
Abstract
Background
The United States recently expanded infant feeding guidelines for persons living with HIV to include chest/breastfeeding.
Methods
A qualitative study was conducted through in-depth interviews with 15 service providers and 7 pregnant/lactating persons living with HIV about infant feeding preferences/experiences and implementation determinants of the revised guidelines. Thematic analysis, guided by the Health Equity Implementation Framework, identified opportunities and constraints to equitable adoption and implementation of the revised infant feeding guidelines for persons living with HIV in the United States.
Results
Providers and persons living with HIV embraced the revised guidelines, citing expanded autonomy in infant feeding choices, destigmatization and normalization of breastfeeding. Nevertheless, overlapping individual (breastfeeding reticence given quantifiable but residual vertical HIV transmission risks), institutional (inconsistent provider/organizational knowledge and resources), and structural (siloed care) implementation barriers were identified.
Conclusions
Equitable guideline rollout should consider person-centered counseling, clear communication around risks, and coordinated public sector-led dissemination.
Keywords
Introduction
Chest/breastfeeding (henceforth referred to as “breastfeeding”) provides many immediate and long-term benefits for both the infant and birthing parent. Human milk supports the infant's developing immune system, 1 and breastfeeding is associated with a lower risk of sudden infant death syndrome, improved cognitive development, and decreased risk of type 2 diabetes in childhood and adolescence.2–10 For the birthing parent, breastfeeding can reduce postpartum bleeding, decrease the risk of cardiovascular disease as well as breast and ovarian cancers, and improve infant bonding.5,11–15 This risk reduction is particularly important for Black and Hispanic/Latine birthing parents and their infants, who are disproportionately affected by these health conditions as well as HIV in the United States.16,17
However, clinical guidelines on breastfeeding for persons living with HIV have been globally disparate for years. 18 The World Health Organization (WHO) has long endorsed breastfeeding among persons living with HIV in resource-constrained environments, as the benefits of breastfeeding in these settings (eg, immune protection and nutrition in the context of high infant mortality, unavailability of infant formula) generally outweigh the risks of vertical HIV transmission. 19 By comparison, guidelines in the United States and resource-rich countries historically have discouraged persons living with HIV from breastfeeding to avert potential vertical HIV transmission risks, especially in the presence of safe, reliable, and accessible alternative feeding options for infants (ie, infant formula, pasteurized donor human milk). 20
When infant feeding guidelines for persons living with HIV in the United States were first published in 1985, the probability of vertical HIV transmission through breastfeeding was 15% to 20% from birth to 2 years of age.21,22 These guidelines, critically, predated the widespread availability and coverage of antiretroviral therapy (ART). In the absence of adequate evidence or interventions to support safe breastfeeding among persons living with HIV, healthcare providers discouraged breastfeeding as an infant feeding option for pregnant and lactating persons living with HIV, effectively restricting their capacity to breastfeed. 23 For some persons living with HIV, specifically those immigrating to the United States from lower-income countries, these breastfeeding restrictions have amplified sentiments of deculturization, as breastfeeding has been long-endorsed by clinical guidelines and, in many cases, is expected of birthing parents in resource-poor countries. 24 Ultimately, physiological, sociocultural, and structural forces shape infant feeding decision-making for persons living with HIV, specifically the appropriateness and relevance of breastfeeding.16,25,26
In January 2023, the U.S. Department of Health and Human Services (DHHS) revised its Perinatal HIV Guidelines, recommending that persons living with HIV on ART with sustained viral load suppression (<200 RNA copies/mL), at least during the third trimester of pregnancy and at the time of delivery, receive counseling on breastfeeding as an infant feeding option and be supported to breastfeed if they choose to do so. 27 These updated guidelines have since (May 2024) been endorsed by the American Academy of Pediatrics (AAP), 28 reflecting current evidence that improved access to ART during pregnancy, coupled with viral load suppression and neonatal antiretroviral prophylaxis, reduces the risk of HIV transmission through breastfeeding to <1%,20,28 which a recent systematic review revised to ≤0.2%. 29 These updated guidelines more explicitly center equity by extending the health benefits of breastfeeding to persons living with HIV and their infants while enabling greater autonomy in infant feeding decision-making. 18 This approach can also address long-standing health inequities faced by Black and Hispanic/Latine birthing parents in the United States, who are disproportionately affected by HIV and often receive inadequate support for breastfeeding.16,30
Given the recency with which the revised infant feeding guidelines were published, few studies have interrogated the facilitators and barriers to their equitable adoption and implementation in various practice settings in the United States. A recent survey of U.S. pediatric infectious diseases providers revealed inconsistencies in knowledge and application of the revised infant feeding guidelines, with some providers expressing implementation reticence due to perceived evidence gaps supporting the safety of breastfeeding for persons living with HIV and a dearth of implementation blueprints. 31 Equitably implementing these guidelines ensures that persons living with HIV and their infants can equally experience the benefits of informed infant feeding choices, including breastfeeding—to which they have long been denied in the United States.20,32,33 We present a qualitative study aiming to identify opportunities and constraints to equitable adoption and implementation of the revised infant feeding guidelines for pregnant and lactating persons living with HIV in the United States.
Methods
Study Design
Following the publication of the DHHS and AAP revisions to the U.S. infant feeding guidelines for persons living with HIV, we conducted qualitative research in one metropolitan area in the U.S. Mid-Atlantic region. Data collection and analyses were theoretically grounded in the Health Equity Implementation Framework (HEIF),34,35 which situates the implementation determinants of clinically delivered “innovations” (eg, treatments, therapies, policies, guidelines) into a nested socioecology of theorized health equity antecedents (see Figure 1). Our interdisciplinary research team included clinicians and public health researchers, none of whom were persons openly living with HIV, with expertise in pediatric and adult infectious diseases (AMP, AL, ALA, MGF, LRC, AJR, JGR), obstetrics and gynecology (HS, AMP, AL, AJR), neonatology (WCG), and maternal/child nutrition (AJB, HS, SMG).

The Health Equity Implementation Framework.
Sampling
In February–September 2024, health providers (none of whom were openly living with HIV) and pregnant/lactating persons living with HIV from a city in the U.S. Mid-Atlantic region were sampled purposefully 36 to participate in one-time, semistructured, in-depth interviews. Adult (aged 18+ years) healthcare and nutrition service providers with direct experience interfacing with pregnant and/or postpartum persons living with HIV were initially approached through targeted outreaches to healthcare facilities with services tailored to persons living with HIV and their infants. Leveraging their professional networks and contacts, study investigators (AMP, SMG, ALA, WCG, MF, AJR) disseminated recruitment materials to clinical and program directors in heterogeneous practice settings, directing potentially eligible providers to contact trained qualitative interviewers (AJB, HS, AP, JGR) to verify eligibility for participation.
Pregnant and lactating persons living with HIV were recruited via convenience sampling 36 from a single clinic specializing in antenatal and postpartum care for persons living with HIV. Clinic-based providers and counselors (AMP, AL) disseminated study information to potentially eligible patients, and persons expressing interest in the study were connected in the clinic to a study team member (AJB, BW), who explained the purpose of the research and administered a structured screening form to verify eligibility. Persons living with HIV were enrolled in the study if they: (i) were aged 18+ years, (ii) were assigned female sex at birth, (iii) self-reported living with HIV or received an HIV diagnosis from a healthcare provider, and (iv) reported a current or recent (past 24 months) pregnancy following their HIV diagnosis.
Data Collection
Participants completed one 30 to 60-min interview with 1 of 4 trained qualitative interviewers (AJB, HS, AP, JGR) via secure video-conferencing platform (providers only), face-to-face in a private space at the clinic (persons living with HIV only), or telephone (persons living with HIV only). A semistructured interview guide was developed, organized around domains from the HEIF, and used for the interviews with providers, focusing on their experiences providing infant feeding counseling to persons living with HIV, initial impressions of the revised infant feeding guidelines, anticipated challenges implementing the revised guidelines, and solutions to optimize adoption and sustained implementation of the guidelines (see Supplemental File 1). As not all providers may have been aware of the updated guidelines, interviewers provided a brief description of the guideline revisions to enrich conversation. Additionally guided by the HEIF, a semistructured interview guide was also developed and used for the interviews with persons living with HIV, with questions that elicited experiences with pregnancy and infant feeding (including clinical care and counseling), impressions of the revised HIV infant feeding guidelines, and future infant feeding intentions in the context of the revised guidelines (see Supplemental File 2). Persons living with HIV were also asked questions from a brief structured survey before the interview. No questions were directed to providers or persons living with HIV to establish whether they had preexisting relationships with one another. To iteratively refine interview guides in parallel with data collection, interviewers met weekly with the Principal Investigator (JGR), as well as monthly with the broader investigative team, to discuss burgeoning themes and propose requisite updates to the semistructured guides. The interviewers also practiced reflexivity throughout the study, reflecting on and discussing relationships between study participants and themselves and how those relationships may have shaped the content and structure of the interviews. 37
Persons living with HIV received financial compensation in the form of a $50 gift card for their participation, but clinical providers were not compensated for completing an interview. Interviews were audiorecorded, transcribed verbatim using artificial intelligence-powered software, and reviewed by a study team member (BW) for deidentification and fidelity to the recorded dialog.
Analysis
Textual data were synthesized using team-based, iterative thematic analysis, 38 implemented concurrently with data collection to guide subsequent revisions to the semistructured interview guides. First, guided by the tenets of rapid qualitative analysis,39,40 study team members (AJB, HS, AP) abstracted emerging insights from transcripts by populating summative data matrices, organized by thematic constructs derived deductively from the semistructured guides and the HEIF. Summative insights were then transformed into inductive codes through synchronous (during weekly team discussions) and asynchronous (independently through analytic memoing) textual sorting tasks (ie, labeling and consolidation of themes). One study team member (AJB) then applied these inductive codes to transcript text segments in Dedoose version 9 (SocioCultural Research Consultants LLC, Manhattan Beach, CA).
Next, text segments were exported and repositioned deductively onto domains from the HEIF (see Figure 1), mining and integrating coded text from persons living with HIV and providers for data triangulation (dependability and confirmability). 41 The HEIF facilitated (re)organization of emerging enablers and constraints to equitable implementation of the revised infant feeding guidelines (ie, the “innovation”) across heterogeneous clinical and practice contexts. Accordingly, these determinants of implementation equity were structured at the recipient (ie, patient), deliverer (ie, provider), organizational (ie, clinic, hospital), and systems (ie, healthcare network/infrastructure) levels. To further enhance the credibility and confirmability of findings, 41 emerging insights were discussed among the broader study team and convened practitioners (member checking) to guide evolving interpretations and crystallize salient data patterns.
Ethical Approval and Informed Consent
This study protocol was reviewed and approved by the Johns Hopkins University Bloomberg School of Public Health Institutional Review Board (No. 00026827). All individuals provided verbal informed consent prior to study enrollment, which was witnessed and documented by a trained study interviewer.
Results
A total of 22 in-depth interviews were conducted, including with 15 healthcare and nutrition service providers as well as 7 persons living with HIV. Healthcare and nutrition service providers represented a range of professional backgrounds: infectious disease physicians and nurse practitioners (n = 4), pediatricians and pediatric nursing professionals (n = 3), breastfeeding coordinators and lactation-specializing nurses (n = 3), obstetricians and gynecologists (n = 3), and HIV nurse managers (n = 2).
The 7 persons living with HIV interviewed were all cisgender women. Six were pregnant at the time of the interview, and one was postpartum; their ages ranged from 25 to 39 years, with a median age of 33 years (see Table 1). Nearly all identified as non-Hispanic Black (n = 6), and 2 had university-level education. Five were enrolled in the Special Supplemental Program for Women, Infants, and Children (WIC). Participants were living with HIV for 1 to 27 years, with a median of 6 years. Most expressed intentions to breastfeed their infants (n = 5).
Demographic and Healthcare Characteristics of Interviewed Pregnant and Postpartum Women Living With HIV (n = 7).
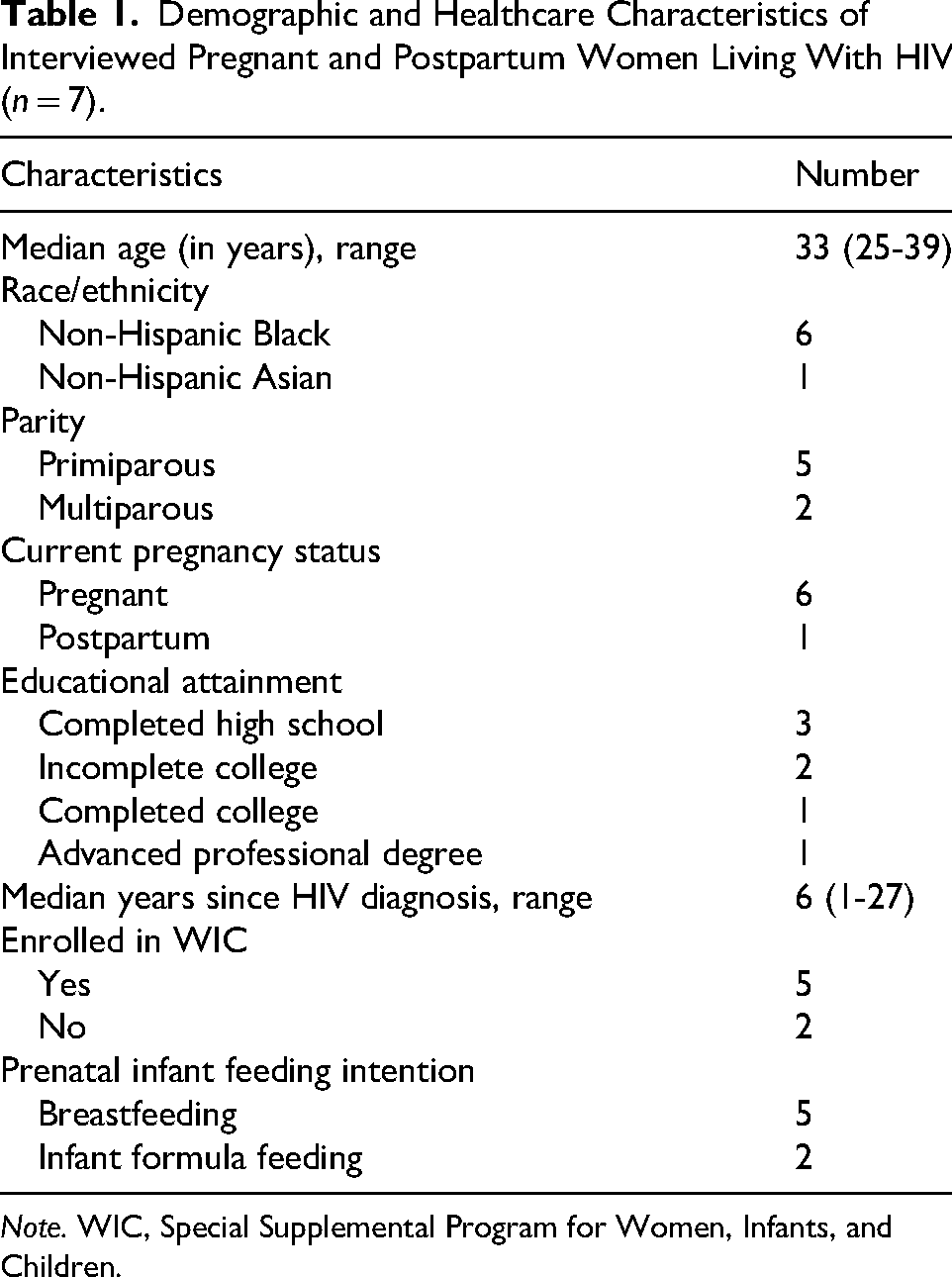
Note. WIC, Special Supplemental Program for Women, Infants, and Children.
Salient opportunities and constraints to the timely, equitable rollout and universal adoption of the revised infant feeding guidelines were identified and summarized according to HEIF domains at the recipient, organizational, and systems levels (see Figure 2).
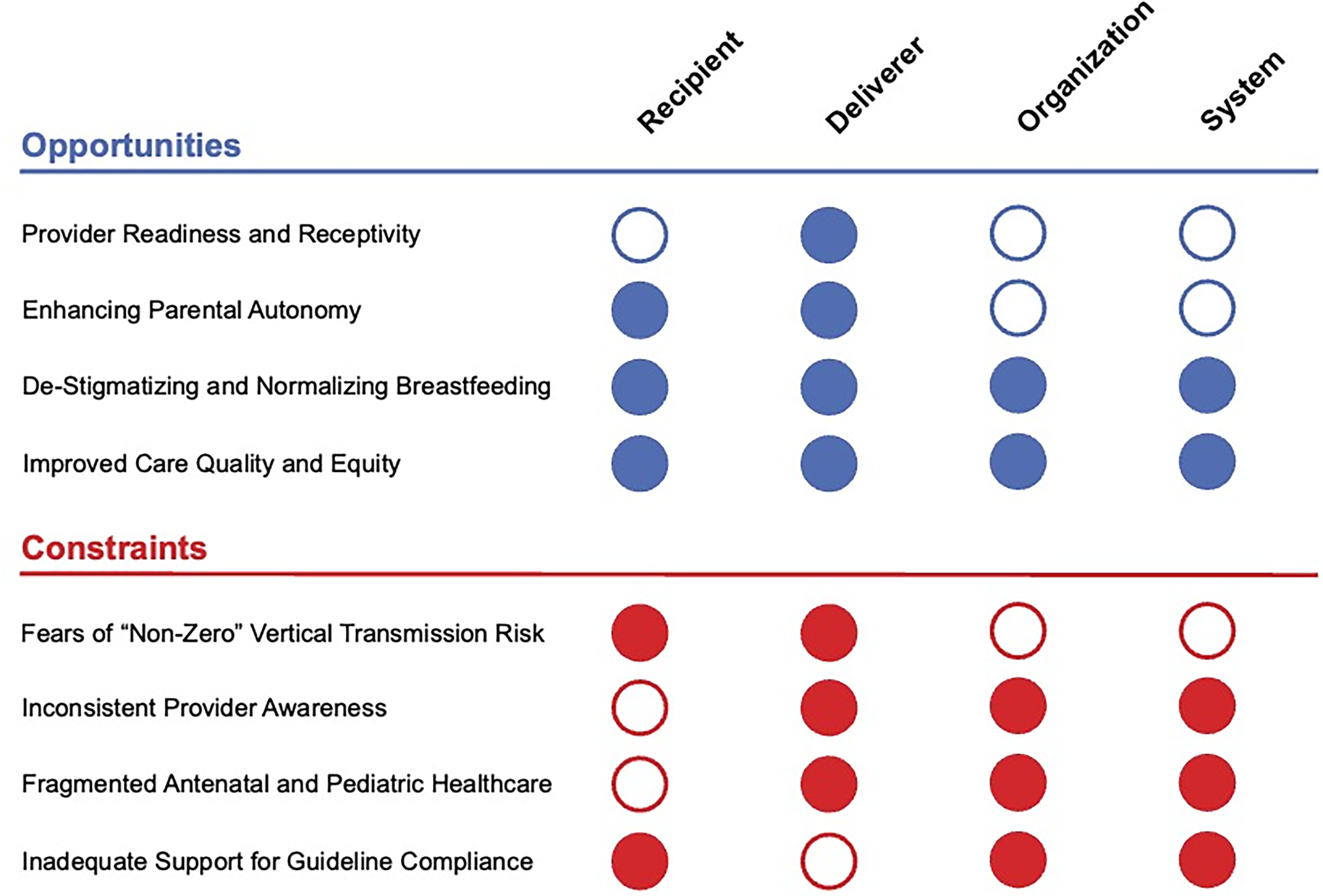
Emerging Opportunities and Constraints to the Equitable Implementation of the Revised U.S. HIV Infant Feeding Guidelines, Mapped to HEIF Constructs.
Opportunities for Equitable Implementation of the Revised Infant Feeding Guidelines
Provider Readiness and Receptivity
Both providers and persons living with HIV welcomed the revised infant feeding guidelines and generally reacted positively to guideline updates (HEIF domains: deliverer). Providers unanimously endorsed willingness to support persons living with HIV to breastfeed their infants, in accordance with the updated infant feeding recommendations. These positive reactions demonstrate providers’ readiness and motivation to support breastfeeding goals among persons living with HIV, as one lactation consultant explained: It backs us up when we say that we can support women with HIV and breastfeeding their infants. It helps us to be able to show the guidelines and that we are following them … because a lot of our population is not 100% healthy. It's good now that the guidelines have changed. They’re actually encouraging breastfeeding because it really makes a difference in mothers living with HIV because they can get so discouraged if that is something they want to do.
Enhancing Parental Autonomy
Both persons living with HIV and providers described how expanded infant feeding options through the revised infant feeding guidelines could facilitate more active participation among persons living with HIV in infant feeding decision-making with their healthcare team (HEIF domains: recipient, deliverer). Even in the absence of breastfeeding intentions, pregnant and lactating participants acknowledged the numerous benefits of breastfeeding, specifically improved infant health and nutrition of their infant as well as infant bonding. For example, a 38-year-old postpartum woman living with HIV emphasized the importance of breastfeeding to bond with her infant, saying: “The biggest thing was the benefits from breast milk. A lot of that is bonding as well … building that bond between the baby and mom.” Weighing different infant feeding options, a 33-year-old pregnant woman living with HIV shared her distrust of infant formula, asserting that her own breast milk—even in the context of minimal but quantifiable vertical HIV transmission risks—would be safer for her infant to consume: I feel like there's a lot of stuff going on with these formulas like recalls. I feel like the best thing for me to do is breastfeed. I feel like my body is more safe than actual formula because there's been a lot of stuff going on with formula. Before, we advised against [breastfeeding], and there's the risk [of vertical HIV transmission]…But now, it feels okay. ‘These are your options, and these are the things we think about with these options.’ And I think that gives somebody a choice and power … I think it's empowering.
Destigmatizing and Normalizing Breastfeeding
Providers anticipated that implementing the revised infant feeding guidelines could help destigmatize breastfeeding for persons living with HIV (HEIF domains: recipient, deliverer, organization, system). Persons living with HIV who breastfeed regularly confronted judgment from clinical professionals, their communities, and their families—navigating sentiments of shame associated with their infant feeding choices in the context of their HIV status or, in other cases, using infant feeding choices as a mechanism to conceal their HIV status. Given the revised guidelines’ permissiveness towards breastfeeding, providers anticipated this would normalize and, subsequently, mitigate breastfeeding stigma among persons living with HIV. A pediatrician elaborated on this hope, stating: I suspect that [stigma] could be reduced if … our leading professional organization encourages or recommends that women breastfeed who are able to … I imagine without that stamp of approval … women are treated differently and negatively by providers or in the healthcare system.
Improved Care Quality and Equity
Providers reported eagerness to adopt the revised infant feeding guidelines, expressing interest in providing care that allows persons living with HIV to share in the health benefits of breastfeeding historically availed to other persons not living with HIV (HEIF domains: recipient, deliverer, organization, system). As one pediatric nurse explained, the revised guidelines enable providers to deliver services and care that empower persons living with HIV to make critical, intimate decisions about infant feeding: I think the sense of normalcy that [the guidelines] give them [persons living with HIV] … plus the advancement of HIV care allows them to live an extended life. They can be moms. They can know that their babies will be breastfed like other people's babies. I think the advancement has been extremely good for them, as people and mothers and parents and partners.
Constraints to Equitable Implementation of the Revised Infant Feeding Guidelines
Fears of “Nonzero” Vertical Transmission Risk
Both providers and persons living with HIV discussed breastfeeding reticence in the context of quantifiable, albeit residual, risks of vertical HIV transmission (HEIF domains: recipient, deliverer). Most interviewed providers explained that concerns related to vertical HIV transmission are realities that must be considered during infant feeding counseling with birthing parents. Despite the minimal likelihood (≤0.2%) of vertical HIV transmission in the context of viral load undetectability,20,28 the presence of “nonzero” transmission risks induced anxiety for both providers and persons living with HIV. A 27-year-old pregnant woman who acquired HIV perinatally expressed apprehension toward breastfeeding, sharing that the quantifiability of the vertical transmission possibility motivated her to formula feed her newborn. Even if there's medication that is protecting the child, they still tell you that [there is a] 1% chance that something can happen, God forbid … I don't even want that 1% chance. Yes, breastfeeding is good, but I cannot take the risk … That made me go more on formula feeding, which started me and my partner doing research. There are many who are interested and would like to [breastfeed] but don’t want to take that tiny, tiny risk … I think more people would breastfeed if they felt like there wasn’t that risk—that it was not zero risk. If they felt like it was ‘undetectable equals untransmittable,’ then they would breastfeed. My biggest concern would be for the parent who chooses to breastfeed and then down the road, their child becomes a person who's living with HIV … It's not something that you’re going to be able to pinpoint to breastfeeding … In talking to people who are more knowledgeable about this and educating myself in the field … I’ve learned a lot more about HIV … I’m confident that if people want to make these decisions [to breastfeed], that's fine.
Inconsistent Provider Awareness
As with any changes to clinical guidelines, communication delays and bottlenecks in the dissemination pipeline are expected to drive lags in institutional and practice adoption (HEIF domains: deliverer, organization, system). Several providers expressed that their colleagues—even within their same institutions—may not be privy to or aware of the revised infant feeding guidelines. Providers anticipated that the velocity of the guideline adoption would vary across clinical settings, with academic hospitals/clinics likely to adopt the revised guidelines more swiftly than lower-threshold, community-based clinics (eg, federally qualified health centers) with fewer resources allocated to research and practice optimization. Other providers also anticipated that less experienced clinicians may have more difficulty implementing the revised guidelines, especially if they observe discordant practices from more seasoned providers. One lactation consultant shared her concerns, stating: I know there are providers out there who don’t know about the change. We tripped across it and found out. And my counterparts … were like, ‘Wait, how did you find this out?’ And now they’re all spreading the word as well. But there's always going to be somebody who may not know that this change has occurred, and that's going to make it more difficult for parents. They’re going to hear multiple things from multiple people, not knowing who to believe. You see this one [clinician], who tells me this [breastfeeding] is the right way. Then another one tells you a different thing. It is more confusing and annoying because they [clinicians] are not on the same page.
Fragmented Antenatal and Pediatric Healthcare
Several newborn and pediatric care providers expressed concerns about their capacity to adequately counsel persons living with HIV about infant feeding in the context of highly siloed antenatal and pediatric healthcare (HEIF domains: deliverer, organization, system). Unable to access health records (ie, viral load, ART adherence, clinical history) from the birthing parent, providers felt restricted in their capacity to provide appropriate infant feeding support to birthing parents during newborn or pediatric clinical encounters. Multiple providers cited challenges verifying or validating birthing parents’ health information while acknowledging the inherent paternalism of providers’ mistrust of mothers and birthing parents during clinical encounters with their newborns. One pediatrician stated: I wouldn’t actually have a sense if a parent's viral load is undetectable. Since I'm not the parent's clinician, and I’m often meeting them for the first time because this might be their first baby, I don’t have a sense of their risk of being non-adherent with their medication and having a detectable viral load …. But at the end of the day, in pediatrics, we’re so paternalistic … you do have to let a parent have some agency in deciding what's appropriate.
Inadequate Support for Guideline Compliance
The revised infant feeding guidelines stipulate that breastfeeding persons living with HIV will require close medical monitoring and strict compliance with scheduled clinical visits, which may be challenging for persons living with HIV with competing obligations (eg, employment, caregiving) and resource constraints (HEIF domains: recipient, organization, system). Some providers, like the lactation consultant below, anticipated that in the absence of supplemental support to persons living with HIV who breastfeed (eg, transportation vouchers, telemedicine or home healthcare), some birthing parents—especially the most disenfranchised—may confront insurmountable social and structural barriers to guideline compliance, making some providers apprehensive about counseling persons living with HIV about breastfeeding as an infant feeding option: An honest conversation about the commitment level that it [breastfeeding]takes [is important] because I never want anyone to go into it thinking it's just like any other breastfeeding situation. There is a lot more to it than that … I think when they [persons living with HIV] hear how much work is going to go into it, it may scare them off a little bit.
Discussion
The revised U.S. infant feeding guidelines avail new opportunities and constraints related to equitable counseling of persons living with HIV on breastfeeding during clinical encounters—reflected in institutional policies and buttressed by structural factors, as articulated in the HEIF.34,35 Ultimately, these updated guidelines provide new avenues to advance health equity for persons living with HIV and their infants in the United States, but if they are not implemented with fidelity and fairness, existing inequities may be aggravated.
The revised U.S. infant feeding guidelines are now more aligned with the recommendations from Switzerland and the United Kingdom. The Swiss infant feeding recommendations were revised in 2018 to support birthing parents who want to breastfeed as part of a shared decision-making process, as long as they are adherent to ART and remain virally suppressed with close postpartum monitoring. 42 An observational study of 41 birthing parents in Switzerland following the 2018 guideline update found that over half decided to breastfeed, and no cases of vertical HIV transmission were documented. 43 In the United Kingdom, the British HIV Association recommends exclusive formula feeding as the safest option for infants born to persons living with HIV. 44 However, in 2025, the guidelines were updated to recommend shared patient/provider decision-making around infant feeding and support of birthing parents who choose to breastfeed, if they are virologically suppressed and adhering to ART during pregnancy; this recommendation includes regular monitoring of the viral loads of both the birthing parents and their infants. 44 Both the United States and United Kingdom infant feeding guidelines recommend exclusive human milk feeding for persons living with HIV who choose to breastfeed.27,44
We identified several opportunities to equitably implement the revised infant feeding guidelines for persons living with HIV. Both providers and persons living with HIV were enthusiastic about the potential to destigmatize and normalize breastfeeding for persons living with HIV while enhancing parental autonomy over infant feeding practices. These findings reify the potency of injunctive norms and HIV stigma attributed to formula feeding in shaping preferences for breastfeeding among persons living with HIV.45,46 Previous studies have highlighted how persons living with HIV in high-income countries—including the United States, Canada, and the United Kingdom—experience complex emotions around perceived social pressures to breastfeed, desires to be a “good mother,” and concerns surrounding the residual but nonzero likelihood of HIV transmission via breastfeeding as they make infant feeding choices.47–49 Clinicians also experience challenges providing autonomy-centered counseling of pregnant or postpartum persons living with HIV, navigating tensions between the well-documented benefits of breastfeeding for infants and birthing parents and the potential likelihood of vertical HIV transmission associated with breastfeeding.50,51 Autonomy, a foundational principle in medical ethics, 52 plays an important role in parental infant feeding decision-making and is a documented facilitator of breastfeeding, 45 reaffirming the importance of provider communication about the benefits and relative risks of breastfeeding for persons living with HIV. 53 To support the equitable implementation of the revised guidelines, counseling must avoid a myopic focus on the clinical benefits of breastfeeding and should be person-centered, acknowledging the sociocultural meanings and values of breastfeeding for persons living with HIV.
Persons living with HIV and provider narratives also uncovered anticipated barriers to equitable adoption of the revised guidelines, most saliently concerns about inadvertently exposing infants to HIV through breastfeeding. While many pregnant women expressed breastfeeding preferences, most acknowledged the quantifiable, albeit residual, risks of vertical HIV transmission associated with breastfeeding, prompting some participants to declare exclusive formula-feeding intentions. These findings align with other U.S. studies predating the revised infant feeding guidelines, which found perceived vertical HIV transmission risks underpinned formula-feeding intentions among persons living with HIV.45,46,54 Likewise, studies in Botswana, South Africa, and Uganda have shown that some persons living with HIV, inconsistent with clinical recommendations, opted to formula feed instead of breastfeed because they feared unintentionally exposing their newborns to HIV.45,55–57 Taken together, these findings highlight the importance of effective risk communication during clinical encounters with persons living with HIV to appropriately align their anxieties about vertical HIV transmission with available safety evidence about breastfeeding in the context of HIV care engagement.
While the probability of HIV transmission through breastfeeding is negligible when the lactating parent is virally suppressed through sustained ART adherence,20,28 “undetectable equals untransmittable” (U = U) has not yet been established for breastfeeding due to insufficient study of vertical HIV transmission risks relative to formula feeding.20,29 Communicating uncertainty can be challenging for providers, especially when explaining the probabilities of future outcomes,58,59 and overemphasizing the risks of HIV transmission through breastfeeding could unfairly discourage persons living with HIV from breastfeeding who might otherwise benefit from it. To ensure the equitable implementation of the revised infant feeding guidelines, it is essential that communication demystify the “residual” risks of HIV transmission associated with breastfeeding. Providers may benefit from training in effective risk communication, which involves judicious articulation of vertical HIV transmission risks in the context of well-established benefits of breastfeeding.
Our study also highlighted a cross-cutting barrier to the equitable implementation of the revised infant feeding guidelines: systems-level bottlenecks to supporting guideline compliance. Inconsistent provider knowledge, competencies, and institutional resources, including limited access to training on the updated infant feeding guidelines or insufficient staffing for breastfeeding support in clinical settings (especially in lower-threshold service delivery environments) contribute to these inadequacies. Compounding this issue is the fragmentation of antenatal and pediatric care, which further contributes to knowledge gaps and inconsistent care practices regarding infant feeding counseling and support for persons living with HIV and their infants. This issue, as documented by others as gaps in perinatal HIV services for persons living with HIV and their infants,60,61 creates silos that impede the delivery and coordination of care that are essential to implementation equity of the revised infant feeding guidelines.
Addressing these systemic barriers requires a coordinated, family-centered care approach. This approach treats families as partners and collaborators, 62 prioritizing the birthing parent-infant dyad 63 and ensuring coordinated care from antenatal to pediatric care providers and nutrition safety net services like WIC or the Supplemental Nutrition Assistance Program.27,64 Coordination between public sector institutions (ie, health departments), professional associations, and healthcare institutions—enhanced through learning collaboratives or other multidisciplinary interest-groups 65 —will be critical to equitable dissemination and implementation of the revised guidelines, ensuring that persons living with HIV, irrespective of provider or healthcare practice environment, have the opportunity to receive timely, accurate, and high-quality infant feeding counseling.16,26,46,54
Limitations
Study findings should be considered with some limitations in mind. First, findings may have limited transferability to other clinical settings, as we recruited a convenience sample of persons living with HIV from one clinic specializing in antenatal/postpartum care for persons living with HIV. The healthcare institution in which this clinic is nested has been certified by the Baby-Friendly Hospital Initiative 66 through accredited implementation of the WHO's 10 Steps to Successful Breastfeeding 67 —indicating a strong culture of breastfeeding support among its providers and institutional policies limiting infant formula provision. In the United States, only one-quarter of births occur in certified Baby-Friendly facilities. 66 Second, the small sample of persons living with HIV included in this study may not be fully representative of the diverse identifies of pregnant and postpartum persons living with HIV in the United States, attenuating the likelihood of achieving data saturation and potentially limiting the transferability of our findings. Third, while the hybrid inductive-deductive analytic approach enables detection of pertinent themes unrelated to the guiding conceptual framework, study findings and accompanying interpretations may have been constrained by data collection instruments and analytic inputs that overemphasized domains and constructs from the HEIF. Fourth, well-documented barriers to breastfeeding among persons living with HIV in other contexts (eg, anticipated or expected intimate partner violence, loss of child custody) may not have emerged in the present study because the interview guides intentionally avoided probing around these highly sensitive topics. Lastly, the present study was conducted in one mid-sized urban area in the U.S. mid-Atlantic region. Future studies could benefit from greater geographic (ie, Midwest and Southeast), residential (ie, rural and semiurban areas), and sociodemographic diversity—including representation of persons living with HIV on the investigative team. While providers in the present study generally articulated support for the revised HIV infant feeding guidelines, future scholarship, particularly with greater geographic and cadre representation, may be needed to confirm these findings.
Conclusions
There is tremendous promise to advancing health equity for persons living with HIV and their infants by promoting breastfeeding, as supported by the revised U.S. infant feeding guidelines. The present study highlights the excitement among some providers and persons living with HIV for the potential to destigmatize breastfeeding and enhance parental autonomy through the revised infant feeding guidelines. However, equitably implementing these guidelines requires addressing several key barriers. Effective risk communication is crucial to mitigate fears surrounding any residual vertical HIV transmission risks through breastfeeding. Providers should be capacitated to provide consistent, balanced, person-centered counseling on the risks and benefits of breastfeeding, acknowledging the sociocultural meanings of breastfeeding for persons living with HIV and adapting with agility to a birthing parent's evolving infant feeding preferences, whether breastfeeding or formula feeding. Lastly, coordinated, public sector-led dissemination of the revised guidelines is critical to optimizing equity in guideline rollout—ensuring persons living with HIV and their infants across clinical practices can benefit from informed, autonomous infant feeding choices.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251396636 - Supplemental material for Opportunities and Constraints to Equitable Implementation of the Revised Infant Feeding Guidelines for Pregnant and Lactating Persons Living With HIV in the United States: A Qualitative Study
Supplemental material, sj-docx-1-jia-10.1177_23259582251396636 for Opportunities and Constraints to Equitable Implementation of the Revised Infant Feeding Guidelines for Pregnant and Lactating Persons Living With HIV in the United States: A Qualitative Study by Audrey J Buckland, Helen Schmedtje, Abinethaa Paramasivam, Anna M Powell, Alison Livingston, Susan M Gross, Allison L Agwu, W Christopher Golden, Mary Glenn Fowler, Laura R Clark, Christina Bunch, Beatrice Wendling, Andrea J Ruff and Joseph G Rosen in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251396636 - Supplemental material for Opportunities and Constraints to Equitable Implementation of the Revised Infant Feeding Guidelines for Pregnant and Lactating Persons Living With HIV in the United States: A Qualitative Study
Supplemental material, sj-docx-2-jia-10.1177_23259582251396636 for Opportunities and Constraints to Equitable Implementation of the Revised Infant Feeding Guidelines for Pregnant and Lactating Persons Living With HIV in the United States: A Qualitative Study by Audrey J Buckland, Helen Schmedtje, Abinethaa Paramasivam, Anna M Powell, Alison Livingston, Susan M Gross, Allison L Agwu, W Christopher Golden, Mary Glenn Fowler, Laura R Clark, Christina Bunch, Beatrice Wendling, Andrea J Ruff and Joseph G Rosen in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-3-jia-10.1177_23259582251396636 - Supplemental material for Opportunities and Constraints to Equitable Implementation of the Revised Infant Feeding Guidelines for Pregnant and Lactating Persons Living With HIV in the United States: A Qualitative Study
Supplemental material, sj-pdf-3-jia-10.1177_23259582251396636 for Opportunities and Constraints to Equitable Implementation of the Revised Infant Feeding Guidelines for Pregnant and Lactating Persons Living With HIV in the United States: A Qualitative Study by Audrey J Buckland, Helen Schmedtje, Abinethaa Paramasivam, Anna M Powell, Alison Livingston, Susan M Gross, Allison L Agwu, W Christopher Golden, Mary Glenn Fowler, Laura R Clark, Christina Bunch, Beatrice Wendling, Andrea J Ruff and Joseph G Rosen in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We thank all study participants for generously sharing their time, candor, and insights. We also acknowledge Schuyler Blee for supporting initial conceptualization of the study and development of data collection instruments.
Ethical Approval and Informed Consent
This study protocol was reviewed and approved by the Johns Hopkins University Bloomberg School of Public Health Institutional Review Board (No. 00026827). All individuals provided verbal informed consent prior to study enrollment, which was witnessed and documented by a trained study interviewer.
Consent to Participate
All individuals provided verbal informed consent prior to study enrollment.
Authorship Contribution Statement
AJB: conceptualization, formal analysis, investigation, methodology, project administration, writing—original draft, and writing—review and editing; HS: formal analysis, investigation, writing—original draft, and writing—review and editing; AP: formal analysis, investigation, and writing—review and editing; AMP: methodology, resources, and writing—review and editing; AL: resources, and writing—review and editing; SMG: methodology, resources, and writing—review and editing; ALA: methodology, resources, and writing—review and editing; WCG: methodology, resources, and writing—review and editing; MF: methodology, resources, and writing—review and editing; LRC: project administration, resources, and writing—review and editing; CB: project administration, resources, and writing—review and editing; BW: data curation, project administration; and writing—review and editing; AJR: conceptualization, methodology, resources, supervision, and writing—review and editing; JGR: conceptualization, data curation, funding acquisition, investigation, methodology, supervision, visualization, and writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the National Institute of Mental Health and the Johns Hopkins University Center for AIDS Research (CFAR), a program of the National Institute of Allergy and Infectious Diseases (Grant Nos. R25MH083620 and P30AI094189). The contents of this article are solely the responsibility of the authors and do not necessarily represent the official position of the NIH.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JGR serves as a paid consultant to the Elizabeth Glaser Pediatric AIDS Foundation on an evaluation of efforts to integrate HPV vaccination into adolescent HIV services, funded by Gavi, the Vaccine Alliance. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data generated from the present study are not publicly available. However, the corresponding author can make deidentified data available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.