
Abstract
Objective
To identify the correlates of early breastfeeding (BF) cessation and breastmilk expression (BE) among mothers 12 months after childbirth.
Methods
We used a case-control study design to compare characteristics between mothers who stopped BF and expressed breastmilk 12 months after childbirth in Uganda. BF practices were determined in 12-month follow-up interviews using an adapted World Health Organization infant feeding questionnaire. Univariate and bivariate logistic regression models identified correlates of early BF cessation and BE as distinct but related outcomes.
Results
The odds of early BF cessation were higher among mothers who expressed breastmilk irrespective of maternal age (adjusted odds ratio: 2.82; 95% confidence interval: 1.39, 5.68). Mothers who stopped BF and did not express breastmilk were more likely to be older than those who continued BF and did not express breastmilk during the first 12 postpartum months.
Conclusion
Mothers living with human immunodeficiency virus infection have disproportionately high odds of early BF cessation that may contribute to disparities in child health outcomes. Promotion of safe BF practices coupled with family and social support could be a viable preventive strategy for attenuating such disparities, especially among young mothers at risk of early BF cessation.
Keywords
Introduction
The 2016 World Health Organization (WHO) guidelines 1 recommend that “mothers living with HIV should breastfeed for at least 12 months and may continue breastfeeding (BF) for up to 24 months or longer” (similar to the general population) while being fully supported for anti-retroviral treatment (ART) adherence” in the absence of adequate conditions for the provision of safe and affordable replacement feeding. Here, breastfeeding (BF) is defined as the provision of breast milk regardless of how breast milk is delivered to an infant/child. Previous WHO guidelines (2004) had recommended BF cessation by human immunodeficiency virus- (HIV−) infected mothers if replacement feeding was deemed “acceptable, feasible, affordable, sustainable, and safe” after at least 6 months of exclusive BF after childbirth. 2 In contrast to these WHO guidelines, the prevention of mother-to-child transmission of HIV (PMTCT) guidelines from 2006 to 2009 in Uganda recommended exclusive BF for the first 6 months, followed by abrupt weaning to reduce the risk of mother-to-child transmission. 3 These changing and conflicting guidelines have contributed to mixed messaging by healthcare providers regarding appropriate BF practices and may be linked to early BF cessation (i.e., stopping BF during the first postpartum year) among mothers living with human immunodeficiency virus (HIV) infection. Although BF has been an accepted method of infant feeding in African culture, little is known about other sources of BF advice outside healthcare settings and how these sources may influence the use of feeding methods in the context of PMTCT.1–3
In low- and middle-income countries (LMICs), 77% of deaths among children 5 years and younger are attributed to suboptimal BF, such as non-exclusive BF during the first 6 months of life, inadequate complementary feeding, and early BF cessation. 4 Early BF cessation has negative effects on childhood health and survival, especially in LMICs where the burden of HIV/acquired immunodeficiency (AIDS) and child malnutrition remains high. 5 Despite these negative consequences, early BF cessation remains prevalent among mothers living with HIV infection in part because of the fear of mother-to-child transmission.6–8
Among mothers living with HIV infection, the risk of early BF cessation tends to be higher among boys and sickly and hospitalized infants.8–10 The prevalence of early BF cessation is also higher among mothers with multiparity, a low educational level, HIV status disclosed to their current partners, and full or part-time employment.7,11–13 Mothers with concerns about breastmilk supply and poor breast health (e.g., breast engorgement, severe mastitis, and painful nipples) also have a higher prevalence of early BF cessation.14–15 These concerning statistics highlight the urgent and critical need to compare the effects of conflicting guidelines on BF practices. This comparison can ultimately inform more coherent healthcare provider messaging and improve childhood health and survival, particularly in LMICs where the burden of HIV/AIDS and child malnutrition remains high.
Conversely, factors that are associated with early BF cessation could serve as motivators for breastmilk expression (BE).16,17 Manual BE or BE with a pump can be a viable strategy to help mothers overcome barriers to direct BF (i.e., feeding an infant directly at the breast) that are linked to early BF cessation.18,19 Despite a growing frequency of mothers who use BE as an integral part of BF-related activities,14,20 research that examines how and to what extent BE impacts BF duration (or early cessation) remains limited. Moreover, existing literature on BE is limited to developed countries, and data on mothers with HIV infection are not available.14,20 Therefore, gaps remain in the understanding of BE prevalence and associated correlates in developing countries in the context of changing WHO guidelines.
To the best of our knowledge, the correlates of these distinct but related BF practices (i.e., early BF cessation and BE) have not been examined in resource-limited settings such as LMICs. Separate analyses are often conducted for each outcome, making it impossible to assess whether correlates or associated risk factors vary by BF practice (i.e., early BF cessation or BE). A better understanding of these risk factor inter-relationships is critical to designing interventions and supporting the promotion of longer breastmilk exposure among at-risk infants.
To address this knowledge gap, our study investigated the pattern of BF practices and identified the correlates (risk factors) of early BF cessation and BE in Uganda, an LMIC with a high prevalence of HIV/AIDS. We used a bivariate logistic regression model to explore these distinct yet interconnected outcomes. In contrast to univariate model results in the literature,14,20 bivariate models can be used to determine how and to what extent BF practices are related and adjust for this dependence to identify correlates of interrelated practices.
Method
Study design, setting, and participants
We used a case-control study design. Specifically, our analytic study sample was selected based on outcome status (i.e., BF practices) independent of participant characteristics.
The study participants were consecutively recruited from three ongoing studies between November 2005 and April 2006 at Mulago Hospital, Kampala, Uganda. Study I (N = 722) was the phase III randomized clinical trial of the standard two-dose nevirapine regimen with the addition of HIV immune globulin or extended infant nevirapine dosing compared with the standard nevirapine regimen alone for the prevention of maternal–infant HIV transmission in Uganda. 21 Study II (N = 1,505) was an HIV Prevention Trials Network study entitled ‘A Phase III Trial to Determine the Efficacy and Safety of an Extended Regimen of Nevirapine in Infants Born to HIV-Infected Women to Prevent Vertical HIV Transmission During Breastfeeding’. 22 Study III (N = 225) included participants who received antenatal and postnatal care at a PMTCT program clinic at Mulago Hospital, Kampala, Uganda. 23 The eligibility criteria across the three studies (Studies I, II, and III) are described elsewhere.21,22 Briefly, all of the participants across the three studies were at least 18 years old at childbirth, had a validated HIV test result, planned to breastfeed during postpartum, and planned to stay in Kampala until their infants were at least 6 months of age.
Data collection: At approximately 12 months after childbirth, all of the eligible study participants from the three parent studies (Studies I, II, and III described above) completed structured interviews during their mother–infant dyad visits at the study clinics. These interviews were conducted in a local Ugandan language (Luganda) by study counselors. Interviews included questions from an adapted WHO questionnaire on infant feeding and sought information on participants’ sociodemographic characteristics based on the local cultural context. Study coordinators reviewed all of the completed questionnaires to ensure completeness in real time before the participants left the clinic. Thereafter, double data entry was employed to ensure accurate data entry on all study-enrolled mother–infant dyads.
Analytic sample: Only the mothers who responded to both the BF cessation and BE-related questions at 12 months postpartum were included in our analyses (Figure 1).
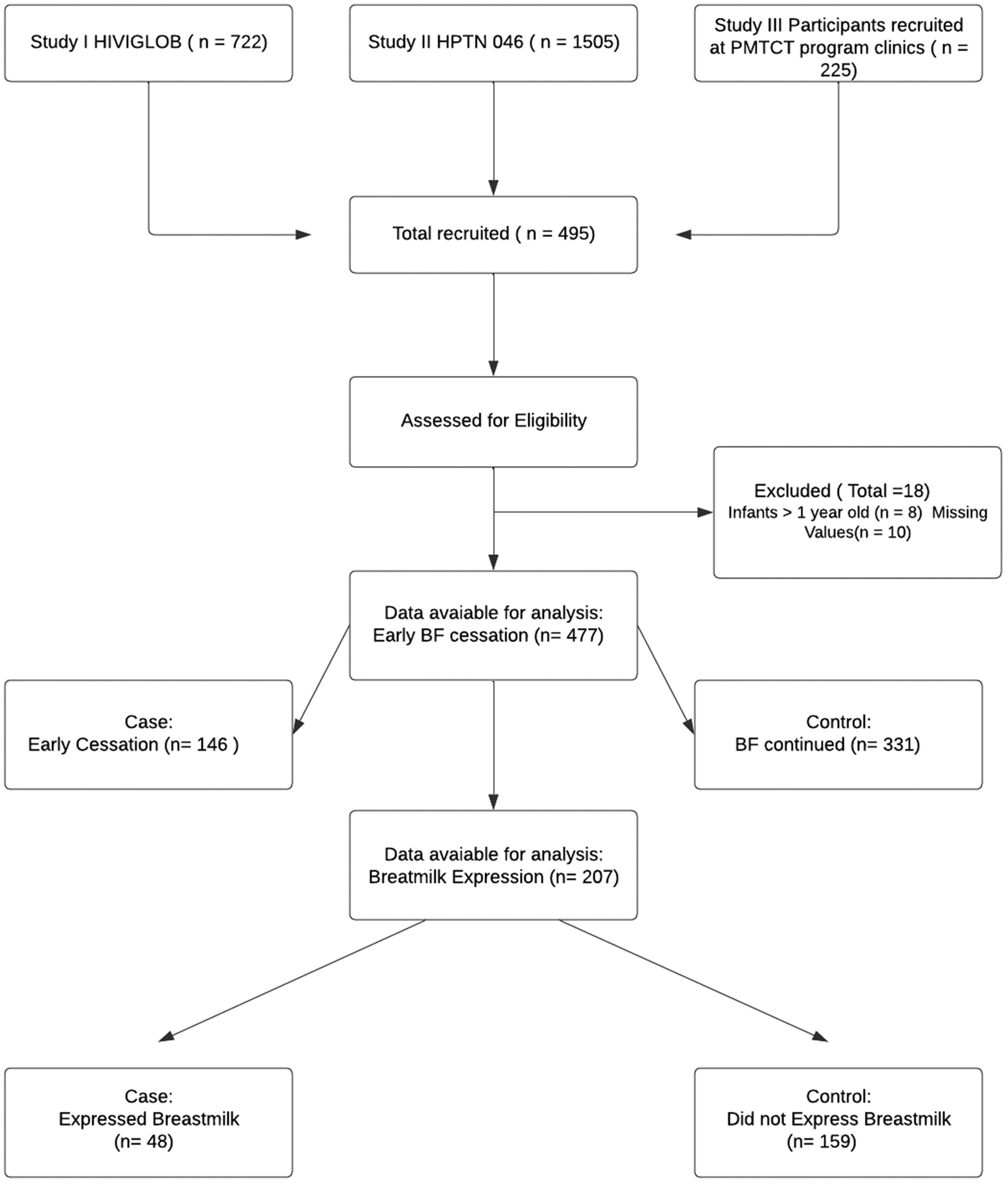
Flowchart showing the case–control study design human immunodeficiency virus (HIV); Study I: a phase III randomized clinical trial of the standard two-dose nevirapine regimen with the addition of HIV immune globulin (HIVIGLOB) or extended infant nevirapine dosing compared with the standard nevirapine regimen alone for the prevention of maternal–infant HIV transmission in Uganda; a phase III trial to determine the efficacy and safety of an extended regimen of nevirapine in infants born to HIV-infected women to prevent vertical HIV transmission during breastfeeding (HPTN 046); and prevention of mother-to-child-transmission of HIV (PMTCT). BF, breastfeeding; BE, breastmilk expression.
Explanatory variables: Sociodemographic characteristics included maternal age (in years), weight, height, education (years of formal education), marital status, occupation, type of housing, number of household members, monthly household income, whether the participant earned income by working outside the home, pregnancy/live birth history, separation from infants, and source of infant feeding advice.
Outcome (case/control) definition: The primary outcomes of interest that were used to define case/control status were early BF cessation and BE. Early BF cessation was defined as stopping BF (directly at the breast or expressed breast milk) before the infant’s first birthday. BE was defined as the act of removing milk from a mother’s breast by hand (hand expression) or using a manual or electric machine called a pump. The expressed milk is then offered to an infant using a bottle or spoon.
The cases were mothers who stopped BF and/or expressed breastmilk during the first 12 postpartum months (Figure 1). The controls were mothers who continued BF 12 months after childbirth and/or did not express breastmilk during the first 12 postpartum months.
Sample size/power considerations: Assuming an equal number of cases and controls (1:1), if 40% of controls had a specific characteristic (e.g., single marital status) to achieve 80% power at a 5% level of significance, a sample size of 214 (107 cases and 107 controls) would be needed to detect a 20% difference (i.e., a 60% prevalence of the same characteristic among cases) with a continuity correction. However, if the prevalence of this characteristic was 20% among cases, a lower sample size would be needed (i.e., 91 cases and 91 controls).
The AIDS Research Committee of the Uganda National Council of Science and Technology and the designated institutional review board at Johns Hopkins University Medical School reviewed and approved the study protocol of our case-control study and all of the study participants provided written consent. All of the participant details were de-identified before analysis. The reporting of this study conforms to the strengthening of the reporting of observational studies in epidemiology guidelines. 24
Statistical analysis
We used descriptive statistics to summarize participant characteristics by BF practice (i.e., early BF cessation and BE). Separate univariate logistic regression models were used to identify independent correlates of early BF cessation and BE (i.e., these outcomes were assumed to be independent). The main effects were reported in the absence of significant (p < 0.05) pairwise statistical interaction terms (tests for effect modification) between the explanatory variables examined. Because early BF cessation and BE are not mutually exclusive events (i.e., they are not polytomous), a multinomial framework was deemed infeasible for statistical analysis.
Bivariate logistic regression was used to account for the dependency between early BF cessation and BE as distinct but related outcomes. 25 Bivariate logistic regression allows the fitting of a single model for both early BF cessation and BE. Each participant has two binary dependent variables, Y1 (BF – y10, y11,) and Y2 (BE – y01, y11), and each takes the value of 0 (control) or 1 (case). We modeled the joint outcome (Y1, Y2) using a marginal probability for each dependent variable and the odds ratio (i.e., the extent to which early BF cessation and BE occurred together), which parameterizes the relationship between the two dependent variables (see Appendix 1 for details). Each of these systematic components is modeled as a function of the investigated explanatory variables. Model parameters were estimated by maximum likelihood using a Newton–Raphson algorithm iterative procedure, and the likelihood ratio test was used to evaluate the significance of parameter estimates.
In this study, we compared the results of the univariate and bivariate logistic regression models to highlight the varying inferences derived from the same study data with (bivariate model) and without (univariate) adjustment for the dependence in BF practices.
All data analyses were conducted using RStudio Version 1.3.1093 (www.r-project.org) and the VGAM package was used for the logistic regression models. 26
Results
Overall, 207 (42%) of the mothers who were recruited met our study eligibility criteria and provided information on their BF practices during the first 12 postpartum months (Figure 1). Most of these women were HIV positive (86%), had vaginal delivery (86%), had at least 8 years of formal education (64%), were married (81%), and were 21 years of age or older (94%). In addition, 42% of the study participants were classified as overweight or obese at 12 months postpartum. In addition to healthcare providers, the most common source of BF advice was a spouse/partner (8%) or a non-family member (8%).
Early breastfeeding cessation
Overall, among the study participants who completed both BF cessation and BE questions (207), 24% stopped BF (cases) and 76% continued BF during the first 12 months (controls). The distribution of sociodemographic factors (e.g., education, income) did not differ between cases and controls (Table 1). The cases were more likely than the controls to have received BF advice from a partner (16% vs 6%) and non-family member (10% vs 2%). The prevalence of HIV infection was higher among the cases than the controls (100% vs 81%).
Distribution of maternal characteristics by BF practice at 12 months postpartum (N = 207).

P values: crude univariate models; report column percentages (i.e., percentage under cases should add up to 100%).
OR, odds ratio; BF, breastfeeding; CI, confidence interval; BMI, body mass index, HIV, human immunodeficiency virus.
Univariate logistic regression showed higher odds of receiving advice from a partner (adjusted odds ratio [aOR] 5.87; 95% confidence interval [CI] 1.39, 29.53) or non-family member (aOR 10.88; 95% CI 2.41, 76.12) among cases than controls. The level of education, marital status, employment, monthly income, body mass index, pattern of delivery, and parity were not associated with early BF cessation (Table 1). Similar results were obtained when we considered a larger sample of respondents, irrespective of whether BE was determined (Supplementary Table 1).
Breastmilk expression
Twenty-three percent (48 out of 207) of mothers in the study sample expressed breastmilk during the first 12 postpartum months. The distribution of sociodemographic factors and sources of BF advice did not differ between mothers who expressed breastmilk (cases: n = 48; 23%) versus those who did not express breastmilk (controls: n = 159; 77%; Table 1). Similarly, univariate logistic models did not reveal significant differences between the characteristics of mothers who expressed breastmilk versus mothers who did not express breastmilk 12 months after childbirth (Table 1).
Joint Outcomes – bivariate model
Bivariate logistic regression showed a strong positive correlation between early BF cessation and BE adjusted for maternal age (OR 2.82, 95% CI 1.39, 5.68) or, stated differently, the odds of early BF cessation given a mother expressed breastmilk. Some maternal characteristics (e.g., age and source of BF advice) were differentially associated with early BF cessation and BE; therefore, these covariate effects were reported for each of the following BF practice configurations: early BF cessation & BE, early BF cessation and no BE, continued BF and BE, and continued BF and no BE (Table 2).
Correlates of BF practices (univariate and bivariate model results).
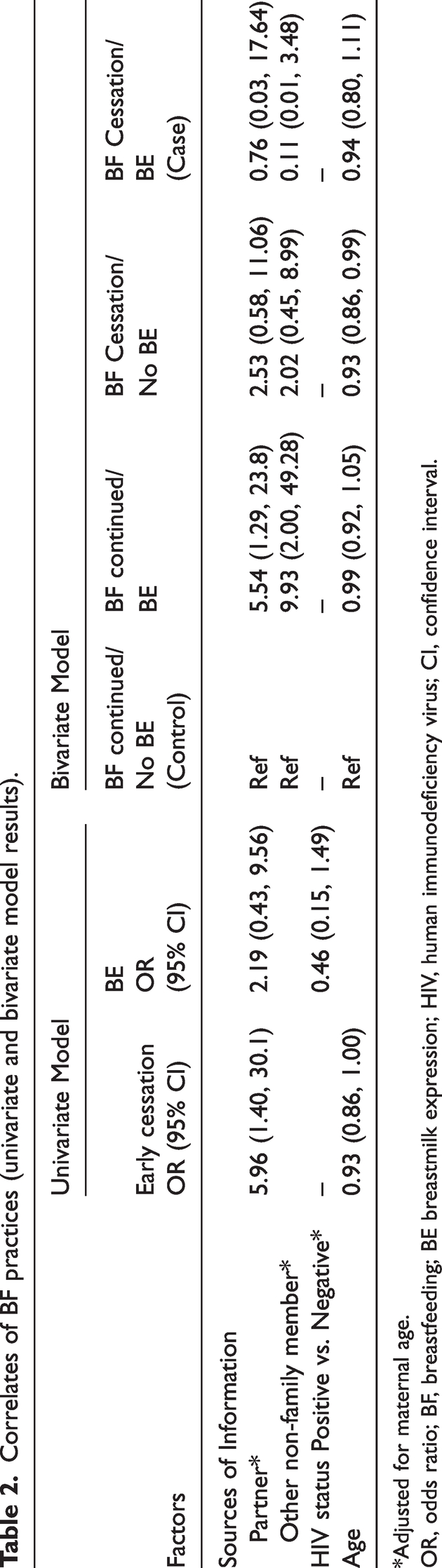
*Adjusted for maternal age.
OR, odds ratio; BF, breastfeeding; BE breastmilk expression; HIV, human immunodeficiency virus; CI, confidence interval.
The association between maternal age and BF practices differed between mothers who received BF advice from partners versus those who did not (BF advice from a partner × age interaction term, p = 0.06). Among mothers who did not receive BF advice from a partner, the odds of older age were 8% lower among mothers who stopped BF and did not express breastmilk than those who continued BF and did not express breastmilk (controls) at 12 months postpartum (aOR 0.92; 95% CI 0.86, 0.99). Mothers who had early BF cessation without BE were more likely to be younger than those who continued BF without BE (controls; Figure 2). Importantly, however, this trend was observed among only mothers with HIV-positive results. None of the mothers who had HIV-negative results had stopped BF at 12 months postpartum. In contrast, among mothers who received BF advice from a partner, this association was not statistically significant. Receipt of advice from non-family members did not modify the association between maternal age and BF practices (BF advice from a non-family member × age interaction term, p = 0.10); however, the odds of receiving BF advice from a non-family member were higher among mothers who reported continued BF with BE than those who reported continued BF without BE (aOR 9.93; 95% CI 2.00, 49.28).

Proportional stacked area graph of breastfeeding practices with change of age among HIV-positive and negative mothers. Mothers who had early BF cessation and no BE were more likely to be younger than those who did not (controls – continued BF without BE). The trend was only observed among HIV-positive mothers. None of the HIV-negative mothers had stopped BF at the time of the postnatal interview. BF, breastfeeding; BE, breastmilk expression.
When the 0.05 interaction threshold was considered, the odds of receiving BF advice from a partner were 5.54 times higher among mothers who continued BF with BE than those who continued BF without BE (aOR 5.54; 95% CI 1.29, 23.80). The odds of older age were 8% lower among mothers who stopped BF and did not express breastmilk than those who continued BF and did not express breastmilk (controls; aOR 0.92; 95% CI 0.86, 0.99).
Discussion
In this study, we used a bivariate logistic regression model to identify the correlates or risk factors of early BF cessation and BE as distinct but related outcomes. Our findings showed that the odds of early BF cessation were higher among mothers who expressed breastmilk. Specifically, early BF cessation and BE were statistically dependent outcomes. The association between maternal age and BF practices was modified by the receipt of BF advice from a partner. Among mothers who did not receive BF advice from a partner, those who stopped BF and expressed breastmilk were more likely to be older than those who continued BF and did not express breastmilk (controls) during the first 12 months postpartum. However, maternal age was not associated with BF practices among mothers who did not receive BF advice from a partner.
Comparisons between our univariate and bivariate model results demonstrate the utility of appropriate adjustment for statistical dependence between BF practices (i.e., early BF cessation and BE) for valid causal inference. Previous studies that ignore the statistical dependence between these BF practices by using univariate statistical analysis models5,6 may have obscured important insights regarding the correlates or predictors of related BF practices.
First, compared with mothers who did not express breastmilk, the higher odds of early BF cessation among mothers who expressed breastmilk suggests BE during the first 12 months may be a good surrogate indicator of mothers who are at risk of early BF cessation. Some research shows that compared to direct BF, BE may be an alternative method for providing breastmilk during periods of maternal–infant separation and can help manage BF difficulties. 27 Therefore, targeting risk factors that are most proximal to BE among mothers who are at risk of early BF cessation could be a viable strategy for increasing the duration of breastmilk exposure, especially among mothers living with HIV infection.28,29 However, the relatively high prevalence of BE in a resource-limited setting (i.e., Uganda) may entail a high risk of maternal–child transmission of HIV in the absence of adequate conditions for the provision of safe and affordable replacement feeding. If true, mothers involved in BE may need to be targeted with additional support to ensure that BE is safer and that the risk of breastmilk contamination is reduced. Currently, BE receives little to no attention as a strategy for breastmilk exposure; however, BE has the potential to increase the duration of BF in a population that is disproportionately affected by poor breast health.
Second, in contrast to previous studies that have shown that younger maternal age is associated with a shorter duration of BF,7,30–34 our study shows that younger maternal age is associated with a shorter duration of BF (i.e., early BF cessation without BE vs continued BF without BE) only among mothers who do not receive BF advice from a partner. Among mothers who received BF advice from a partner, age was not associated with BF practices. These findings underscore the relevance of preventive strategies that target a mother’s partner for inclusion in BF promotion activities to improve BF practices in LMIC settings.7,30–34 Equally important, these findings raise the question of whether maternal age and partner education influence the duration of BF through their impact on BE. To the best of our knowledge, this is the first study to document the moderating effect of BF advice from a partner on the relationship between maternal age and BF practices. This moderating effect could be leveraged to better inform the design and targeting of BE promotion programs that encourage a longer duration of breastmilk exposure for at-risk infants. BF promotion programs that encourage family and/or community support are effective in increasing the rate of exclusive BF during the first 6 months of life.33–36 Targeting such programs to young mothers whose decision-making about BF practices may be influenced by negative partner, family, or societal pressures is warranted.
Third, because of the strong dependence between early BF and BE, separate BF practice-specific correlates were computed, and the differences in the strength and direction of the association between investigated maternal characteristics and BF practices may have important interpretations. For example, the stronger association between the receipt of BF advice from a non-family member and early BF cessation without BE compared with other variations of BF practices (e.g., continued BF without BE) may reflect the varying cultural or societal importance assigned to a specific BF practice. In contrast to the impact of receiving BF advice from a partner, this association was not modified by maternal age. This suggests that unlike the situation in which BF advice is received from a partner, a mother’s receptivity to non-family member advice does not depend on age. Thus, correlates for different BF practices that are identified using multivariate models could lead to important advances in the understanding of why a mother chooses one BF practice over another.
Our analysis has some limitations. First, the data used in this study were collected in 2005 and 2006, more than 10 years before the release of the 2016 WHO guidelines. Consequently, the study is unable to assess the direct impact of these guidelines on BF practices. To better inform resource allocation to improve the duration of breastmilk exposure, future research must examine how and to what extent changes in WHO and national BF guidelines impact BF practices.
Second, a substantial proportion of our study sample included mothers who were HIV-positive (86%); therefore, our findings may not be generalizable to other populations (e.g., mothers without HIV infection). Third, because of our small sample size, our logit models were limited to two responses. Furthermore, the study’s power was too low to detect interaction effects given the sparse data in strata categories. Moreover, because of singularity, the effect of HIV status on BF practices—particularly early BF cessation—could not be examined in our study. In future research, multivariate models that consider more than two responses/outcomes should be considered to better characterize correlates of BF practices (e.g., other descriptors of BF practices such as the introduction of complementary foods and the exclusivity of BF). Finally, the potential for misclassification bias given the reliance on self-report for the classification of BF practices cannot be ruled out. The prevalence of BF at 12 months postpartum may likely have been overestimated among mothers with HIV-negative results compared with those with HIV-positive results.
Importantly, despite these limitations, our study is the first to examine the prevalence of BE and characterize the correlates of BE relative to BF in a resource-limited setting with a high prevalence of HIV/AIDS. 1 Therefore, our results provide a benchmark against which future BE research can be powered for a more comprehensive examination of trends and correlates of BF practices among mothers with HIV infection in resource-limited settings. The fact that all mothers with HIV infection had early BF cessation in our study underscores a substantial challenge to meeting the 2016 WHO guidelines, which recommend continued BF up to 2 years postpartum.
Future studies, such as those that include multi-outcome models, must examine how and to what extent cultural perceptions, misinformation, and inadequate maternal protection policies (e.g., workplace childcare, physical areas for BF or pumping and storing breastmilk, and paid maternity leave policies) may impact various interrelated BF practices.
In conclusion, mothers living with HIV infection continue to have disproportionately high odds of early BF cessation that may contribute to disparities in child health outcomes. Promotion of safe BF practices (e.g., BE) coupled with family and social support could be a viable preventive strategy for attenuating such disparities, especially among young mothers who are at risk of early BF cessation.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231223041 - Supplemental material for Correlates of early breastfeeding cessation and breastmilk expression in Uganda: a case–control study
Supplemental material, sj-pdf-1-imr-10.1177_03000605231223041 for Correlates of early breastfeeding cessation and breastmilk expression in Uganda: a case–control study by Yu Du, Carolyn Onyango-Makumbi, Bhavneet Walia, Maxie Owor, Phillipa Musoke and Arthur H. Owora in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231223041 - Supplemental material for Correlates of early breastfeeding cessation and breastmilk expression in Uganda: a case–control study
Supplemental material, sj-pdf-2-imr-10.1177_03000605231223041 for Correlates of early breastfeeding cessation and breastmilk expression in Uganda: a case–control study by Yu Du, Carolyn Onyango-Makumbi, Bhavneet Walia, Maxie Owor, Phillipa Musoke and Arthur H. Owora in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to express our sincere appreciation to all contributors, including participating mothers, healthcare professionals, research assistants, and relevant institutions, for their invaluable support.
Author contributions
AO and COM contributed to conceptualization, funding acquisition, formulation of research goals and aims, and development of study design; COM contributed to supervision, data curation, and investigation; YD contributed to the evolution of research goals; AO and YD contributed to data analysis and article writing; BW, MO, and PM contributed to article review and editing.
Data availability statement
Data can be provided upon request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Appendix 1
In this study, the probabilities of the two binary response variables (Y1, Y2) are presented below.
BF = Y1
1
0
Total
BE = Y2
1
γ
11
γ
10
γ
2
0
γ
10
γ
00
1–γ2
Total
γ
1
1–γ1
1
Therefore, the joint probability function of outcomes was defined as follows:
The marginal probabilities of Y1 and Y2 are
The marginal probabilities were expressed as follows:
The joint possibility of
According to equations (4) and (5), the possibilities of the rest outcomes were expressed as follows:
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.