
Abstract
We investigated men who have sex with men's (MSM) location preferences for long-acting injectable pre-exposure prophylaxis (LA-PrEP). MSM (n = 1076) who completed the 2021 American Men's Internet Survey, were currently prescribed oral PrEP, and expressed LA-PrEP interest reported location preferences for receiving LA-PrEP: healthcare provider (HCP) setting, pharmacy, or at-home. HCP settings were preferred by 60% of participants; 26% preferred home and 14% preferred pharmacy. In adjusted models, high healthcare stigma was associated with preferring pharmacy and at-home versus HCP, while high friends/family stigma was associated with preferring HCP settings versus pharmacy. Healthcare access history was associated with preference for HCP setting versus home. Being 25 to 29 or 30 to 29 years old versus 40+ was associated with preferring HCP versus home. Private insurance was associated with location preferences. Findings support the need for multiple LA-PrEP service locations to best reach MSM and highlight multiple complex factors that influence such preferences.
Plain Language Summary
We investigated location preferences among men who have sex with men (MSM) for receiving long-acting injectable pre-exposure prophylaxis (LA-PrEP), a medication approved to prevent human immunodeficiency virus (HIV). MSM (n = 1076) who completed the 2021 American Men's Internet Survey, were currently prescribed oral PrEP, and expressed interest in switching to LA-PrEP reported preferences for where they would like to receive LA-PrEP. Responses included healthcare provider (HCP) setting, pharmacy, or at-home. HCP settings were preferred among 60% of MSM; 26% preferred home, and 14% preferred pharmacy. In adjusted models, high healthcare stigma was associated with preferring pharmacy and at-home over HCP setting, while high friends/family stigma was associated with preferring HCP settings over pharmacy. Healthcare access history was associated with preference for HCP setting over home. Being younger (25-29 or 30-29 vs 40+ years old) was associated with preferring HCP over home. Private insurance was associated with various location preferences. Findings support the need for multiple LA-PrEP service location options to best reach MSM and highlight multiple complex factors that influence their preferences.
Introduction
Men who have sex with men (MSM) continue to be disproportionately impacted by the human immunodeficiency virus (HIV) epidemic; MSM accounted for 70% of new HIV diagnoses in the United States in 2021, despite representing only 3.9% of the general population.1,2 HIV oral pre-exposure prophylaxis (PrEP), approved by the federal drug administration (FDA) in 2012, is an established safe and effective method of preventing HIV. 3 Despite a high awareness of and willingness to use PrEP among US-based MSM, initiation rates remain low; past year PrEP usage rates among MSM range from 3.8% in 2014 to 14.6% in 2020. 4 Although usage is increasing over time, many barriers to PrEP uptake remain. Structural and social factors contributing to low PrEP uptake include stigma from healthcare providers and/or close social networks, distrust of healthcare providers and systems, health insurance coverage barriers, and difficulty navigating financial assistance programs.4-10 MSM living in rural areas have lower oral PrEP uptake compared to MSM living in urban areas. Data on racial disparities vary showing that Black MSM have lower 11 or similar 12 oral PrEP uptake compared to non-Black MSM; given the higher rates of new HIV diagnoses among MSM in the United States 13 even equal uptake rates indicate a disparity in unmet need.
The effectiveness of oral PrEP pills, the only modality available until recently, is dependent on daily or near-daily pill taking; this has presented barriers to both uptake and adherence.14,15 Injectable cabotegravir, a form of long-acting injectable PrEP (LA-PrEP), received FDA approval in 2021 for use with adolescents and adults at risk of HIV. 16 Results from clinical trial HPTN-083 demonstrate a 66% relative reduction in HIV risk compared to oral PrEP among MSM and transgender women, indicating high effectiveness, attributed in part to better adherence among LA-PrEP users. 17 LA-PrEP administered by a healthcare provider every 2 months through gluteal intramuscular injection also reduces the adherence-related challenges of daily oral PrEP.17-20 By avoiding the presence of pills or bottles in the household, LA-PrEP affords a greater level of discretion, minimizing PrEP-related stigma as an uptake barrier.21,22 LA-PrEP also has the potential for self-administration, particularly in the context of the growing popularity of and familiarity with other at-home injectable medications, (eg, Ozempic).23,24 An emerging body of literature has demonstrated high levels of interest in and preference for LA-PrEP among both MSM who are currently taking daily oral PrEP and those who are not, including MSM at highest risk for HIV acquisition, with some variation by demographic factors such as race.25-32 Modeling suggests that LA-PrEP could prevent more incident infections in the United States than oral PrEP at similar usage.33-35 However, more research is needed to identify optimal service delivery strategies that facilitate LA-PrEP use among MSM.
The provision of PrEP services at locations other than traditional healthcare settings, including pharmacies or at home, may improve PrEP uptake and utilization rates among MSM by addressing barriers such as lack of available transportation, healthcare provider stigma, and inequitable access to healthcare settings.5,36-41 While there is a dearth of research on PrEP service location preference, previous studies among MSM in the U.S., England, and China have found that HIV and sexually transmitted infection (STI) testing and sexual healthcare location preference is influenced by various factors, including sociodemographics (eg, geographic location and race), structural in/securities (eg, housing stability), healthcare beliefs and prior experiences (eg, privacy concerns, healthcare provider trust, previous HIV testing experience, and HIV risk perception), and stigma factors.42-47
The potential of LA-PrEP to dramatically reduce population-level HIV incidence depends on widespread PrEP uptake and adherence. As we begin to learn more about LA-PrEP uptake through early implementation in the United States, a proactive approach to understanding additional user preferences for LA-PrEP administration is needed to develop effective and targeted PrEP delivery strategies for MSM and to improve PrEP coverage. Among an online sample of the United States MSM, we investigated location preferences for accessing LA-PrEP and the demographic factors, prior healthcare experiences, and types of stigma that are associated with those preferences.
Methods
Study Design and Analytical Sample
We used data from the 2021 American Men's Internet Survey (AMIS), which surveyed MSM using online recruitment and data collection between September 2021 to February 2022. The AMIS methods have been previously reported. 48 Briefly, recruitment used advertisements on a variety of websites, social media, and dating apps. Participants were eligible if they resided in the United States, were 15 years or older, reported male sex at birth, and reported at least one experience of oral or anal sex with a man in their lifetime. Participants age 15 to 17 years were also eligible if they identified as gay or bisexual even if they hadn’t previously had sex with a man. Eligible men who provided informed consent completed the survey online in English or Spanish which included questions about demographic characteristics, sexual and drug-use behaviors, HIV & STI prevention activities, including PrEP, healthcare utilization, and social determinants of health. Participants did not receive remuneration. Activities were approved by the Emory University institutional review boards.
The analytic sample for the current study (n = 1076) was restricted to participants who reported currently taking daily oral PrEP and who, after a brief description of LA-PrEP, responded yes to the question “If injectable PrEP were available from your local doctor and you could access it for free, would you go to your doctor in the next month to start injectable PrEP?” Survey skip patterns dictated that only this subset of participants were presented with the item used as the primary outcome in analyses, 1076 participants provided valid responses to the item (Figure 1).
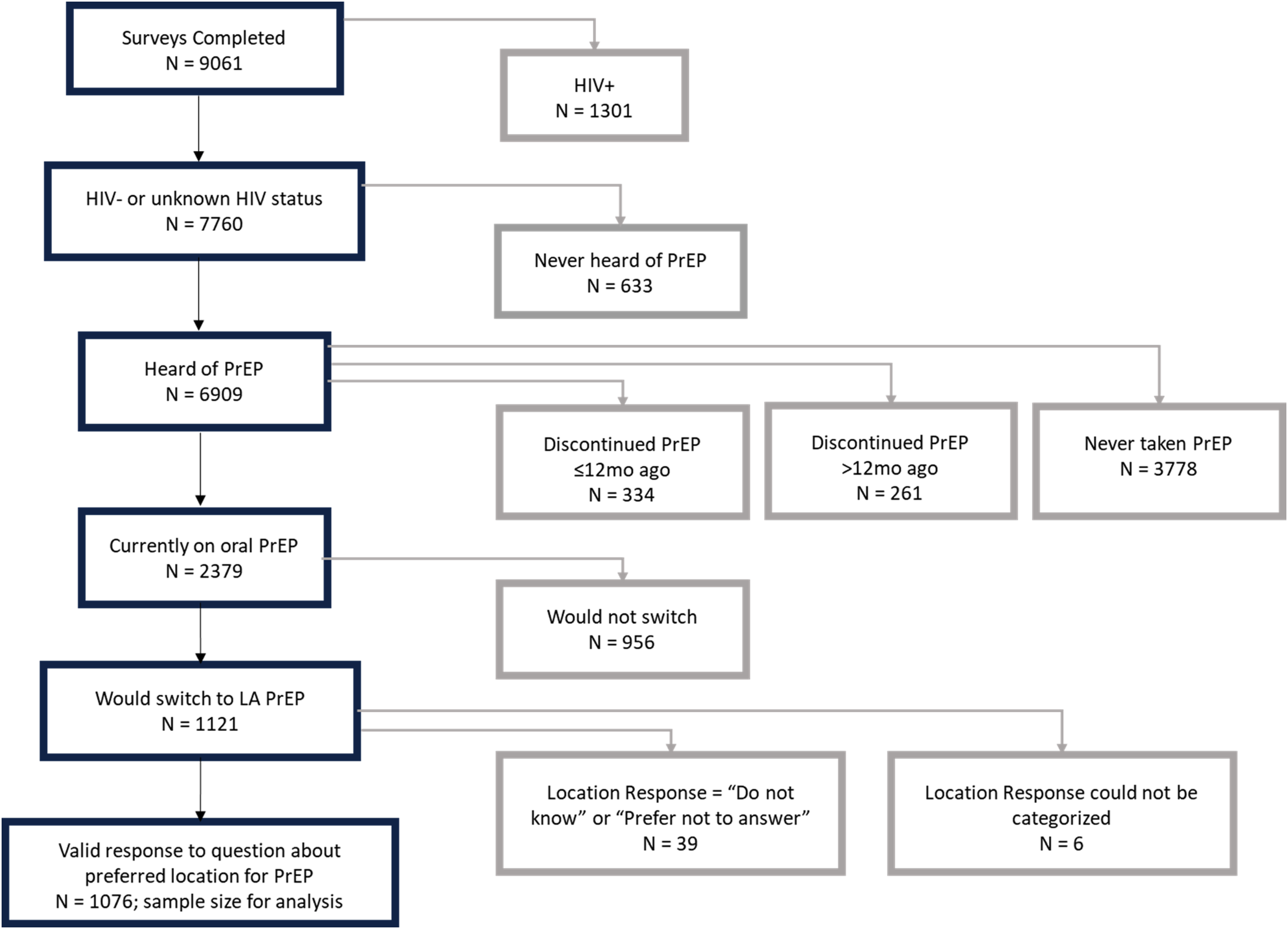
Flowchart of participant inclusion in analytic sample.
Measures
Dependent variable: Participants who expressed interest in going to their doctor in the next month to start injectable PrEP if it were free and available were asked: “Once a doctor prescribes injectable PrEP for you, it may be possible to get your injection at another place. Where would you prefer to get the injection?” Only one response could be selected, and response options were (1) private doctor's office, (2) sexually transmitted disease (STD) clinic, (3) health center, (4) pharmacy, (5) at home, and (6) other, with the option to specify another location, “I prefer not to answer,” and “don’t know.” For analysis, the first 3 options were recategorized as “healthcare provider (HCP) setting,” as were specified “other” responses that described specific HCP settings; specified “other” responses that did not fall into any of the provided categories, as well as “don’t know” and “I prefer not to answer” responses, were excluded from analysis. While pharmacies do provide healthcare, the context of pharmacy healthcare provision was considered different enough from the other HCP settings to constitute its own category. The outcome variable used in all modeling included 3 categories: HCP setting, pharmacy, and at home.
Explanatory Variables
Sociodemographic factors included: age in years (15-24, 25-29, 30-39, 40+), race/ethnicity (non-Hispanic Black, non-Hispanic White, Hispanic of any race, or “Other/multiple/unknown”), sexual orientation (homosexual/gay/lesbian, heterosexual/straight, bisexual, pansexual, or queer), annual household income before taxes (specified ranges between $0-19 999 and $75 000+), highest level of education completed, full-time employment, and past 12 months homelessness. Participants’ ZIP codes were categorized per the National Center for Health Statistics rural/urban classification, and “micropolitan” or “noncore” locations were classified as nonmetropolitan, or rural, for analysis. 49
Substance use variables included use of any nonprescribed or illicit drug other than marijuana in the past 12 months and nonprescribed injection drug use ever.
Various measure of healthcare access and communication were explored: having private insurance (vs other or no insurance), having ever taken an at-home HIV test, location where PrEP was procured in the past 12 months (prescription/directly from an HCP, clinic, or health department vs others [eg, from a friend, online]), and whether an HCP had talked to the participant about sex/sexual health.
Sexual behavior stigma was measured using 15 items assessing feelings, behaviors, and interactions the participant experienced in relation to others knowing that they have sex with men. For each item, participants reported whether they had experienced it never (coded as 0), >6 months ago (coded as 1), or within the past 6 months (coded as 2). Based on prior papers each item was categorized as being in the domain of healthcare (7 items), friends and family (3 items), or social stigma (5 items).50,51 Items within each stigma domain were summed based on the above coding and dichotomized at the median, yielding 3 variables that measured high versus low healthcare, friends and family, and social stigma.
Healthcare-related stigma scores ranged from 0 to 14, with a median of 2 and a mean (standard deviation) of 2.62 (3.06). Friends and family stigma scores ranged from 0 to 6, with a median of 1 and a mean (standard deviation) of 1.55 (1.69). Social stigma scores ranged from 0 to 10, with a median of 2 and a mean (standard deviation) of 1.84 (1.82). For all 3 sexual behavior stigma measures, scores of 2 or higher were categorized as high. Alpha coefficients for healthcare, friends and family, and social stigma scales were 0.85, 0.74, and 0.68, respectively.
Statistical Analysis
We measured the prevalence of each explanatory variable, stratified by preferred location for PrEP injection receipt, and used Pearson's χ2 tests to test for significant differences. We used bivariate and multivariable multinomial regression models with robust variances to estimate prevalence ratios (PR) and robust 95% confidence intervals (CI). Models were run to produce PR estimates for injection location preference of HCP setting versus pharmacy, HCP setting versus home, and home versus pharmacy. Variables that yielded P-values of <.2 in at least one comparison in bivariate multinomial logistic regression models were considered for inclusion in the multivariable-adjusted model; final covariate selection was guided by prior literature, model fit, maximization of parsimony, and minimization of collinearity. In order to present estimates for all preference comparisons, each model was run twice—first with pharmacy as the outcome reference group (HCP setting vs pharmacy and home vs pharmacy) then with home as the outcome reference group (HCP setting vs home). In each case, the underlying model and sample were the same; the change in reference group simply allowed us to present estimates for each possible comparison. The final multivariable model included age, race/ethnicity, injection drug use history, private health insurance, history of at-home HIV test, receipt of PrEP via healthcare provider/setting encounter, seeing an HCP who discussed sex/sexual health with the participant, healthcare stigma, and friends and family stigma. All analyses were conducted using Stata/MP 15.1 (College Station, TX).
Results
Sample Description
Among our sample (n = 1076), age ranged from 18 to 75 years, with a median age of 41 years (Table 1). More than two-thirds of the sample identified as non-Hispanic White, and a large majority identified as homosexual or gay. Majorities reported having a college degree, salaries greater than $75,000, and being employed full-time. More than half (60.4%) preferred an HCP setting, while about one-quarter (25.9%) preferred home and 13.7% preferred a pharmacy for LA-PrEP injections.
Sample Characteristics, Stratified by LA-PrEP Location Preference (N = 1076).
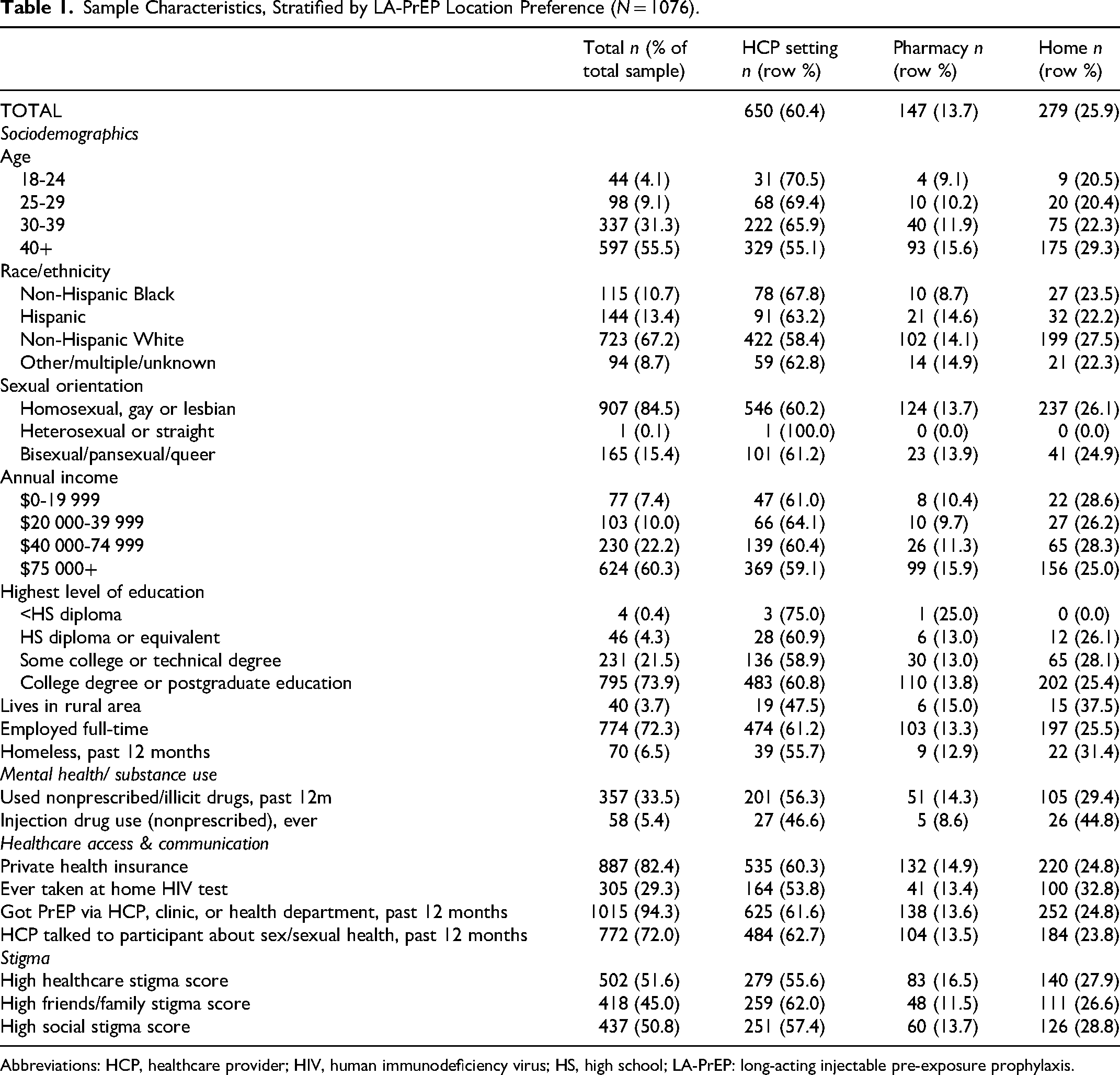
Abbreviations: HCP, healthcare provider; HIV, human immunodeficiency virus; HS, high school; LA-PrEP: long-acting injectable pre-exposure prophylaxis.
HCP Setting Versus Pharmacy
In bivariate models (Table 2), being 30 to 39 versus 40+ years old and high versus low family/friends stigma were significantly associated with preferring an HCP to a pharmacy setting for LA-PrEP injection. Private health insurance and high versus low healthcare stigma were significantly associated with preferring a pharmacy to an HCP setting.
Crude and Adjusted Prevalence Ratios for LA-PrEP Location Preference Based on Multinomial Logistic Regression (N = 1076).
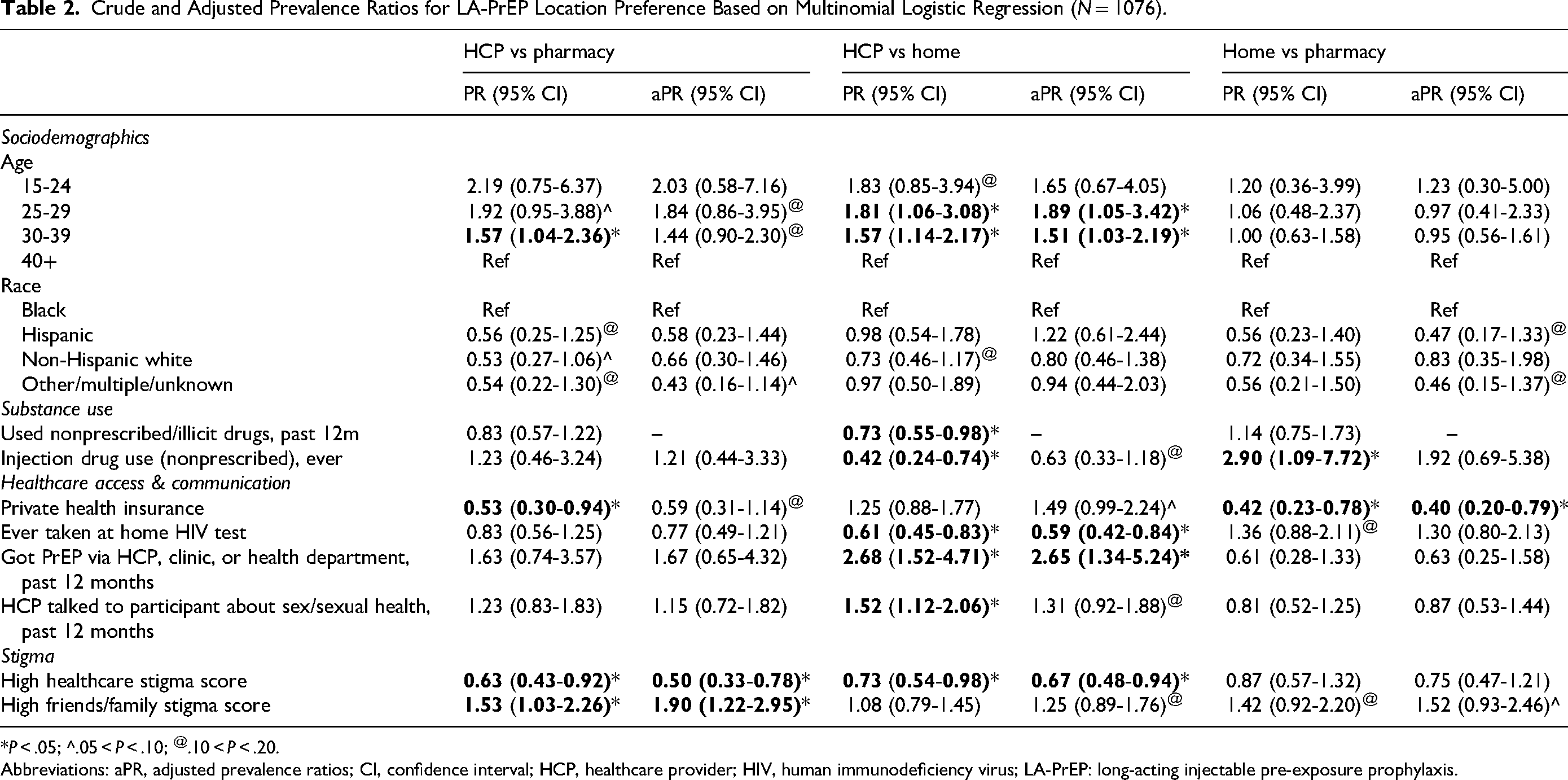
*P < .05; ^.05 < P < .10; @.10 < P < .20.
Abbreviations: aPR, adjusted prevalence ratios; CI, confidence interval; HCP, healthcare provider; HIV, human immunodeficiency virus; LA-PrEP: long-acting injectable pre-exposure prophylaxis.
In the multivariable model (Table 2), those with high healthcare stigma (aPR = 0.50; 95% CI = 0.33-0.78) remained more likely to prefer pharmacy over HCP settings, and those with high friends/family stigma (aPR = 1.90; 95% CI = 1.22-2.95) were more likely to prefer HCP over pharmacy settings.
HCP Setting Versus Home
In bivariate models (Table 2), being 25 to 29 or 30 to 39 versus 40+ years old, having received PrEP through a healthcare encounter, and having had an HCP talk to the participant about sex were all significantly associated with preferring an HCP setting versus home for LA-PrEP administration. Having used nonprescribed/illicit drugs in the past 12 months (not included in multivariable model because of overlap with injection drug use), any history of injection drug use, having ever taken an HIV test at home, and high versus low healthcare stigma were significantly associated with preferring home to an HCP setting for LA-PrEP injections.
In the multivariable model (Table 2), being 25 to 29 (aPR = 1.89; 95% CI = 1.05-3.42) or 30 to 39 (aPR = 1.51; 95% CI = 1.03-2.19) versus 40+ years old, and getting PrEP via HCP, clinic, or health department in the past year (aPR = 2.65; 95% CI = 1.34-5.24) remained significantly independently associated with a preference for HCP setting versus home. A history of at-home HIV testing (aPR = 0.59; 95% CI = 0.42-0.84) and high healthcare stigma (aPR = 0.67; 95% CI = 0.48-0.94) were associated with preferring home over an HCP setting.
Home Versus Pharmacy
In bivariate models (Table 2), history of injection drug use was significantly associated with a preference for home versus pharmacy for LA-PrEP injection. Private health insurance was significantly associated with preferring a pharmacy compared to home settings for LA-PrEP injection.
In the multivariate model (Table 2), only having private health insurance (aPR = 0.40; 95% CI = 0.20-0.79) remained significantly independently associated with preference for pharmacy versus home.
Discussion
This is the first study, to our knowledge, to explore location preferences for receipt of LA-PrEP care among a large sample of US-based MSM. We found significant demographic, healthcare-related, and stigma-related correlates of preferences for receiving injections at HCP settings, pharmacies, or at home. While approximately 60% of participants preferred an HCP setting, sizable minorities preferred home (about 25%) or pharmacy (about 14%). Given that the study sample was comprised entirely of MSM currently prescribed oral PrEP, and nearly all of them had received PrEP via an HCP setting in the past 12 months, it follows that most would prefer what they are used to. However, our findings highlight that among those already connected to PrEP services in an HCP setting, 40% would prefer an alternate setting for LA-PrEP. These findings suggest that MSM not currently utilizing PrEP might also be interested in care setting alternatives, although future research is needed to confirm this hypothesis. Nonetheless, our findings highlight the utility of diverse PrEP service delivery locations in improving PrEP access for MSM.
In adjusted models, previous HIV/PrEP service location was significantly associated with LA-PrEP location preference. Those who reported getting oral PrEP from an HCP setting in the past 12 months were significantly more likely to prefer an HCP setting to home, while prior use of an at-home HIV test was associated with a preference for home versus HCP setting. Our findings suggest that research exploring location experiences and preferences for HIV, STI, and sexual health services42-47 may also translate to LA-PrEP. This complementary existing research may be useful in informing LA-PrEP implementation strategies to be evaluated in future studies. Further, this suggests that expanding location services regarding one healthcare service may pave the way for others, and efforts to provide pharmacy-based and at-home healthcare may be useful in broadly expanding service access for MSM, meeting unmet need.
High healthcare stigma scores—based on both anticipated and enacted MSM-related stigma—were associated with a strong and significant preference away from HCP settings. These findings align with previous studies that have identified a link between discrimination in a healthcare setting due to sexuality- and race-based stigma and healthcare utilization/preferences among MSM, including diminished HCP trust, avoidance of healthcare settings and a preference for home-based HIV self-testing.43,52-55 While the healthcare field continues efforts to reduce healthcare stigma through diversity, equity, and inclusion initiatives, alternative LA-PrEP locations may help to fill a gap of unmet need. Hypothetical LA-PrEP at-home injections have also been identified as a stigma reduction strategy.27,56
High levels of enacted stigma experiences from friends and family were associated with a nearly 2-fold increase in preferring an HCP setting over a pharmacy. While it was not statistically significant, the same trend was noted in preference for home versus pharmacy. This preference away from pharmacies may be due to their inherently public nature, where one might be more likely to be seen by friends or family. While there is limited literature on non-HC setting location preferences for care receipt among MSM, what exists shows contradicting findings on preferences, but consistently highlights the important role of privacy.42,44,57 For example, a study with young Black MSM in the Deep South indicated a desire to receive HIV testing services at a private doctor's office as opposed to home-based care, in part due to concerns about privacy at home. 44 Another study, on HIV testing location preferences among MSM in Los Angeles, found a penchant for at-home testing over testing in a healthcare setting, due to increased geographic convenience and increased privacy. 42 A third study found that MSM were more likely to be comfortable discussing HIV testing, results, and care referrals in a pharmacy if there was a private room. 57 Taken together, this data highlights the importance of privacy in HIV testing and prevention services, which, for some, may be more inherent at an HCP office and/or home than a pharmacy.
Participants with private insurance were more likely to prefer an HCP setting or pharmacy than a home setting for LA-PrEP services. This could reflect a greater ease with which privately insured MSM may be able to access and pay for care outside of their home. Research about private health insurance coverage and healthcare access/usage has yielded mixed findings depending on the study population and comparison group.58,59 In a sample of US adults, individuals with employer-sponsored private insurance were more likely to have difficulty seeing a physician or taking medications because of costs than individuals with Medicare, but less likely to have difficulty than those with Medicaid. 58 Among people living with HIV in the United States, sustained viral suppression was more common among those with private insurance compared to the uninsured. 59 More research on the relationship between insurance type and service location preference among MSM is warranted.
We also found that participants who were 25 to 29 or 30 to 39 years old were significantly more likely to prefer receiving LA-PrEP injections at an HCP setting versus home compared to participants 40+ years old; a similar trend was noted among 18 to 24 year olds, but it was not statistically significant, perhaps due to small cell sizes. We are unaware of prior literature that helps to explain or contextualize this finding, which may be confounded or mediated by a third factor. Prior studies have examined the relationship between age and discrimination/stigma, which we hypothesize might be a mediator, given the significant stigma associations found.60-63 However, most of those studies have found that various types of discrimination and stigma are inversely associated with age, with younger MSM experiencing more stigma than older MSM, while, in our sample, higher levels of stigma were not associated with a preference for HCP over home.60-63 The opposite association was noted for high healthcare stigma, and high friends/family stigma was only associated with a preference for HCP setting compared to pharmacy, not home. Another hypothesis is that the age associations are confounded by duration on daily oral PrEP, and that those with longer PrEP experience may prefer being at home to the inconvenience of HCP visits. While we did find that older age was associated with being on PrEP for a year or longer, PrEP duration was not associated with location preference in our sample (data not presented). It is also possible that older people are simply more experienced at managing their own healthcare needs. Future research should more explicitly explore age, stigma, PrEP duration, healthcare management, and healthcare location preference.
Our findings, along with prior location preference research for HIV-related services,42,44,57,64 highlight the diversity of both location preference and the factors that may drive those preferences. Prior research on oral PrEP delivery and related care outside of traditional HCP settings shows the feasibility of pharmacy- and home-based PrEP services.65,66 Pharmacy-based PrEP services may address geographic barriers to accessing care by leveraging the existing infrastructure of community pharmacies; MSM have found pharmacies acceptable.67-69 While more research is required to confirm the efficacy of pharmacy-based PrEP services, they offer potential utility, given that community pharmacy initiatives for smoking cessation, weight management, and syringe exchanges have helped improve population health outcomes. 70 Home-based delivery of PrEP services is an emerging modality that has shown promise in addressing barriers related to accessibility, privacy, and convenience.71,72 Home-based HIV test kit interventions have shown consistent success in increasing testing rates among MSM. 64 Results of a pilot study providing MSM with at-home self-collection kits indicated high acceptability and an increased likelihood of PrEP care persistence, supporting the potential efficacy of home-based care. 73 It is important, however, to consider the potential exclusionary nature of home-based care due to the challenges some subgroups of MSM may face, including those who live with unsupportive family or room-mates and those who are unhoused.38,74,75 Taken together, these findings highlight the importance of providing multiple service delivery options, and the need for further research to better elucidate existing preferences among MSM populations.
Limitations
These results should be considered in light of several limitations. First, although the question about location preference was intended to be asked of all respondents who expressed willingness to use LA-PrEP if/when it became available, due to an error in the survey design and skip patterns, the study sample was limited to MSM who were currently using oral PrEP and expressed a strong intention to switch to LA-PrEP. This narrow subgroup does not include MSM who are not currently using PrEP or who may not have a strong interest in LA-PrEP, therefore findings may not be generalizable. Second, while our sample was demographically similar to the population of MSM using PrEP in the United States, 76 it is not representative of demographics of MSM who are at highest risk of HIV acquisition, 13 so additional research with a broader population of MSM is warranted. Third, it is important to note that, by definition, participants currently using PrEP are also currently connected to some type of HCP. Location preferences among MSM not currently engaged in care might differ. Fourth, the survey item for which our location preference outcome was derived allowed for only one response, and response options were not mutually exclusive. For example, an STD clinic might be part of a health center, and there could be private doctor's offices within both STD clinics and health centers. Therefore, we collapsed all HCP settings into one category, and, in doing so, we may have lost some nuance. Fifth, our analyses yielded wide confidence intervals for the prevalence ratio estimates for some less-frequently reported variables/characteristics, such as Hispanic ethnicity, age 15 to 24 years, and injection drug use, suggesting small sample sizes may have limited our ability to detect statistically significant associations. Finally, LA-PrEP had not been approved at the time of data collection, so all questions about LA-PrEP, including location preference, were hypothetical about a product that was unavailable; interest or intention for a hypothetical option may not directly transfer to currently available options. This limitation is true of any research examining stated preferences instead of enacted preferences, as notable variation may exist between what people prefer hypothetically and how they actually act when making decisions.
Conclusions
Our study investigated MSM location preferences for accessing LA-PrEP among a sample of MSM currently engaged in oral PrEP services provided at an HCP setting and found that nearly 40% of these men would prefer receiving LA-PrEP at an alternate location. Expanding LA-PrEP home-based and pharmacy-based models may also appeal to MSM indicated for PrEP but not currently engaged. We also explored the demographic factors, prior healthcare experiences, and stigma experiences that impact LA-PrEP location preference and found that age, type of insurance, healthcare and friend/family sexual behavior-stigma, prior oral PrEP source, and HIV testing locations were all significantly associated with location preference. Our findings support the need for multiple LA-PrEP service location options to effectively reach MSM and highlight multiple complex factors that might influence location choices. Future LA-PrEP location preference research with MSM who are not currently using PrEP will inform expanded options to improve PrEP uptake and coverage among a wider group of MSM.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank all of the men who participated in the AMIS study and the full AMIS research team.
Data Availability
Data cannot be shared publicly because of the sensitive nature of the data. Data are available from the first author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Study funding was provided by Viiv Healthcare, makers of LA-PrEP.
Ethics Approval and Consent to Participate
Activities were approved by the Emory institutional review board- MOD0037-IRB00047676. Participants provided informed consent, via an online survey check box.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by ViiV Healthcare. ViiV co-authors are employees of ViiV Healthcare and hold stock in GSK as part of their employment.