
Abstract
Despite progress in human immunodeficiency virus (HIV) prevention, global targets remain unmet, with over 1.3 million new infections annually—driven by adherence challenges, stigma, and daily pill fatigue linked to oral pre-exposure prophylaxis (PrEP). Lenacapavir, a long-acting injectable capsid inhibitor approved by the FDA in June 2025, offers transformative twice-yearly subcutaneous dosing with sustained efficacy and minimal drug interactions. PURPOSE 1 and 2 trials demonstrated near-complete protection across cisgender women, men who have sex with men, transgender individuals, and adolescents, highlighting its potential to overcome barriers to PrEP uptake. Its high acceptability, infrequent dosing, and pharmacologic durability make it ideal for individuals facing stigma, mobility constraints, or limited healthcare access. WHO's endorsement marks a pivotal milestone, but real-world implementation must address cold-chain logistics, cost, provider training, and systemic inequities. Integrating lenacapavir through decentralized delivery models, differentiated care, and inclusive national guidelines will be key to equitable access, decreasing gaps and advancing epidemic control.
Introduction
Human immunodeficiency virus (HIV) remains one of the most pressing global health challenges, disproportionately affecting marginalized communities and impeding progress toward universal health coverage. By the end of 2024, approximately 40.8 million (37.0-45.6 million) people were living with HIV globally, with 65% residing in the World Health Organization (WHO) African Region. That year alone, 1.3 million (1.0-1.7 million) people acquired HIV, and 630 000 (490 000-820 000) died from HIV-related causes; contributing to a cumulative death toll of 44.1 million (37.6-53.4 million) lives lost worldwide. 1
Pre-exposure prophylaxis (PrEP) has been a cornerstone in HIV prevention, demonstrating high efficacy when taken consistently. Currently approved PrEP modalities include daily oral tenofovir disoproxil fumarate/emtricitabine (TDF/FTC), tenofovir alafenamide/emtricitabine (TAF/FTC), long-acting cabotegravir long-acting (CAB-LA) injections, and the dapivirine vaginal ring. Each of these approaches has demonstrated efficacy in clinical trials, but real-world effectiveness varies by population, health-system capacity, and adherence. CAB-LA offers dosing every 2 months but requires clinic-based intramuscular administration, while the dapivirine ring provides a woman-controlled option with modestly lower efficacy than oral or injectable PrEP.2,3 On the other hand, in real-world settings, adherence to daily oral PrEP remains a substantial challenge, driven by factors such as pill burden, HIV-related stigma, and difficulties in sustaining long-term motivation—particularly among young adults, sex workers, and other marginalized populations. 4 In a landmark policy advancement, the WHO has issued updated guidelines recommending twice-yearly administration of injectable lenacapavir as an additional PrEP option for HIV prevention. This guidance is particularly timely, as global HIV prevention efforts have plateaued, with a disproportionate impact on key and priority populations, including sex workers, men who have sex with men (MSM), transgender individuals, people who inject drugs, individuals in custodial settings, and children and adolescents. 3 On June 18, 2025, the U.S. Food and Drug Administration approved Gilead's lenacapavir (Yeztugo®) for PrEP to reduce the risk of sexually acquired HIV, marking the first approval of a twice-yearly injectable PrEP product. 5 As a long-acting subcutaneous formulation, lenacapavir offers a highly effective alternative to daily oral pills and shorter-acting options, with just two doses per year; representing a transformative advancement for individuals who face difficulties with daily adherence, HIV-related stigma, or inconsistent access to healthcare services.5,6
Against this backdrop, lenacapavir represents a promising innovation aligned with the global shift toward long-acting, user-centered HIV prevention strategies. This review article aims to highlight its clinical efficacy and explore its potential to enhance access and adherence across diverse populations, particularly those disproportionately affected by structural and behavioral barriers to traditional oral PrEP modalities.
This article has been prepared as a pharmacological review in line with ICMJE recommendations. Literatures were identified through PubMed, WHO guidelines, and international conference proceedings, prioritizing clinical trial data on lenacapavir, with supplementary references from policy statements and expert commentaries. No new data collection or statistical analysis was performed; the manuscript synthesizes and interprets existing evidence.
Mechanism and Pharmacologic Profile
Lenacapavir functions as a selective, multi-stage inhibitor targeting the HIV-1 capsid. It specifically binds at the junction between two neighboring capsid protein subunits, thereby disrupting critical interactions required across various stages of the HIV replication cycle. These include capsid-mediated nuclear import of preintegration complexes, stabilization of Gag and Gag-Pol polyproteins during virion assembly, and the proper formation of the viral capsid core.7,8 Importantly, lenacapavir remains effective against HIV-1 strains that possess resistance mutations to other antiretroviral drug classes, such as protease inhibitors, nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), integrase strand transfer inhibitors (INSTIs), and maturation inhibitors. 9
Lenacapavir has a prolonged elimination half-life, ranging from 10 to 12 days following oral administration and extending to approximately 8 to 12 weeks after subcutaneous injection. This pharmacokinetic profile underpins its long-acting therapeutic effect. 10 The recommended dosing regimen for lenacapavir PrEP consists of two 300 mg oral tablets taken on Day 1, followed by a second dose of two 300 mg tablets on Day 2 (oral lead-in). The oral lead-in is followed by two subcutaneous injections of 1.5 mL each (total dose 927 mg) administered within a brief time window. Maintenance dosing requires the same pair of subcutaneous injections every 6 months for adults and adolescents weighing at least 35 kg. It is contraindicated in individuals who are HIV-positive. 11
Reported side effects are generally mild and include injection site reactions, nausea, and headache. There is a known risk of resistance development if HIV-1 infection occurs prior to initiation, during the course of treatment, or after discontinuation of lenacapavir. Additionally, since lenacapavir acts as a moderate inhibitor of CYP3A and an inhibitor of P-glycoprotein (P-gp), patients starting therapy with strong or moderate CYP3A inducers may require adjusted doses.6,10
Clinical Evidences
Lenacapavir, given as a twice-yearly subcutaneous injection, is emerging as a breakthrough in HIV prevention—particularly for individuals who struggle with daily pill adherence. Its ultra-long-acting nature and strong protective efficacy have been demonstrated through two major global trials: PURPOSE 1 and PURPOSE 2.
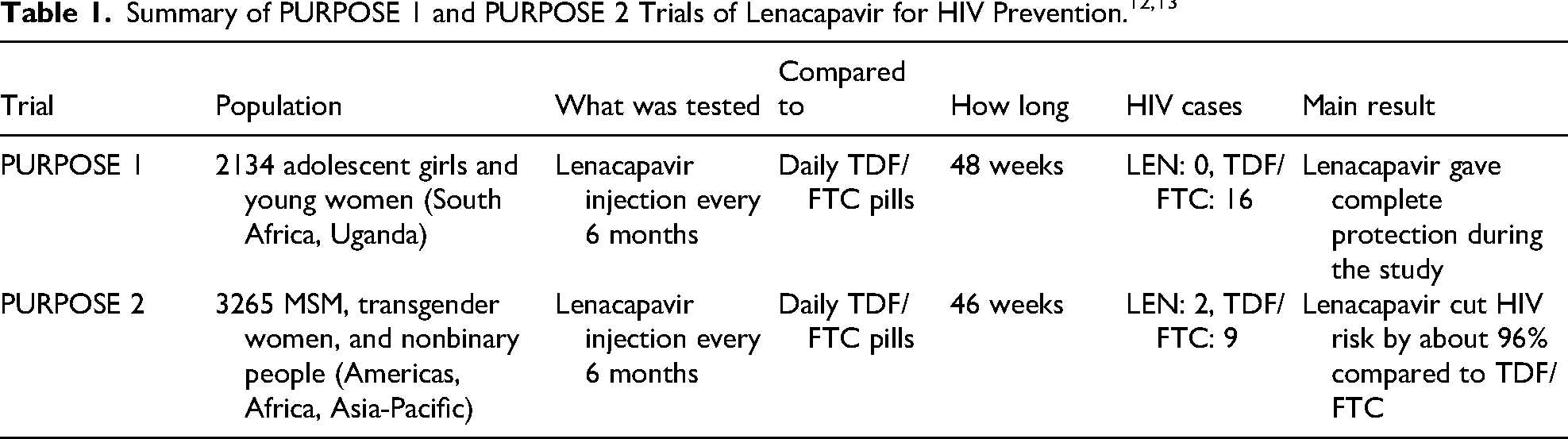
In the PURPOSE 1 trial, a high-risk group of 2134 HIV-negative cisgender adolescent girls and young women from South Africa and Uganda received lenacapavir, while 3204 participants were assigned to daily oral Truvada (TDF/FTC) and followed for a median of 48 weeks. Notably, none of the individuals who received lenacapavir contracted HIV, indicating nearly 100% protection, while 16 new HIV infections were observed in the TDF/FTC arm over the study period. 12
The PURPOSE 2 trial extended this investigation to a broader population, enrolling 3265 participants, including MSM, transgender women, and nonbinary individuals across the Americas, South Africa, and the Asia-Pacific region. Participants were randomized in a 2:1 ratio to receive either twice-yearly lenacapavir injections or daily oral Truvada. In the lenacapavir group, only two new HIV infections occurred—likely due to undiagnosed HIV at baseline or missed follow-up visits—compared to nine infections in the daily oral PrEP group, reflecting a 96% reduction in risk. The median follow-up in PURPOSE 2 was approximately 46 weeks. Two infections in the lenacapavir arm were adjudicated as likely due to either baseline undiagnosed infection or missed follow-ups; nine infections occurred in the daily oral comparator arm, some of which may also reflect adherence gaps or missed dosing. These findings highlight the importance of robust baseline HIV testing and continued adherence support in PrEP programs. 13
Together, these two landmark trials offer compelling clinical evidence of lenacapavir's effectiveness across a variety of populations and settings. The combination of exceptional efficacy, infrequent dosing, and broad demographic success underscores lenacapavir's potential as a next-generation PrEP agent, capable of transforming HIV prevention strategies on a global scale (Table 1).
Public Health Implications
Emerging qualitative and quantitative data from the Phase III PURPOSE 1 and 2 trials reveal a strong preference for twice-yearly injectable PrEP with lenacapavir over daily oral PrEP, with over 75% of participants favoring the injectable option and more than half expressing a strong preference. Reported benefits include a greater sense of protection against HIV and improved confidence in adherence—factors critical for uptake and sustained use. 14
PURPOSE 1, the first HIV prevention trial to demonstrate zero incident infections, signals a potential breakthrough in epidemic control. Lenacapavir's long-acting formulation, requiring just two doses per year, addresses common adherence barriers such as stigma, privacy concerns, and the burden of daily medication. 15 As a newly WHO-recommended PrEP option, alongside daily oral PrEP, injectable cabotegravir, and the dapivirine vaginal ring, lenacapavir broadens the global HIV prevention toolkit. While current access remains limited outside clinical trials, WHO urges countries to begin integrating lenacapavir into national combination prevention programs with concurrent monitoring of real-world uptake, adherence, and impact. 7 Lenacapavir's twice-yearly schedule reduces visit burden and pill fatigue, but adherence remains conditional on clients returning for scheduled semiannual injections and on trust in injectable prevention strategies. Targeted education, appointment reminders, and community-based delivery models will be needed to translate trial efficacy into real-world effectiveness.
UNAIDS echoes this call, advocating for rapid regulatory approval in low- and middle-income countries (LMICs); particularly those with high HIV incidence and for ensuring equitable, affordable access. Emphasis is also placed on prioritizing high-impact prevention strategies and delivering services through simplified, differentiated models that effectively reach underserved populations. 16
Limitations and Implementation Challenges
Implementing twice-yearly injectable PrEP with lenacapavir requires resilient health systems, particularly in low-resource settings, to support storage, delivery, and trained personnel. Provider engagement remains limited by the “purview paradox”—a disconnect where primary care providers assume HIV prevention falls under specialist care, while HIV specialists view it as the responsibility of primary care—resulting in gaps in PrEP delivery. Implicit biases and inconsistent prescribing patterns further threaten equitable access, underscoring the need for standardized, inclusive clinical guidelines. 15 Tailored patient education must address stigma, low awareness, cultural and gender differences, and variable literacy. Additionally, diverse populations face unique psychosocial and structural barriers; successful uptake will depend on inclusive research, support for retention in care, and shared provider-patient decision-making. 17
Cost-related and logistical challenges present significant implementation hurdles. The high price of long-acting injectable PrEP—compounded by cold-chain requirements, patent protections, and laboratory monitoring—limits feasibility in many African settings. Rural health facilities often lack refrigeration, stable electricity, or trained staff, making safe storage and delivery difficult. Moreover, without WHO recommendations, many LMICs are excluded from donor funding and cannot negotiate drug pricing, delaying national guideline development. 18
On the client side, barriers include limited facility access, fear of injections, stigma associated with HIV services, and concerns about reduced autonomy with provider-administered care. Socioeconomic factors such as transportation costs and rigid clinic hours further restrict uptake, especially when long-acting PrEP is not integrated into broader health systems. 1 Without intentional strategies to decentralize service delivery and bring care closer to communities—through community pharmacies, mobile clinics, or lay health workers—the full public health potential of lenacapavir may not be realized.
Conclusion and Future Directions
Lenacapavir represents a transformative advancement in HIV prevention, offering highly effective, twice-yearly protection that addresses key barriers to daily oral PrEP. However, realizing its full public health potential will require strategic and equitable implementation. Future priorities include ensuring affordability through global procurement mechanisms, integrating lenacapavir into national HIV prevention guidelines, and expanding delivery through decentralized, community-based models. Real-world evidence on long-term safety, use in special populations, and programmatic integration will be essential to guide sustainable scale-up. With robust investment, inclusive policy frameworks, and community-centered delivery approaches, lenacapavir could play a pivotal role in accelerating progress toward global HIV prevention targets—bringing us closer to the goal of ending the HIV epidemic.
Footnotes
Abbreviations
Ethics Approval and Informed Consent
Not applicable as this is a review article based on previously published literature and did not directly involve any human subjects, patient data, or animal research.
Consent for Publication
Not applicable.
Author Contributions
SS and UI contributed to the conception, data gathering, literature review, and writing the first draft of the manuscript; TM, NU, and TY played a role in optimizing the grammar, literature review, and English language editing, extensively reviewing the first draft, and substantially contributing to revising it critically for important intellectual content in the final manuscript. All authors accepted the accountability of research work authenticity and agreed to publish the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
Not applicable.