
Abstract
In 2017, Morocco became the first Arab country to incorporate pre-exposure prophylaxis (PrEP) in its HIV-prevention program. Yet no research has been published on PrEP from Morocco. Although female sex workers are one of the target populations of PrEP in Morocco, their enrollment in PrEP is lower than men who have sex with men. In this study, we conducted 38 semi-structured interviews with female sex workers, physicians who prescribe PrEP, policymakers, and community advocates to identify problems associated with access to and use of PrEP. We also investigated preferences for daily oral, vaginal ring, and long-acting injectable PrEP. A reflexive thematic analysis revealed seven themes: PrEP stigma; stigmatization and criminalization of sex work; one size doesn’t fit all; knowledge and misconceptions about PrEP; economic burden; inconvenience of PrEP pills; and preferred PrEP modalities. This paper discusses the implications of the findings for increasing access and use of PrEP in Morocco.
Plain Language Summary
One of the most recent scientific advancements in the history of the HIV pandemic was the introduction of pre-exposure prophylaxis (PrEP). However, the uptake of PrEP in the Arab world is low. In this paper we interviewed female sex workers, physicians who prescribe PrEP, policymakers, and community advocates to identify problems associated with access to and use of PrEP. Several barriers were identified including stigma attached to PrEP, misconceptions about PrEP, and financial burden. Although most female sex workers in our study were interested in using PrEP, the delivery methods of PrEP should be tailored to fit the lifestyle and personal circumstances of potential users.
Introduction
One of the most recent scientific advancements in the 40-year history of the HIV pandemic was the introduction in 2012 of pre-exposure prophylaxis (PrEP), a highly effective medication for HIV prevention. Oral PrEP based on tenofovir disoproxil fumarate emtricitabine has been recommended by the World Health Organization as a component of a comprehensive strategy for HIV prevention. 1 When taken as prescribed, it reduces the risk of HIV infection among people who are at substantial risk. The dapivirine vaginal ring, a PrEP delivery device that is worn for 28 days, is another option recommended for women at substantial risk of risk of HIV infection. In December 2021, the FDA approved a long-awaited PrEP extended-release injectable. 2
As of 2019, 121 countries had adopted the WHO recommendations on oral PrEP to varying degrees. 3 Morocco and Lebanon are the only countries in the Arab world that officially offer PrEP as a part of their HIV-prevention programs. Recent data from UNAIDS 4 show that 360 people in Lebanon and 631 in Morocco received PrEP at least once in 2020. A literature review revealed only one study related to PrEP from Lebanon. 5 The study found that 44.5% of 218 men aged 18 to 29 years who had sex with men were reluctant to take PrEP. Although Morocco was the first Arab country to implement PrEP, in 2017, 6 to date no study has been published on PrEP in Morocco. The present qualitative study sought to identify barriers to access to and uptake of PrEP and preference for oral daily pills, vaginal ring, or long-acting injectable (LAI) PrEP modalities among female sex workers (FSWs), with inputs from three key stakeholders in Morocco.
Research on challenges related to access to, uptake of, and adherence to PrEP has been conducted in many parts of the world, including countries in sub-Saharan Africa,7,8 Europe,9,10 Latin America,11,12 North America, 13 and Asia.14,15 Key factors limiting access, uptake, and PrEP initiation include medication-related factors; personal and interpersonal factors; and community and state-level policies. Examples of challenges are actual or perceived PrEP side effects16,17 or perceived low risk of HIV acquisition, 18 HIV stigma,19,20 limited knowledge of PrEP,17,21 mistrust of the medical establishment, 22 PrEP service delivery, 23 and discriminatory policies such as criminalization of sex work.24–26
Awareness of, preference for, and tolerance of different PrEP modalities vary among people at risk of HIV infection.27–29 In one study, 30 32.1% of Black women in the United States were aware of PrEP, with slightly over half (51.1%) preferring oral PrEP and 26% favoring injectable PrEP. The vaginal ring was the least preferred (6.7%) delivery form of PrEP. A global review of the PrEP vaginal ring found that preference for this device is lower in African studies than in European, Asian, and multi-region studies. 31 FSWs, people who inject drugs (PWIDs),32,33 and sexual minority men, especially inconsistent condom users34,35 preferred LAI PrEP.
HIV and PrEP in Morocco
Morocco is a North African Arab and Muslim country with about 37 million inhabitants. It is part of the Middle East and North Africa region, one of two regions in the world where new HIV cases are on the rise. In Morocco, almost 65% of new infections occurred among key populations and their partners. 4 In 2020, 8727 gay men and other men who have sex with men (MSMs), 19,825 sex workers, and 304 PWIDs in Morocco tested for HIV. 4 HIV prevalence rates among sex workers, MSMs, and PWIDs in 2020 were 1.7%, 4.9%, and 7.1%, respectively. 4 The Association de Lutte contre le Sida (ALCS), in collaboration with the National AIDS Program (NAP), the Global Fund Support Program Morocco (UGFM), and UNAIDS, launched a pilot project in 2017 to test the feasibility of using PrEP among FSWs and MSMs. Since then, PrEP has been offered at ALCS free of charge. As of 2022, 736 people had received PrEP at least once in Morocco. 4
In this paper we examined some obstacles that prevent access to and use of PrEP and preferences for three PrEP delivery methods from the perspectives of FSWs, PrEP prescribers, and stakeholders in the policy and advocacy arenas in Morocco.
As discussed above, determinants of access to, use of, and adherence to PrEP consist of a combination of factors that reside within and outside individuals that constrain their choices. Hence, we adopted the social ecological model as an organizing sensitizing framework for data collection. 36 This model has been used to understand the facilitators and barriers to PrEP uptake which are embedded in multiple levels including individual, interpersonal, social, cultural and policy levels. 37 In this study we utilized this model by collecting data from various PrEP stakeholders.
Methods
Participants and Procedures
We conducted semi-structured interviews with ten FSWs and 28 key stakeholders, including ten physicians who prescribed PrEP, eight policymakers, and ten community advocates. The interview guides were not pre-tested.
All FSWs and nine of the ten community advocates were recruited from ALCS branches located in two major cities in Morocco. The other participants were recruited in seven cities in Morocco. Inclusion criteria for FSWs were (a) being assigned female sex at birth; (b) 18 years of age or older; (c) having had sex with men in the last 6 months in exchange for money or material goods; (d) having resided in Morocco for the last 6 months; (e) being HIV-negative; and (f) consenting to participate in the study. Data were collected between March 15 and May 31, 2021, during the COVID-19 pandemic. The interviews lasted on average 60 minutes and were conducted virtually via Zoom. Participants were interviewed in Arabic and French, and the interviews were translated into English. For all participants, the interview guide focused on their awareness of and experience with PrEP, issues associated with the use of PrEP, and preferences for PrEP delivery methods. FSWs were asked to provide minimal sociodemographic data to protect their anonymity. All interviews were recorded and transcribed by members of the study team. To protect FSWs’ identity, they were assigned numbers followed, when appropriate, by age (e.g., P03-29). Finally, the study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guideline. 38
Ethical Approval and Informed Consent
This study protocol was reviewed and approved by the institution. As per ALCS policy, a written informed consent must be acquired from all FSWs. Thus, we obtained written informed consent from FSWs and verbal consent from other participants prior to enrollment in the study. Illiterate FSWs marked an X or other mark to signify their consent.
Analytic Approach
Interviews were transcribed and analyzed using reflexive thematic analysis (RTA). 39 This approach helps to discover, analyze, and interpret patterns of meaning or themes. 40 The flexibility of this analytical method does not limit its use to a specific theoretical or epistemological framework. It can be used with various research designs and sample sizes. 41 To avoid pursuing consensus of meaning among multiple coders, 42 only the second author conducted the analysis.
RTA was carried out through several nonlinear steps starting with the second author, who read the dataset several times to feel and become familiar with the data. Next, the focus was on generating initial labels, followed by connecting the codes and identifying meaningful themes across the entire dataset. Because RTA is recursive and iterative, 42 we revisited the data and reviewed themes and subthemes generated earlier. Throughout the analysis, we engaged in reflective and insightful interaction with our data.
Results
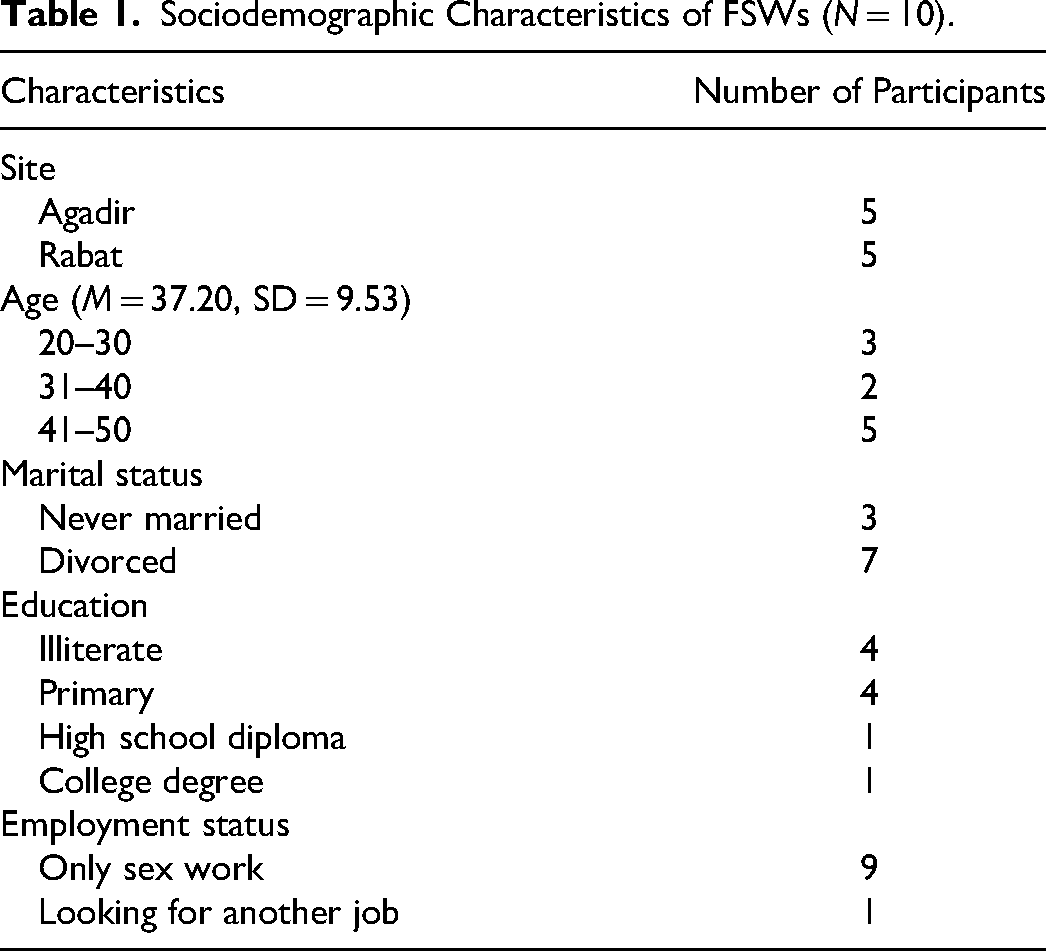
The sociodemographic characteristics of the FSWs are presented in Table 1. Half of the FSWs were under the age of 40 and the other half were 41 and older (M = 37.20, SD = 9.53). Seven were divorced, three were never married, nine were only working as sex workers, and only one had a college degree.
Sociodemographic Characteristics of FSWs (N = 10).
Among the other participants, nine of the community advocates and four of the PrEP prescribers were females. The policymakers consisted of three females and five males. RTA identified seven main distinctive themes: (a) PrEP stigma; (b) stigmatization and criminalization of sex work; (c) one size doesn’t fit all (this theme has two subthemes: a condom is enough, and both PrEP and condoms if possible); (d) knowledge and misconceptions about PrEP; (e) economic burden; (f) inconvenience of PrEP pills; and (g) preferred PrEP modalities.
PrEP-Stigma: “A Girl with HIV”
Most FSWs were reluctant to take PrEP because of its association with HIV for fear of being labeled as HIV positive, as expressed a FSW who said, “PrEP protects you but there is a stigma attached to its use. You might be labeled as a girl living with HIV” (P01-33). Similarly, P02-44 said, “Women are afraid to use it because of stigma associated with it as an HIV-related drug.” One participant was hesitant to try PrEP because, as she put it, “there is the possibility that I could forget it somewhere or someone else might see the box and then I would be stigmatized” (P03-29). Being suspected of having HIV might have serious consequences for FSWs, including physical and sexual violence from clients. As one interviewee put it, “Oral PrEP might not be appropriate because some girls might experience violence if they were discovered using it” (P01-33).
Stigmatization and Criminalization of Sex Work: “Laws Kill”
Punitive and nonprotective laws regarding sex work increase FSWs’ vulnerability to HIV infection, physical and sexual violence, avoidance of HIV care, taking PrEP, and adhering to PrEP protocols.25,43 The criminalization of sex work and its impact on FSWs and their uptake of PrEP was elaborated by a policymaker who said, “Laws that criminalize sexual relations between two adults outside of marriage are in themselves a real barrier to access to protection. Laws kill. They prevent these people from having access to the means of prevention.” A community advocate summed up the status of FSWs in Morocco by saying, “Their work is criminal both legally and religiously. They are rejected by society.”
One Size Doesn’t Fit All
Participants across the four stakeholder groups highlighted the importance of personal and social conditions in PrEP decision-making. While some FSWs argued that condoms are a sufficient method of protection, mainly against unwanted pregnancy, others stated that PrEP is the best and most secure option. Yet, a few FSWs strived to use both condoms and PrEP.
“A Condom is Enough to Protect Me”
Despite the limitation of condoms, some FSWs preferred them over PrEP for various reasons, including the belief that condoms provide enough protection and a dislike of all medications. One participant (P04-28) expressed her strong view of condoms, saying, “I think condoms are enough to protect me.” Another FSW (P04-42) stated, “I use condoms. I always use them with customers, but I don’t use them with my boyfriend.” A young FSW described her reasons for using condoms rather than PrEP in these words: I haven’t tried PrEP. I don’t like medications. I’m still young and I use condoms. I’m not going to continue in this profession my whole life, so I don’t see a reason to take PrEP. I use condoms and that's enough for me. (P06-20)
Some FSWs preferred condoms due to their social circumstances, while others were more concerned about getting pregnant than getting sexually transmitted infections (STIs), including HIV. An FSW with three children told us, “I use birth control and condoms. I am most concerned about getting pregnant” (P07-44). Another interviewee said, “I’ve been protecting myself from pregnancy, but I’m not protecting myself from HIV” (P03-29). The concern about pregnancy rather than STIs among most FSWs was noted by a community advocate who told us, “Another problem is unwanted pregnancies.” They often say, “I would rather have HIV and not get pregnant.” A policymaker echoed prioritizing unwanted pregnancies over avoiding HIV infection and other STIs, stating that condoms are “mainly for unwanted pregnancies rather than HIV.”
Another reason for using condoms only and not PrEP that was mentioned by FSWs and the other participants is cultural attitudes toward medications. In Morocco, as stated by a health care provider, “I take medication, therefore I am sick.” Thus, for some FSWs, the association between medications and illness makes it difficult to persuade them to take PrEP. A community advocate reiterated this cultural assumption: “To take medicine without being sick is not accepted. It doesn’t make sense to many [Moroccans] to take pills every day without being sick.”
Both PrEP and Condoms If Possible: “I Can’t Lose a Client Who Doesn’t Want to Use a Condom”
Inconsistent condom use, clients’ refusal to use condoms, the inability to negotiate condom use with clients, and condom failure were some of the factors reported by some FSWs that motivated them to take or consider taking PrEP. For example, a 44-year-old (P02) reported, “The condom could tear, or the client doesn’t want to use it.” Another stated, “I use condoms, but most of the time the people I have sex with don’t want to use them and then I have to have sex without a condom” (P03-29). Sometimes, as indicated above, FSWs have no choice but to engage in condomless sex because they cannot risk losing clients. A community advocate reported that she often heard FSWs say, “What should I do if I don’t have money to live on? I can’t lose a client who doesn’t want to use a condom.” For these and other reasons a group of FSWs use both condoms and PrEP. One participant who uses both said, I use condoms. I don’t want to have sex without a condom. My health is the most important thing, and I don’t want to get sick. I feel like I’m protecting myself 100% because I take PrEP––I don’t forget it, and I insist on using condoms. (P09-37)
A health care provider confirmed that some FSWs do not have access to condoms, as a 42-year-old (P05) explained: “Most women have sex with multiple clients, and they can’t always use condoms.” For those women, PrEP is better than nothing. Thus, it seems that using condoms and PrEP is a way to minimize the harm that results from FSWs’ own and their clients’ behavior associated with condoms.
Knowledge and Misconceptions of PrEP: “This Drug is Only an Experiment”
Awareness and misconceptions among FSWs and some health care providers about PrEP and its role in HIV prevention were found to be significant barriers to PrEP promotion and uptake. A 44-year-old stated, “I had no idea that there was a drug to protect us against HIV even if we don’t use a condom. I was shocked to learn this” (P02). Several other FSWs expressed similar sentiments.
One of the misconceptions about PrEP is that it is a new experimental drug. As one PrEP prescriber put it, Some went to pharmacies and didn’t find it, and therefore began to say that this drug is only an experiment and that they are trying this drug in our country and that's why it isn’t sold in pharmacies. They have preconceived ideas that it's new and has side effects.
A community advocate complained about some doctors who were unaware of PrEP and unknowingly hindered efforts to promote PrEP use: “I’ve had discussions with doctors who aren't well informed or don't even know about PrEP. This poses a real obstacle to the promotion of PrEP.”
To combat unawareness and misinformation about PrEP, one FSW suggested that peer education was the solution: “In order to convince women and overcome these obstacles, we women of the association must meet other girls and women so we can talk and raise their awareness of this problem” (P02-44). A similar idea was proposed by another FSW: “Each girl tells [about PrEP] and explains it to others, so the information will reach other women” (P03-29). Another FSW participant wanted to move beyond peer-education, saying, “There should be an awareness campaign––a lot of advertising about the drug, promotion in pharmacies for PrEP and for its safety and benefits” (P07).
Economic Burden: “Sometimes I Don’t Have Money for Transportation”
HIV was depicted long ago as a pandemic of poor, marginalized, and disenfranchised communities.
44
One of the most cited barriers to uptake, attrition, and adherence to antiretroviral therapy was the financial burden.
45
A participant stated that FSWs need “financial support for transportation from and to the PrEP clinic, because sometimes, I don’t have money to go there” (P10-33). A community advocate who has been working with FSWs for many years said, Transportation costs [money]. These girls usually can’t even pay the rent, can’t feed their children, and there are those who get pregnant often and then their [financial] condition worsens, and they start going out a lot to earn money from sex work.
Inconvenience of PrEP Pills: “I Don’t Like the Big Pills”
The size of PrEP pills, their side effects, and having to take them every day were some of the concerns raised by participants in this study and in previous studies. One FSW commented “I don’t like the big pills. I took PrEP for 15 days and then stopped” (P10-33). Another participant complained, “It's not good for me; it hurts my stomach. I used it for six months. It hurt me a lot. When I ate something, I vomited” (P05-42). The lifestyles of some FSWs, such as substance use and heavy drinking, prevented uptake of and adherence to PrEP. One FSW admitted that PrEP interfered with her lifestyle: “It didn't suit me because I take other medications, I’m an alcoholic, and I smoke. It only gave me more issues” (P05-42). A community advocate agreed: “There are also situations where drugs and alcohol are involved,” where FSWs consume “lot of alcohol” and are not in a position “to protect themselves.” Some FSWs used strategies to overcome some of the side effects as one participant said: “It was explained to me that this drug would protect me from HIV. I’ve been taking it every night with dinner to avoid stomach upset. Now I’ve been taking it for the past two years without any issues” (P09-37).
Preferred PrEP Modalities: “Vaginal Ring! No, I Can’t”
Most of the participants were supportive of LAI modalities of PrEP, 46 as illustrated by one participant who explained that she preferred “injection of PrEP every two months because the tablets can be forgotten one day. I think the injection is the best and it will be amazing, and I will choose it first” (P02-44). Another FSW (P01-33) who had been using oral PrEP for a while said, “An injection of PrEP every two months is much better.” The bimonthly use of LAI is more convenient than daily pills, as stated by one interviewee: “While the pills can be forgotten one day or when you travel, etc., I prefer to do the injection every two months and forget about it until the next injection time” (P03-29).
However, PrEP pills are much preferred by almost all FSWs over the vaginal PrEP ring, as declared by a participant (P05): “Vaginal ring! No, I can’t.” Another participant expressed her strong objection to the vaginal ring: Having to change the vaginal ring every month, I won’t use it, and I think other girls won’t use it, especially girls who have a lot of sex, I prefer to take pills every day rather than putting anything into our vagina. (P09-37)
A health care provider agreed with the FSWs, saying, “Women don’t accept putting anything in their body, so it's a little difficult [to persuade them to use the ring], but the choice must be left to women.” A community advocate thought it might be difficult to use the PrEP vaginal ring in the case of “FSWs who have a lot of sex, and also you have to make sure that it stays in place and doesn’t move.”
Discussion
To our knowledge, this is the first study from the Arab world that explored challenges to PrEP use and preferences for different PrEP modalities among FSWs. Several major challenges to using PrEP were identified at the personal, interpersonal, social, and structural levels.
The burden of HIV infection among FSWs in low- and middle-income countries is very high, with more than 13 times increased odds of getting infected with HIV compared with women in higher-income countries. 43 PrEP is one of the most effective and safest methods for reducing HIV transmission among people at risk of infection. Nevertheless, access to and use of PrEP are thwarted by interconnected factors that range from attributes of PrEP to state-level policies such as criminalization of sex work.
In this study, we highlighted some obstacles that hinder FSWs’ access to and interest in PrEP. Stigma attached to PrEP use was one of them. Because of the association between HIV and PrEP, FSWs feared that people, including their clients, would confuse PrEP with antiretroviral treatment, which might lead to them being misidentified as HIV-positive. As supported by previous studies,15,47 fear of PrEP stigma may discourage adoption of adherence to, and continuation of PrEP. Hence, PrEP stigma is a serious issue and stigma reduction strategies are needed to prepare Morocco for potential nationwide implementation of PrEP. One of the approaches we favor to reduce PrEP stigma is to present PrEP as a lifestyle choice driven by personal agency. 47
Stigma and punitive laws against sex work are structural drivers that have tremendous negative consequences for FSWs, including increasing their vulnerability to HIV infection, ill health, exploitation, and abuse and hindering their interest in and use of PrEP. It is important to reduce stigma and remove punitive and nonprotective laws against sex work in Morocco to boost access to PrEP among FSWs.
Another theme we identified was related to condoms and PrEP use. FSWs who chose to use only condoms provided several justifications, including forgetting to take the pills, their dislike of pills, and that their engagement in sex work was not permanent. These barriers have also been reported in other studies in various parts of the world.48,49 Another interesting barrier reported by the participants was a cultural belief that people take drugs only if they are sick. There is clearly a need to educate FSWs that medication is also taken as a preventive measure. Another reason that some FSWs believe condoms are enough is that they are more concerned about pregnancy than HIV infection. Pregnancy is indeed a valid concern, especially since the incidence of unwanted pregnancies among FSWs is high in low- and middle-income countries. 50 FSWs know that male condoms are often not under their control, so they need to be encouraged to use both PrEP and condoms until a pill is developed that prevents both pregnancy and HIV.
Lack of awareness and misconceptions about PrEP were common among some FSWs and health care providers. One serious misconception is the belief that PrEP is an experimental drug, which might stem from mistrust of the medical establishment.51,52 A similar misconception was reported in a study in which one participant told the researchers, “We’re all an experiment. We’re like guinea pigs, you know? You don’t know for real if it's gonna be effective. I mean they say it is, but who's to say that it really will be?” 51 Educating FSWs and especially health care providers about the safety and effectiveness of PrEP is important to increase PrEP use and to prevent discontinuation of the drug. It is important that the information given to FSWs be simple and in plain language so it can be easily understood because, as we noted above, most of the FSWs had a low level of education.
Although PrEP is offered free of charge in Morocco in ALCS's PrEP clinics, there is an economic burden associated with transportation to the designated PrEP locations. Most of the FSWs in our study were living in poverty and could not afford the cost of transportation to collect PrEP and sometimes condoms. Hence, it is necessary to develop a financial assistance program to help with transportation expenses to locations that prescribe and dispense PrEP.
In accordance with findings from other studies,23,53 participants in this study talked about some of the inconveniences associated with PrEP, such as the size of the pills, having to take them every day, and being on medications. With respect to the known side effects of PrEP, although some participants developed strategies to reduce them, they expressed a perception of PrEP as both a preventive measure and a poison. 54 Another challenge voiced by some participants was the lifestyle of FSWs, including heavy drinking and drug use.
Some of these inconveniences may explain the preference that most FSWs indicated for LAI PrEP. Whereas others vacillated between oral and LAI PrEP. Concerning the vaginal ring, however, there was no doubt that it was the least preferred delivery method. PrEP literature shows that there is no consensus regarding the preferred PrEP modality,27,31 as preference for one type over another depends heavily on personal preferences and lifestyles. For example, preference for LAI PrEP is driven by some of its positive features, including less interference with daily activities, not needing permission from sex partners, and a reduced burden for both patients and providers.29,34,51 Our data suggest that LAI PrEP may be best for FSWs who are at higher risk of HIV infection due to factors such as having multiple partners, not using condoms, or using them inconsistently, having no interest in or trouble using oral PrEP, and heavy alcohol or drug use. The next step toward the prevention of HIV in Morocco might incorporate LAI PrEP.
Notwithstanding the significant contributions of the current study, it has certain limitations. First, FSWs were drawn from one AIDS association (ALCS) in two cities in Morocco, which limits our ability to claim that similar patterns of challenges and preferences hold true in other parts of Morocco. However, the literature reviewed above suggests that the patterns we identified might reflect the experience of most FSWs in Morocco. Since PrEP has become a foundational pillar of HIV prevention, more work on other at-risk groups in Morocco, including MSM and PWIDs, is important.
The findings of this study call for multifaceted approaches to HIV prevention that take into consideration the determinants of access to and use of PrEP at all levels. Most FSWs are interested in PrEP and indicated their preferred delivery methods. To increase use of and adherence to PrEP, delivery methods should be tailored to fit the lifestyle and personal circumstances of potential users.
Conclusions
This pioneer work provides important insights into acceptability and preferences for different PrEP modalities among FSWs, with significant contributions from PrEP prescribers, policymakers, and community advocates in Morocco. Although some of the FSWs realized the benefits of PrEP, several micro, meso, and macro variables influenced their decision to initiate and continue use of PrEP.
Supplemental Material
sj-docx-1-jia-10.1177_23259582241266691 - Supplemental material for Barriers to Oral PrEP: A Qualitative Study of Female Sex Workers, PrEP Prescribers, Policymakers, and Community Advocates in Morocco
Supplemental material, sj-docx-1-jia-10.1177_23259582241266691 for Barriers to Oral PrEP: A Qualitative Study of Female Sex Workers, PrEP Prescribers, Policymakers, and Community Advocates in Morocco by Amal Ben Moussa, Abdallah M Badahdah, Khadija Hidous, Rime Barakad, Fodié Diallo, Mariam Traoré, Niloufer Khodabocus, Annette Ebsen Treebhoobun, Rosemary Delabre, Daniela Rojas Castro, Lahoucine Ouarsas and Mehdi Karkouri in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582241266691 - Supplemental material for Barriers to Oral PrEP: A Qualitative Study of Female Sex Workers, PrEP Prescribers, Policymakers, and Community Advocates in Morocco
Supplemental material, sj-docx-2-jia-10.1177_23259582241266691 for Barriers to Oral PrEP: A Qualitative Study of Female Sex Workers, PrEP Prescribers, Policymakers, and Community Advocates in Morocco by Amal Ben Moussa, Abdallah M Badahdah, Khadija Hidous, Rime Barakad, Fodié Diallo, Mariam Traoré, Niloufer Khodabocus, Annette Ebsen Treebhoobun, Rosemary Delabre, Daniela Rojas Castro, Lahoucine Ouarsas and Mehdi Karkouri in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Author Contributions
AB led the research and contributed to drafting the paper, AMB led the data analysis and writing of the paper, KH contributed to the interpretation of the data, RB provided critical feedback, FD provided critical feedback, MT provided critical feedback, NK provided critical feedback, AT provided critical feedback, RD provided critical feedback, DC provided critical feedback, and LO provided critical feedback and helped shape the research, analysis, and manuscript. MK supervised the research and successive drafts of the paper.
Availability of Data and Material
Participants in this study did not consent for their data to be shared publicly.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Standards
All participants consented to participate in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Agence Française d’Expertise Technique Internationale (grant number SUBVENTION N°20-SB1361).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.