
Abstract
Background:
Alcohol use remains a significant challenge for treating people living with HIV (people living with HIV). We aimed to examine current use and retrospective self-reported changes in drinking behavior after HIV+ diagnosis in people living with HIV.
Method:
Survey data were collected from a large random sample of people living with HIV (N = 2964, mean age = 42.5, standard deviation = 12.8) in Guangxi, China.
Results:
The estimated prevalence rate of current alcohol use was 42.8%. Among current drinkers, 41.7% reported binge drinking and 10.4% reported hazardous drinking. Among the ever drinkers, 45.4% reported reductions in drinking and 19.5% reported quitting after HIV+ diagnosis. Older age, female gender, higher income, being employed, if currently on antiretroviral therapy, and having received an HIV+ diagnosis within a year were positively associated with quitting; and more education, lower income, currently on antiretroviral therapy, and having received an HIV+ diagnosis more than one year were associated with reduced drinking.
Conclusion:
The time period immediately following receiving an HIV+ diagnosis may represent a window of opportunity for alcohol use intervention in people living with HIV.
Introduction
Alcohol use has been recognized as a common issue in the treatment for people living with HIV (PLWH).1–3 The various health consequences of alcohol use in PLWH range from poor treatment adherence/outcomes to increased comorbidity/mortality. 4 Prior research shows that alcohol use, especially high-risk drinking (e.g. binge drinking) can result in a compromised immune response, 5 increased viral loads and lower CD4 counts, 6 and heightened risk for other diseases including hepatitis C and other liver infections 7 as well as cardiovascular diseases.8,9 In addition to the detrimental consequences in physical health, alcohol use also shows significant negative cognitive effects in PLWH. 10 Studies have shown that alcohol abuse in the context of HIV infection is associated with greater risk for cognitive deficits in various aspects such as reaction time, executive functioning, and verbal/visuospatial learning and memory.10,11 Alcohol use is also associated with other substance use 12 and sexual risk behaviors, such as multiple sex partners and unprotected sex, 13 which increase the risk of transmitting the disease and acquiring secondary infections. 14
It is estimated that there are 850,000 PLWH in China, 15 of whom 115,000 are newly diagnosed. 16 While great efforts have been devoted to control the HIV epidemic in China, less attention has been paid to alcohol use among PLWH. 17 Alcohol use is common in China, as the culture has a long tradition of drinking alcohol for activities including socializing and coping with stress. 18 Among the general Chinese population, 35.7% (55.6% for men and 15% for women) are current drinkers, with more than a half as excessive drinkers. 19 Few studies reported alcohol use among PLWH in China. One survey study in Kunming, a provincial capital city in Southern China, reported that 40% of PLWH are self-reported current drinkers, of whom, one-third were reported as daily drinkers and 40% hazardous drinkers. 17
Various intervention programs have been designed to reduce alcohol use among PLWH,20,21 but few are successful with regard to long-term effects.22,23 One potential limitation of such programs is lacking consideration of timing for best intervention—whether receiving an HIV+ diagnosis will be a good time to initiate alcohol intervention that can improve treatment outcomes. Being aware of the HIV+ status represents an important event in one’s life that can be associated with dramatic behavioral changes. According to the Protection Motivation Theory, 24 being aware of the HIV+ status as a “severe health condition” may motivate patients to gain control of the disease process by re-assessing their own behavior, stopping or reducing health risk behaviors, and initiating or strengthening health promotion behavior.25–27
There is only limited literature that explored behavioral changes among PLWH after they become aware of their HIV+ status. Results from one study with a national probability sample of HIV+ drinkers in the United States indicate substantial reductions in the use of alcohol and other substance after they received HIV+ diagnosis. 28 However, no existing literature reported any data regarding self-reported changes in alcohol use behavior among PLWH in China after they become aware of their HIV+ status. If the hypothesized quitting or reduction in alcohol use is supported by empirical data, the period immediately following the time when a person becomes aware of his or her HIV+ status may present a window of opportunity to initiate alcohol use intervention for maximum effects among this population.
Purpose of this study
The purpose of this study was to bridge the data gap by describing self-reported changes in drinking behavior among PLWH in China after receiving an HIV+ diagnosis. Such information can provide evidence to highlight the importance of investigating changes in alcohol use after receiving HIV+ diagnosis with longitudinal research design. Results of this research may inform the appropriate time period for implementing alcohol use intervention programs after HIV diagnosis.
Methods
Study site and participants
Data used for this study were collected between 2012 and 2013 in Guangxi Zhuang Region, a province located in southwestern China with the second largest number of PLWH among China’s 31 provinces. 29 The detailed sampling procedure was reported previously. 30 Briefly, a total of 17 cities and 75 counties in Guangxi were ranked by the reported number of PLWH. Of these site, 12 (2 cities and 10 towns) with the largest numbers of PLWH were selected as the sampling frame, covering a total of 29,606 PLWH and accounting for 43% of the total PLWH in Guangxi in 2012. From the database of PLWH in the Guangxi Center for Disease Prevention and Control (CDC), approximately 10% of the adult patients (18 years or older) were randomly selected from each of the 12 selected sites randomly. Under the supervision of Guangxi CDC, a project coordinator from local CDC office at each of the 12 study sites was trained to coordinate data collection. Trained research staff first introduced the study to the potential participants and stated that participation was voluntary and would not affect their treatment. About 90% of the selected participants (N = 3002) agreed to participate and signed the informed consent form. A total of 2964 participants were included in our analysis for this particular study after excluding those who did not complete the survey (n = 15) and those with missing information on key variables (e.g. alcohol use) (n = 23).
Survey procedure
Each participant was asked to complete a survey (about 75 min) regarding a range of topics including socio-demographic characteristics, health behaviors, physical and mental health, nutrition condition, and treatment information. The survey was conducted by trained research staff at local CDC offices or HIV clinics where the participants received care to make the participants more comfortable. Approximately 20% of the participants completed the questionnaire by themselves using the paper-and-pencil survey; the rest of participants, due to low literacy level, completed the questionnaire with the research staff reading the questions to them and recording the answers. Clarification or instruction was provided promptly in both cases when necessary. All the interviewers were local CDC research staff or healthcare workers from HIV clinics who received intensive training on research ethics and interview skills, with emphasis on techniques appropriate for PLWH, prior to data collection. Each participant received a small gift (e.g. umbrella and toothpaste) of appreciation at completion of the survey. The research protocol was approved by the Institutional Review Board (IRB) at Wayne State University and Guangxi CDC.
Measurement
Drinking behavior
Ever drinking was assessed by the question: “Have you ever used any alcoholic beverage in your lifetime?” Current drinking was assessed by the question: “Do you currently drink alcoholic beverages?” Participants who responded positively on current drinking were further asked how often they drink (less than monthly, monthly, weekly, and daily) and how many alcoholic drinks they consume on a typical day (<1 drink, 1–2 drinks, 3–4 drinks, ≥5 drinks). A drink was defined as a can of beer, a glass of wine/distilled spirits, or a glass of any home-brewed alcoholic drinks. Participants were also asked about how frequently they engaged in binge drinking (less than monthly, monthly, weekly, daily). Binge drinking was defined as consuming six drinks for men and four drinks for women on a single occasion. 31 Based on the reported frequency of binge drinking, hazardous drinking was defined as having engaged in binge drinking one or more times per week. 32
Change in drinking behavior
Participants were asked to report any change in their drinking behavior after their HIV+ diagnosis with the following five answer options: (1) started drinking, (2) increased drinking, (3) no change, (4) reduced drinking, and (5) quit drinking. Eight participants reported starting drinking after receiving their HIV+ diagnosis. In our analysis, we combined them with those who answered “increased drinking” and named this group as “started/increased drinking.”
Time since HIV+ diagnosis and antiretroviral therapy–related measure
Time (in years and months) since receiving the HIV+ diagnosis and the status of antiretroviral treatment (yes/no) were determined through self-report and confirmed with medical records. CD4 count was obtained from patients’ medical records.
Demographic variables
These variables include gender (male, female), age (18–35, 35–44, and ≥45), ethnicity (Han, Zhuang, and other), education (0–6, 7–9, 10–12, and >12 years), monthly household income (¥/month), current employment status (yes, no), marital status (never married, married, divorced/separated, and widowed), and sexual orientation (heterosexual, sexual minority including bisexual and homosexual). We include ethnicity as an important demographic factor because Guangxi has a large population of one ethnic minority group (Zhuang) that has unique culture and life style that can influence alcohol use.
Statistical analysis
Chi-square test (Fisher’s exact test for cells with frequency ≤5) was used to examine associations between changes in drinking behavior (i.e. started/increased, reduced, and quit drinking) and sample characteristics including demographics and HIV treatment–related measures. Multivariate logistic regression models were used to further examine the adjusted effects of variables that were associated with each drinking behavior change in the univariate test (i.e. chi-square).
Results
Sample characteristics
Among the 2964 participants (mean age = 42.5, standard deviation (SD) = 12.8), 62.8% were male, 70.8% were ethnic Han (the predominant ethnic group), and 25.8% were ethnic Zhuang. Nearly half (46.3%) of the sample had 0–6 years of education, and 53.2% had a monthly household income less than 1000 RMB, below the provincial poverty level. The average time since their diagnosis of HIV positive status was 39 months (SD = 29). Over 70% of the participants were currently on antiretroviral therapy (ART), and 55.5% had CD4 counts less or equal to 350 cells/mm3. More details about the sample’s characteristics are provided in Table 1.
Characteristics of the study sample by gender, n (%).
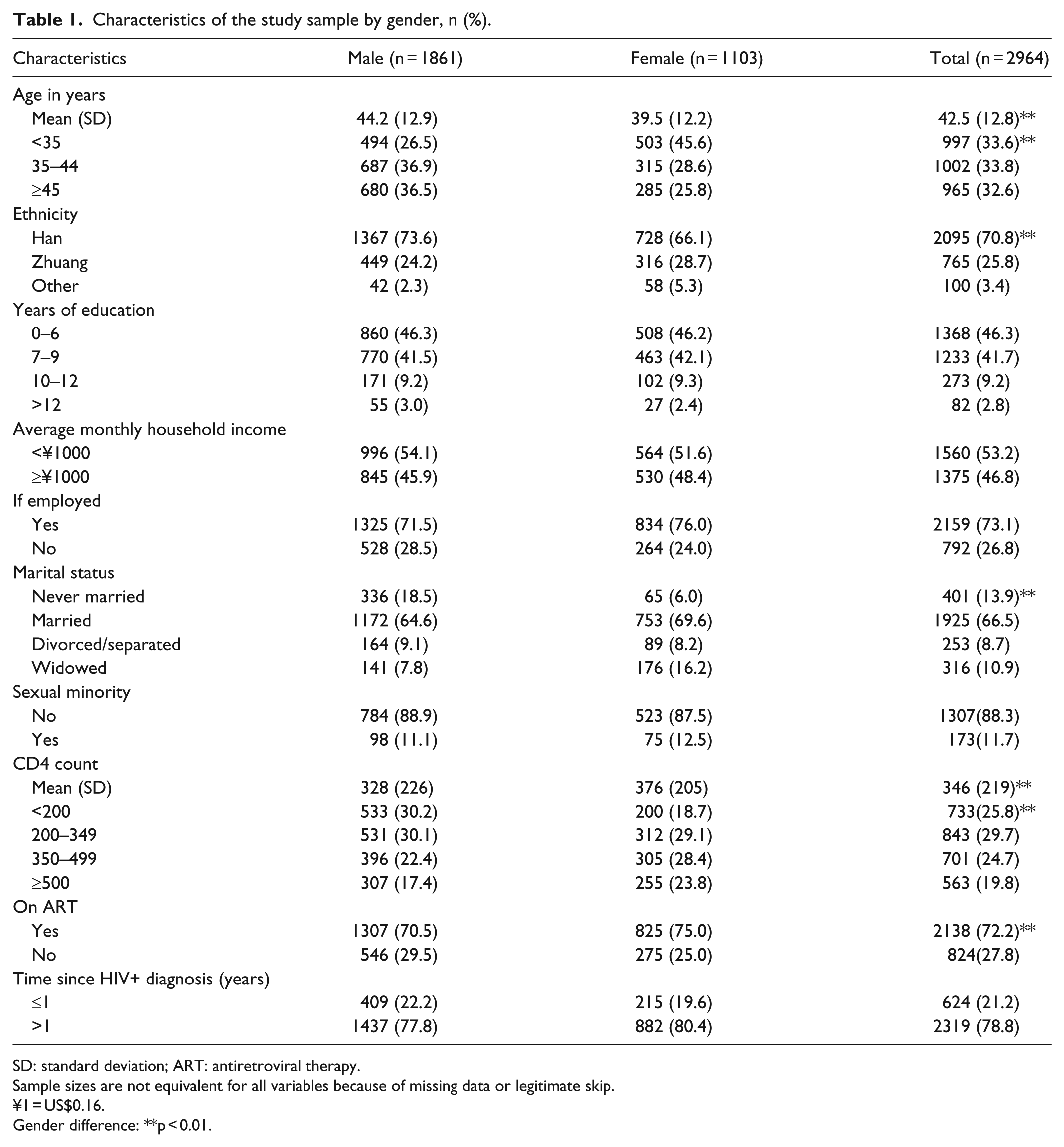
SD: standard deviation; ART: antiretroviral therapy.
Sample sizes are not equivalent for all variables because of missing data or legitimate skip.
¥1 = US$0.16.
Gender difference: **p < 0.01.
Current alcohol use
A total of 1269 (42.8%) participants reported current using alcohol, and Figure 1 depicts the detailed patterns of alcohol consumption. Two-thirds (66%) of female current drinkers reported drinking alcohol on less than one occasion per month, while male current drinkers reported higher prevalence of weekly or daily drinking (Figure 1(a)). Although the majority (80%) of current drinkers reported consuming an average of ≤2 drinks on a typical drinking day (Figure 1(b)), 41.6 % reported engaging in binge drinking and 10.3% reported hazardous drinking (Figure 1(c)). Approximately 30% reported monthly or more frequent binge drinking (Figure 1(d)).

Patterns of alcohol consumption: (a) frequency of alcohol use, (b) amount of alcohol consumed per day on drinking days, (c) prevalence of binge drinking and hazardous drinking, and (d) frequency of binge drinking.
Changes in drinking behavior after receiving HIV+ test result
After receiving their HIV+ diagnosis, 67.4% of respondents reported having made change to their drinking behavior: 45.4% reported a reduction in alcohol use, 19.5% reported quitting drinking, and 2.5% reported initiating or increasing in alcohol use. The associations between drinking behavior change (including started/increased drinking, reduced drinking, and quit drinking) and a set of influential factors are presented in Table 2. Gender, ethnicity, and income were significantly associated with initiation and increases in drinking (Table 2). These relationships remained significant from multivariate logistic regression analysis to simultaneously examine these variables’ effects on started/increased drinking (Table 3). Specifically, being male odds ratio (OR) = 0.39(0.18, 0.86)), Zhuang (OR = 0.13 (0.03, 0.62), and having lower income (OR = 0.45(0.20, 0.99)) were significantly associated with lower risk for drinking initiation/increase.
Changes in drinking behavior after receiving HIV+ diagnosis and their associations with sample characteristics.

ART: antiretroviral therapy.
Sample sizes are not equivalent for all variables because of missing data or legitimate skip.
Fisher’s exact test was used.
p < 0.05; **p < 0.01.
Logistic regression results of changes in drinking behavior after receiving HIV+ diagnosis.

OR: odds ratio; CI: confidence interval; ART: antiretroviral therapy.
Each drinking behavior change type was used as outcome variable, respectively. Sample characteristic variables were used as predictors. Multivariate logistic regression was used to include all sample characteristics. Only variables that showed significant association in the univariate analysis in Table 2 were included in the multivariate model here.
*p < 0.05; **p < 0.01.
Results in tables also indicate that age, ethnicity, education, receiving ART, and the time after receiving an HIV+ diagnosis were significant associated with reduced alcohol use. Results from logistic regression in Table 3 indicate that lowest level of education (OR = 0.52(0.28, 0.99)) and receiving an HIV+ diagnosis within 1 year (OR = 0.68(0.51, 0.92)) were negatively associated with reduced drinking, while lower income (OR = 1.41(1.11, 1.79)) and receiving ART (OR = 1.69(1.30, 2.18)) were positively associated with reduced drinking.
Univariate analysis results in Table 2 also indicate that age, gender, education, income, employment, receiving ART, and the time duration since receiving the HIV+ diagnosis were all significantly associated with quitting drinking. All of these variables from the univariate analysis remained significant when they were simultaneously included in the multivariate logistic regression model except for education. Being younger (OR = 0.62(0.41, 0.93) for <35 age group and OR = 0.67(0.36, 0.81) for 35–44 age group), male (OR = 0.54(0.36, 0.81), lower income (OR = 0.62(0.45, 0.85)), and divorced or separated (OR = 0.43(0.20, 0.92)) were negatively associated with quitting drinking, whereas being employed (OR = 1.52(1.09, 2.13)), on ART treatment (OR = 1.77(1.24, 2.53)), and receiving the HIV+ diagnosis within 1 year (OR = 2.50(1.78, 3.52)) were positively associated with quitting drinking.
Discussion
Prevalence and patterns of current alcohol use
In this study, we documented the prevalence rates and patterns of alcohol use among PLWH and assessed changes in drinking behavior after PLWH received their HIV+ diagnosis. This study, to the best of our knowledge, is the first to investigate changes in drinking behavior among PLWH after becoming aware of their HIV+ diagnosis using survey data collected from a large random sample in China. Findings of our study indicate that the prevalence rate of current alcohol among PLWH was 42.8%, substantially higher than the prevalence rates among the general Chinese population (26.3% for men and 7.8% for women). 19 The prevalence rate of current alcohol use observed in our sample is close to 40%, the rate for PLWH in an ethnic minority community (n = 455) in Southwest China reported in another study by Luo et al. 17 With regard to patterns of alcohol use, the majority of drinkers in this study reported monthly alcohol use or less, while 15.2% (17.4% for men and 3.6% for women) reported daily alcohol use.
Despite the relatively low prevalence rates of daily alcohol use, the prevalence of binge drinking was 41.6% among current drinkers, which is close to 41.2%, the rate of hazardous drinking (defined as 14 drinks per week for men and 7 drinks per week for women) reported in Luo et al.’s 17 study. Although binge drinking was not reported in Luo’s study, information regarding hazardous drinking provides sufficient evidence supporting the significance of alcohol abuse among PLWH in China. In addition, about 10% of the participants in our study sample reported weekly or daily binge drinking. These numbers are particularly alarming when considering the detrimental effects of high-risk alcohol use on HIV patients’ symptoms, adherence to treatment, and overall prognosis.
Changes in drinking behavior after receiving an HIV+ diagnosis
Consistent with findings from research conducted in the United States, 28 we found substantial changes in drinking behavior after PLWH receiving their HIV+ test result. In our study, 45.5% of the sample reported reducing drinking and 19.5% quitting after they became aware of their HIV+ status. Individuals who received their HIV+ diagnosis within 1 year were more likely to quit drinking than those who received their result more than 1 year before the survey, and those who have known for more than 1 year before the survey were more likely to reduce alcohol use compared to those who received their HIV+ diagnosis less than 1 year before the survey. This result suggests that there may be a critical window of opportunity for promoting quitting behavior in PLWH following HIV+ diagnosis.
A number of demographic correlates are also worth mentioning. Relative to younger PLWH, those who were 45 years or older were more likely to quit. It is possible that older people are generally more vulnerable toward alcohol-related health risks. Female PLWH were more likely to quit drinking than their male counterparts. This may be explained by the fact that female participants in this study consumed alcohol at a much lower level than males, so they were more likely to succeed in quitting due to lower level of alcohol misuse. People with higher levels of education were more likely to reduce and quit drinking compared to those with only elementary or middle school education. This is consistent with findings among general population where education is associated with lower likelihood of substance use and higher likelihood of initiating quitting. 33 Similar to but not completely same as education, people with higher income were more likely to quit, whereas people with lower income were more likely to reduce drinking. Also, people who were employed showed higher likelihood to quit drinking.
With regard to treatment, PLWH who were receiving ART at the time of study were more likely to reduce alcohol consumption and/or quit. One possible explanation would be that these participants quit or reduced drinking due to their concerns that alcohol may reduce the effect of their ART treatment. It is also possible that individuals on ART are more likely to be motivated externally by routinely seeing healthcare professionals which may increase their likelihood to change unhealthy behaviors.
Conclusion and limitations
This is the first study to examine changes in alcohol use among PLWH in China after they received the HIV+ diagnosis using self-reported data collected from a large random sample. Findings of this study indicate high prevalence of alcohol use among PLWH, with a considerable portion of PLWH drinkers reported quitting or reducing drinking after receiving their HIV+ diagnosis. Such findings highlight the need for future studies to further investigate the changes in alcohol use following receiving an HIV+ diagnosis using a longitudinal research design. This line of research can provide valuable information for designing more effective alcohol use interventions among PLWH using the timing period after HIV+ diagnosis as a window of opportunity to achieve better intervention effects. In addition, this study also identified some characteristics such as gender, education, income, and ART as important associates of drinking behavior changes, suggesting at-risk subgroups deserving special attention in more tailored intervention programs.
This study has several limitations. First, data used in this study were cross-sectional; therefore, temporal relationships cannot be inferred. Although factors such as ART were associated with quitting or reducing drinking in this study, further research with longitudinal design is required to confirm such relationships. Second, we measured current drinking by asking directly “do you currently drink.” Individuals answered “Yes” to this question would be classified as current drinkers. This is different from the general criteria that current alcohol drinking was measure from alcohol use in the past 30 days. However, the current alcohol drinking prevalence reported in our sample is line with other studies. Third, self-reported behavior change may be impacted by recall bias since the majority of our study participants have known their HIV+ test result for over 1 year. Future studies that recruit participants upon receiving their HIV+ test results and follow participants’ drinking behavior over time would be useful to further clarify the temporal relationship between the timing of HIV diagnosis and alcohol-related behavior change. Fourth, this study did not separate those who have progressed to AIDS, which may be an important limitation because this could be an important factor influencing alcohol consumption. Finally, our study only included PLWH in Guangxi, China, which could have a different ethnic or demographic composition, different prevalence of HIV/AIDS, and different subcultural of alcohol use than other provinces in China, which limits our ability to generalize the results. Despite these limitations, this study represents an important initial step toward a better understanding of self-initiated change in alcohol use behavior after HIV+ diagnosis, which has potential implications for future intervention programs.
Footnotes
Acknowledgements
The authors are grateful to the staff at Guangxi Centers for Disease Control and Prevention and their local offices and HIV clinics for the assistance and cooperation in subject recruitment and data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Wayne State University Institutional Review Board #093308B3F and Guangxi CDC (no number available).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Health (R01AA18090), (R01HD74221).
Informed consent
Written informed consent was obtained from all subjects before the study.