783 in the APIMeM. All data analysis was performed using R statistical software version 4.1.2, and a two-tailed P-value < 0.05 was considered to indicate statistical significance.
Results
Sample Characteristics
Among 800 PLWH, 58.00% were males, with an average age of 54.8 years (SD = 11.2). Most PLWH were married or cohabited with a partner (73.06%), employed (82.25%), had lower than high school education (58.75%), and had a lower-than-average income (53.13%). For the 800 FMs, 48.88% were males, with an average age of 48.5 years (SD = 13.1). The majority of FMs were married or cohabited with a partner (86.25%) and employed (83.50%). About one half the FMs reported having a lower-than-average income (49.69%) and lower than a high school education (44.99%). A total of 259 (32.8%) FMs were diagnosed with a positive HIV status (Table 1).
Demographic Characteristics of HIV Patient and Family Members Sample (N = 800 Dyads).

Note: SD, standard deviation; PLWH, people living with HIV.
The sample size was not equal to the sum of the total sample size due to missing data or choosing not to answer.
Correlation among key Study Variables
As shown in Table 2, PLWH's family cohesion was positively related to FMs’ family relationships (r = 0.19, P < 0.001), and PLWH's family resilience was positively related to FMs’ resilience (r = 0.21, P < 0.001). PLWH's family cohesion was positively correlated with the resilience of PLWH (r = 0.40, P < 0.001) and FMs (r = 0.17, P < 0.001), PLWH's physical QoL (r = 0.11, P < 0.001), and PLWH's mental QoL (r = 0.17, P < 0.001). PLWH's resilience was positively correlated with physical QoL of PLWH (r = 0.28, P < 0.001) and FMs (r = 0.11, P < 0.001), and mental QoL of PLWH (r = 0.26, P < 0.001). PLWH's physical QoL was positively correlated with PLWH's mental QoL (r = 0.22, P < 0.001).
Pearson Correlations Between Family Relationship/Cohesion, Resilience, and QoL.
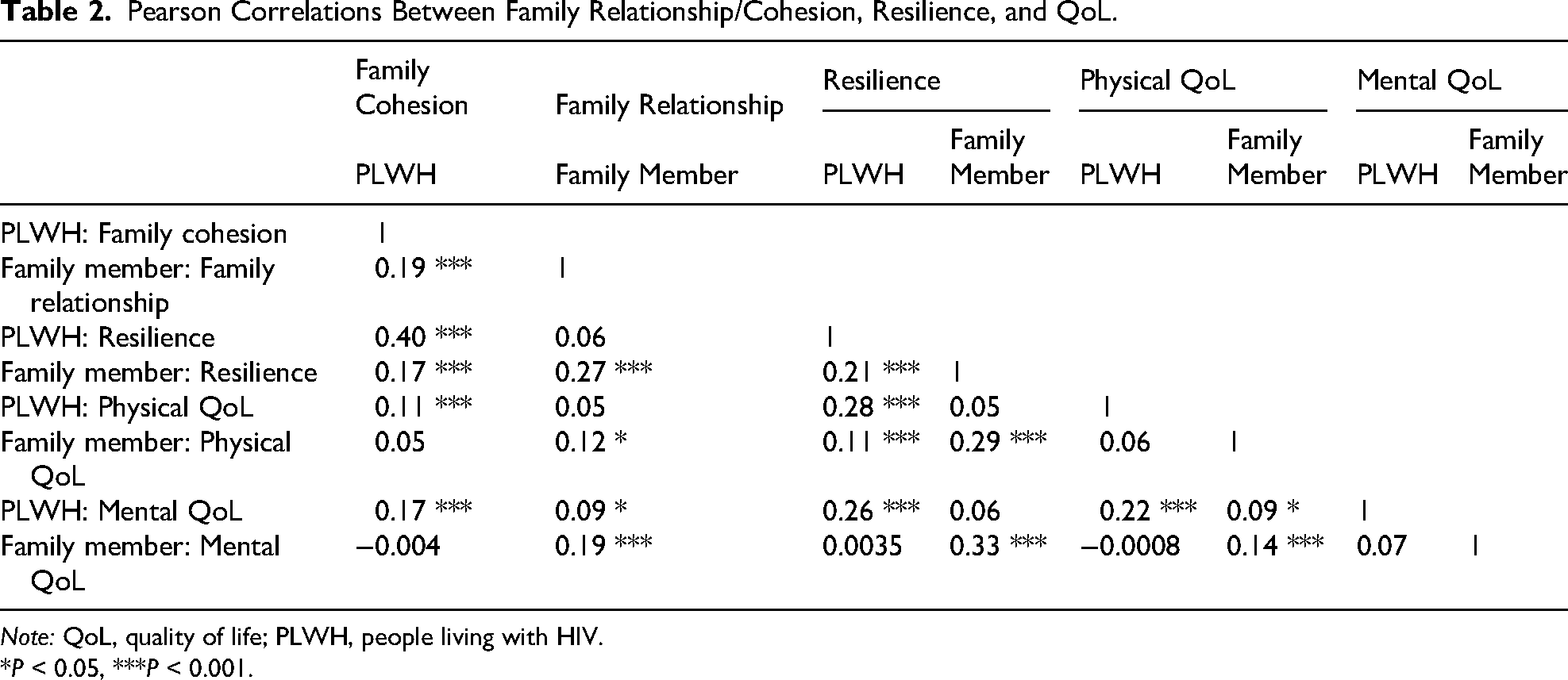
Note: QoL, quality of life; PLWH, people living with HIV.
*P < 0.05, ***P < 0.001.
Actor-Partner Interdependence Mediation Model Analysis
In the APIMeM analysis for physical QoL, the model comparison revealed no significant difference in model fit between the constrained model with equated corresponding paths (cA1 = cA2, bP1 = bP2, cP1 = cP2, see Figure 1) and unconstrained model (Δχ2 = 4.50, P > 0.05). Consequently, we proceeded our analysis with a constrained model over the unstrained model for simplification. The constrained model showed acceptable model fit (RMSEA = 0.06, CFI = 0.93, TLI = 0.82, SRMR = 0.03). As shown in Figure 1 and Table 3, the actor-actor direct effects of PLWH's family cohesion and FMs’ family relationships on their own resilience were found (β = 0.395, P < 0.001, and β = 0.236, P < 0.001, respectively) while no significant effects on their own physical QoL were observed (P > 0.05). PLWH and FMs’ resilience were positively associated with their own physical QoL (β = 0.277, P < 0.001, and β = 0.236, P < 0.001, respectively). The actor-actor indirect effects of resilience were observed in both groups. Specifically, PLWH's family cohesion influenced their own physical QoL through their own resilience (β = 0.101, P < 0.001), and FMs’ family relationships influenced their own physical QoL through their own resilience (β = 0.065, P < 0.001). In terms of the partner effect, PLWH's family cohesion was positively associated with FMs’ resilience (β = 0.136, P < 0.001) and FMs’ resilience mediated the association between PLWH's family cohesion and FMs’ physical QoL (β = 0.038, P < 0.01).

The actor-partner interdependence mediation model of physical quality of life in PLWH and their family members. Note: PLWH, people living with HIV; FM, family members; QoL, quality of life. Estimates are standardized regression coefficients; Significance path coefficients are in solid lines; *P < 0.05, ***P < 0.001.
The Total Effect, Total Indirect Effects, and Direct Effects of the APIMeM in PLWH and Their Family Members (N = 783).

Note. APIMeM, Actor-partner interdependence mediation model; β were standardized regression coefficients; CI, confidence interval; IE, indirect effect; QoL, quality of life; PLWH, people living with HIV.
The APIMeM analysis for mental QoL showed an acceptable model fit (RMSEA = 0.05, CFI = 0.97, TLI = 0.88, SRMR = 0.03). As shown in Figure 2 and Table 3, family cohesion of PLWH and family relationships of FMs were positively associated with their own resilience (β = 0.395, P < 0.001 and β = 0.236, P < 0.001, respectively), resilience of PLWH and FMs were positively associated with their own mental QoL (β = 0.225, P < 0.001 and β = 0.320, P < 0.001, respectively). The actor-direct effect of family relationships on mental QoL was only observed in FMs (β = 0.124, P < 0.05). Resilience served as an actor-actor mediator in both groups. Specifically, PLWH's family cohesion influenced their own mental QoL through their own resilience (β = 0.089, P < 0.001), and FMs’ family relationships influenced their own mental QoL through their own resilience (β = 0.075, P < 0.001). In terms of the partner effect, FMs’ resilience mediated the association between PLWH's family cohesion and FMs’ mental QoL (β = 0.044, P < 0.01).

The actor-partner interdependence mediation model of mental quality of life in PLWH and their family members. Note: PLWH, people living with HIV; FM, family members; QoL, quality of life. Estimates are standardized regression coefficients; Significance path coefficients are in solid lines; *P < 0.05, ***P < 0.001.
Discussion
To the best of our knowledge, this is one of the first efforts using APIMeM to investigate the mediating effect of resilience in the association of FMs’ family relationships and PLWH's family cohesion with QoL from a dyadic perspective. Our study revealed that resilience played an actor-indirect role in both PLWH and FMs. Furthermore, FMs’ resilience played a partner-indirect role in the association between PLWH's family cohesion and FMs’ QoL. These results highlight the interdependent mechanisms between PLWH and their FM and provide new insights into how resilience shapes the impact of family relationships on QoL within HIV-affected families.
The direct effect outcomes of APIMeM revealed that, except for the actor-direct effect of FMs’ family relationships leading to better FMs’ mental QoL, the actor-direct effects of PLWH (PLWH's family cohesion → PLWH's physical and mental QoL) and FMs (family members’ family relationship → family members’ physical QoL) were not significant. Likewise, the partner-direct effects from PLWH's family cohesion and FMs’ family relationships to their partner's physical QoL or mental QoL were also not significant. These insignificant actor-direct effects did not align with previous studies.18,20 For the actor-direct effect, a cross-sectional study among adolescents living with HIV in Uganda showed that PLWH who received more social support and understanding from FMs are more likely to report lower levels of anxiety and depression. 18 A 2-year longitudinal cohort study among ART-treated HIV-infected patients in China also found that PLWH's overall QoL scores were positively associated with having received family support, not feeling discriminated against by their families or discrimination from patients themselves, including never experiencing fear of abandonment by family. 20 Therefore, the result discrepancies may be attributed to differences in participant characteristics and outcome measures. The current study recruited adults with HIV to separately examine physical and mental QoL. Additionally, the absence of such direct effects might indicate that the influence of family relationships/cohesion on QoL is primarily indirect, operating through mediating variables, like resilience, which was verified in our analyses. The significant actor-direct result for FMs’ mental QoL was similar to that of the previous study. 21 A qualitative study that explored the experiences of Chinese FMs of PLWH found that most FMs reported negative emotional experience, psychological stress, and limitation of social interaction due to the long-term care responsibility. 21 Although there is a limited number of quantitative studies directly indicating the impact of family relationships on QoL among PLWH's FMs, some evidence suggests that a cohesive family environment can act as a protective factor against negative psychological outcomes and contribute to improving well-being for FMs coping with HIV. A supportive family relationship means that FMs feel closely bonded and are willing to spend time together. In such environments, FMs can provide significant emotional companionship to one another. This strong emotional bond within the family promotes a sense of loyalty, reciprocity, and solidarity among its members, which are crucial for mental well-being.1,19,47 For the insignificant partner-direct effect, our results were not aligned with the results within the dyads of parents and children, 48 but similar to the dyads of cancer survivors and their spouses. 49 These results suggest that the influence of shared stressors and chronic conditions on QoL in adult partnerships may be more complex, expanding the understanding of dyadic QoL in illness contexts beyond child-parent relationships.
The current studies also revealed an actor-mediating effect of resilience on the association between family relationships/cohesion and QoL. Specifically, experiencing more supportive family relationships and higher family cohesion improved their resilience, which in turn leads to an enhancement of their respective physical and mental QoL in both PLWH and FMs. This means that for each person within the dyad (PLWH and FMs), their personal perception of family cohesion strengthens their individual ability to “bounce back” from adversity, and it is this strengthened resilience that then improves their well-being. 50 Xu et al, conducted a study among older PLWH in China and indicated that strong family support was positively associated with stronger resilience, which led to greater coping, resulting in a better overall physical and mental QoL. 19 Wang et al recruited HIV-positive MSM in China and found that when individuals feel connected and supported by their family, they are better equipped to cope with stress, reframe negative situations, and find positive meaning. 3 These positive consequences can contribute to boosting their individual resilience, which further indirectly improves both the physical and mental aspects of QoL. 3 Although there is no direct evidence in previous research suggesting that these mediating relationships exist among FMs of PLWH, some research indicated that higher levels of resilience among family caregivers of cancer patients promoted adaptive coping strategies, sustained positive emotions, and fostered hope, 51 which in turn improve QoL. The mediating effect of resilience suggests that intervention programs should explicitly target resilience-building within both PLWH and their FMs. This would amplify the benefits of strong family ties and ultimately improve mental and physical health-related QoL.
In terms of partner-mediating effect of resilience, despite the direct effect of resilience on partners’ QoL not being observed, we found FMs’ resilience acts as a bridge linking PLWH's family cohesion to FMs’ physical and mental QoL. This partner-mediating effect of resilience underscore that the psychological well-being within HIV-affected families is deeply interconnected and cannot be understood by examining factors in isolation.1,12 The resilience of FMs serves as a vital mediator, translating the positive familial environment into improved well-being for caregivers. As an unpaid informal caregiver, FMs who are HIV negative and have never cared for an individual living with HIV must learn basic nursing skills and are often under extremely stressful circumstances due to daily care tasks and HIV-related stigma. Conversely, having a positive relationship characterized by reciprocity (defined as the care recipient showing affection or appreciation for the caregiver) and good communication could boost caregivers’ coping skills against stress as an external supportive resource within HIV-affected relationships. 52 A stronger family connection and support perceived by PLWH often signifies similar strong bonds perceived by their FM in the dyadic context. This shared environment facilitates open communication and shared coping strategies that benefit all FMs. 53 Consequently, living within such a supportive and cohesive environment, FMs of PLWH receive more protective psychological resources from the care recipients, which are essential for building and maintaining resilience. 33
Although coping abilities and well-being of one FM can impact the health of others within the family system, it is worth noting that the partner-mediating role of PLWH's resilience on the association between FMs’ family relationships and FMs’ QoL was not found in this study. This unexpected result may be explained by compensatory strain: if PLWH exhibit high resilience and independence, FMs may feel excluded from the caregiving and perceive themselves as unnecessary, leading to a reduced sense of purpose or emotional disconnect.21,54 Furthermore, high resilience in PLWH might signal that they can cope with problems on their own, which could unintentionally reduce emotional closeness or shared coping between dyad members. These findings underscore the complexity of psychological processes among HIV-infected individuals and their FMs.
There are several limitations in this study that should be noted. First, the nature of the cross-sectional data makes it difficult to reflect the dynamic characteristics and the causal relationships among both PLWH and their FMs’ family cohesion, resilience, and QoL. Thus, longitudinal data with dyadic models (eg, APIMeM) are needed to examine causal relationships and examine the stability of these mediation pathways over time. Second, all measures in this study were self-reported, which may introduce self-reporting bias, such as recall bias and social desirability bias. Additionally, shared-method variance within dyads that systematic error raised by using the self-report survey may artificially inflate actor effects. Third, due to the limitation of data availability, we were able to examine only the cohesion domain of family relationships among PLWH, which may reduce construct comparability. Future studies are needed to examine other domains as well, such as expressiveness and conflict, to get a more comprehensive understanding of the impact of family relationships on QoL in this HIV dyadic context. Fourth, the slightly low internal consistency of the SF-12 mental QoL for FMs (Cronbach's α = 0.68) also underscored greater measurement validity in future dyadic research. Fifth, we did not separate specific immediate FMs (eg, spouses or children) during data collection, making it impossible to conduct a sensitivity analysis based on specific relationship types. Future studies could provide additional insights into the impact of different family roles on outcomes using such available categories. Sixth, as this study used baseline data from a parent trial, the sample size for the current dyadic analysis was not pre-determined. Although the inclusion of 783 dyads exceeds the recommended thresholds for robust APIM mediation modeling, 35 future dyadic study designs should pre-determine the sample size to ensure sufficient statistical power for the pathways examined. Seventh, this study was conducted in China, making it difficult to generalize to other regions with different cultural and social backgrounds. For example, the observed dynamics may be influenced by Chinese traditional cultural norms around family obligation, interdependence, and stigma management. Additionally, because of the study design, the results could be generalized only to newly diagnosed PWH or PWH with suboptimal health outcomes. The observed dyadic mediation in diverse cultural and socioeconomic contexts, as well as different HIV infection stages, needs to be explored to understand how resilience shapes the family dynamic system. Nevertheless, our study first utilized the APIMeM to disentangle the interdependent psychological processes within HIV-affected families, moving beyond individual-level correlations to show how (through resilience) and between whom (actor vs partner) family cohesion/relationship impacts physical and mental well-being at a dyadic level, filling the knowledge gap of HIV research.
Conclusion
This study expands the literature by comprehensively examining the dyadic mechanism whereby family cohesion of PLWH and family relationships of their FMs affect QoL and by identifying the potential mediating role of resilience. Our results demonstrated significant direct actor effects of PLWH's family cohesion and FMs’ family relationships on physical and mental QoL, showing that supportive family relationships and a cohesive family environment enhance well-being in both PLWH and their FMs, and an actor-indirect effect of resilience in these associations. Furthermore, FMs’ resilience played a partner-indirect role in bridging PLWH's family cohesion and FMs’ mental QoL. These results suggest that family relationships, resilience, and QoL in PLWH and their FMs operate not in isolation, but rather in a complex and interdependent manner within HIV-affected families. Future interventions aimed at improving QoL of PLWH and their families should target the family as a unit to strengthen family ties and improve the cross-dyadic role of resilience, particularly that of FMs.
Supplemental Material
sj-docx-1-jia-10.1177_23259582261440323 - Supplemental material for Family Relationships, Resilience, and Quality of Life in People Living with HIV and Their Family Members: An Actor-Partner Interdependence Mediation Model
Supplemental material, sj-docx-1-jia-10.1177_23259582261440323 for Family Relationships, Resilience, and Quality of Life in People Living with HIV and Their Family Members: An Actor-Partner Interdependence Mediation Model by Cuihong Huang, Fanghui Shi, Xueying Yang, Shuaifeng Liu, Yuejiao Zhou and Xiaoming Li in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-2-jia-10.1177_23259582261440323 - Supplemental material for Family Relationships, Resilience, and Quality of Life in People Living with HIV and Their Family Members: An Actor-Partner Interdependence Mediation Model
Supplemental material, sj-pdf-2-jia-10.1177_23259582261440323 for Family Relationships, Resilience, and Quality of Life in People Living with HIV and Their Family Members: An Actor-Partner Interdependence Mediation Model by Cuihong Huang, Fanghui Shi, Xueying Yang, Shuaifeng Liu, Yuejiao Zhou and Xiaoming Li in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We greatly appreciate the staff at the Guangxi Center for Disease Control and Prevention for their efforts in participant recruitment and data collection. We extend our appreciation to all the participants who willingly participated in this research.
Ethical Approval Statement
The study protocol was approved by the Institutional Review Boards at both the University of South Carolina (Protocol# Pro00099388) and Guangxi CDC in China (Protocol# GXIRB2020-39-1). All participants provided written informed consent.
Study Registration and Analytic Plan pre-Registration
The data was extracted from the trial which was registered at ClinicalTrials.gov, registration number NCT05174936, registered 13 December 2021. https://register.clinicaltrials.gov/prs/app/action/LoginUser?ts=3&cx=-jg9qo2.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this publication was supported by the National Institutes of Mental Health of the National Institutes of Health under Award Number R01MH127961. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets used in the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.