
Abstract
Background
This study examines chemsex patterns among gay, bisexual, and other men who have sex with men (GBMSM) and their link to depression using a longitudinal approach. Recognizing and addressing chemsex is crucial for human immunodeficiency virus (HIV) care providers, as it supports harm reduction and effective HIV prevention and treatment for GBMSM.
Methods
From 2017 to 2021, GBMSM at two sexual health clinics completed follow-up questionnaires. We identified chemsex trajectories using group-based modeling and assessed their association with depressive symptoms over two years using multivariable logistic models.
Results
Among 256 GBMSM, three chemsex patterns were found: “never or rarely engaged” (87.4%), “consistently engaged” (8.8%), and “high, decreasing and reinitiated” (3.8%). There were no significant differences in depressive symptoms between the “never or rarely engaged” group and the other patterns.
Conclusions
The study reveals diverse chemsex behaviors but does not provide clear evidence linking these patterns to differences in depressive symptoms among GBMSM.
Plain Language Summary
Background: Chemsex refers to the use of drugs to enhance sexual experiences among gay, bisexual men, and other men who have sex with men (GBMSM). Research has suggested a link between chemsex and depression, but findings have been mixed, and most studies have looked at chemsex and depression at only one point in time. This study aims to track changes in chemsex behavior over time and see how these changes relate to depression. Methods: We followed GBMSM who visited two sexual health clinics from 2017 to 2021. Participants completed questionnaires at least twice. Depression was measured using the Patient Health Questionnaire-9, where a score of 10 or more indicates moderate to severe depression. We used statistical methods to identify different patterns of chemsex behavior and to examine how these patterns relate to depressive symptoms over two years. Results: Among the 256 participants, we found three patterns of chemsex behavior: “never or rarely use” (87.40%), “consistently use” (8.78%), and “high, decreasing, and reinitiated” (3.82%). We found that the likelihood of having depressive symptoms was not significantly different between those who never or rarely used drugs and those with other patterns of use. Specifically, the odds of depressive symptoms for those who consistently used drugs or had high, decreasing, and reinitiated use were not significantly higher compared to those who never or rarely used drugs. Conclusions: Our study shows that chemsex behaviors vary among GBMSM, but the evidence is not strong enough to conclude that different patterns of chemsex are linked to varying levels of depression. This adds to the complex and mixed findings in existing research on chemsex and depression among GBMSM
Keywords
Introduction
Chemsex is a specific form of sexualized drug use, that involves substances like methamphetamine, γ-hydroxybutyrate/γ-butyrolactone (GHB/GBL), and mephedrone, primarily reported among GBMSM community. 1 The prevalence of chemsex among GBMSM ranges widely from 3% to 41% in Asian and European countries.2–4 This emerging practice is shaped by social constructs and contextual differences, impacting its prevalence and understanding. Addressing chemsex is not only relevant to reducing its associated harms but also integral to effective human immunodeficiency virus (HIV) prevention and care. A 2022 review highlights the complex interplay between chemsex, HIV prevention and treatment, and harm reduction, emphasizing the need for tailored, community-based interventions for GBMSM. 5 The relationship between HIV and chemsex highlights the need for HIV care providers and physicians to recognize chemsex as a critical issue in the health of gay, bisexual men, and other men who have sex with men. By incorporating awareness of chemsex into their practices, healthcare providers can play a crucial role in reducing risks and improving overall health outcomes within this population.
In recent years, some longitudinal studies have observed an increase in chemsex engagement among GBMSM,6,7 although the nature of sampling in specific clinical contexts and predominantly in Europe complicates our ability to assess changes in this practice more broadly. Regardless though, shifting patterns of drug use have prompted public health concerns and highlighted the need for better understanding of chemsex behaviors, and indicate more tailored harm reduction approaches in local settings to minimize the chemsex-related harms when they occur. 8
Given the complex health risks associated with chemsex, understanding its relationship to mental health, particularly depression, is crucial for improving HIV/AIDS care outcomes. Co-occurring psychosocial and structural conditions, such as substance use, mental health problems, and HIV, interact or worsen health outcomes. 9 Depression, which has been linked to chemsex, can negatively impact medication adherence, retention in care, and overall health outcomes for people living with HIV (PLWH). 10 Integrated care models that address HIV prevention and treatment, substance use, and mental health together are gaining increasing attention globally as a more effective strategy for improving health outcomes and reducing barriers to care.11,12 A increasing amount of research has shown links between chemsex and negative psychosocial consequences—especially depression. 13 The evidence is provided primarily by cross-sectional studies; however, longitudinal data remain scarce. Most cross-sectional studies on chemsex and depression have revealed a positive association14–16; some studies have suggested no association after controlling for confounding factors.17–19
Several mechanisms have been proposed to explain the association between chemsex and depression. One is syndemic theory, which describes synergic interactions between several physical and sociological conditions, resulting in a greater disease burden. 20 Chemsex and mental health problems, as parts of the syndemic, potentiate each other.21,22 In addition, both chemsex and depression can be associated with loneliness, social isolation, and the stress originating from stigma, discrimination, and internalized homophobia. 14
Research from numerous countries has highlighted how drugs can be used during sex by GBMSM in ways that enhance or facilitate sexual pleasure and pursuit of such is commonly reported as a primary motivation for engaging in chemsex.23,24 However, for some, their relationship with drugs can be more complex and their reasons for engaging in chemsex can involve an attempt to overcome more challenging personal or social issues. Indeed, some research has indicated that chemsex can be used as a strategy to cope with stresses and increase social connections. 25 It is, however, difficult to identify the temporal sequence regarding the association between chemsex practice and depression. Depression is a long-term and dynamic physical condition, and the severity and chemsex behaviors can change over time26,27—both of which highlight the importance of longitudinal studies when observing the association between chemsex and depression.
Thus far, two published longitudinal studies have examined the association between chemsex and depression and have additionally categorized chemsex patterns. One study including 622 HIV-negative GBMSM attending sexual health clinics in the UK categorized the frequency of chemsex engagement at baseline into no use, once, weekly and monthly. The result of this study showed a higher prevalence of clinically significant depressive symptoms among chemsex practitioners over a 3-year follow-up period compared to those who did not engage in chemsex. The other longitudinal study used data from the Multicenter AIDS Cohort Study (MACS) in the United States, which followed 2457 GBMSM for over four years. That study identified five distinct patterns of stimulant drug use—no use, very low, increasing, decreasing, or consistently frequent use of stimulants—without specifically linking this use to sexual activity or chemsex contexts. Individuals not using stimulants had lower levels of depressive symptoms than those who did use stimulants. 28 Though the importance of a longitudinal approach and categorization of chemsex behaviors has been emphasized, there were some limitations of these studies. They either classified chemsex behavior based only on baseline data or did not assess the longitudinal association of different levels of chemsex engagement and depression.
In order to address the evident gaps in the research, the present study aimed to (1) identify distinct chemsex trajectories using data collected from multiple time points, and (2) assess the association of depressive symptoms with chemsex trajectories over time among GBMSM attending sexual health clinics in Taiwan.
Methods
Study Design, Setting, and Participants
We used data from an ongoing, observational, prospective cohort of GBMSM from two hospital-based sexual health clinics between November 2017 and December 2021: the Integrated Health Center of Healing, Empowerment, Recovery of Chemsex (HERO) in Kaohsiung City, and the Sexual Health Integrated Polyclinic (SHIP) in Taipei City. These two sites provided integrated services including STI screening and treatment, preexposure prophylaxis and post-exposure prophylaxis consultation, and chemsex evaluation and consultation. HERO also provides mental health treatment and chemsex recovery groups. 29
All clients attending the clinics for healthcare received detailed information about the study and were invited to complete a baseline questionnaire if they agreed to participate and provided written consent. Follow-up questionnaires were filled out at subsequent visits. Questionnaire items used in this study are provided in Supplemental File 1. The study participants were eligible if they met the following criteria: (1) 20 years old or above at the time of enrollment, (2) assigned male at birth, (3) had sex with men, and (4) had completed the baseline and at least one wave of follow-up questionnaires during the follow-up period. Participants were excluded if they reported having sex with females only, had missing baseline information on age or gender, or did not provide at least two waves of chemsex or mental health measurements. To determine the required sample size, we aimed for a 95% confidence level with a margin of error of ±5%. Based on a systematic review estimating the global prevalence of depression among MSM, 30 we adopted a prevalence rate of 23% when using the Patient Health Questionnaire (PHQ) as the measurement tool. Applying these parameters, the calculated minimum sample size required was 273 participants. At the time of the initial IRB application, the legal age of adulthood in Taiwan was 20 years; therefore, eligibility was restricted to participants aged 20 years or older.
A longitudinal dataset was built based on data from the baseline and follow-up questionnaires of each participant, with a 2-year follow-up period. All participants provided written informed consent prior to joining the study.
Measurements
Chemsex
In relation to the extent of chemsex, participants answered the question “What proportion of your sex life involves MDMA, ketamine, ice (methamphetamine), GHB/GBL or meow meow (mephedrone)?” with a visual analog scale (VAS) ranging from 0 to 100 at the baseline questionnaire. Within follow-up questionnaires, the time frame of the behavior was specified to the past month on the same VAS scale. The self-reported VAS scores at baseline and follow-up questionnaires were collected to determine the trajectory of chemsex behavior. These scores were used as reported, representing the directly stated proportion of chemsex involvement without transformation or adjustment.
Depressive Symptoms
The severity of depressive symptoms was measured using the Patient Health Questionnaire-9 (PHQ-9). 31 Each item of the PHQ-9 was scored on a four-point Likert scale ranging from 0 (not at all) to 3 (nearly every day), and all items of each scale were summed to provide a total score. The unanswered items were substituted with average values of the other items if the missed data were less than 20% within a questionnaire. The Cronbach's alpha for PHQ-9 was 0.94 in our sample. A total PHQ-9 score of 10 or more was identified as moderate to severe depressive symptoms, which was used as a binary variable at baseline and follow-up questionnaires to assess the changes in the severity of depressive symptoms. At the conclusion of the questionnaire, participants were provided with a table explaining the PHQ-9 score thresholds for depressive symptoms along with recommendations for seeking support. Additionally, information on available mental health services was provided, ensuring that participants with moderate or severe depressive symptoms had clear guidance on accessing appropriate care.
Sociodemographic Characteristics
Baseline sociodemographic characteristics included age (categorized into 20-34, 35 + years old), educational level (university degree or below, graduate degree or higher), employment status (full-time, non-full time), monthly income (<30 000 New Taiwan Dollar [NTD], 30 000 NTD or more, based on questionnaire options: <15 000, 15 001-30 000, 30 001-45 000, >45 000 NTD). This cut point aligns with Taiwan's 2021 minimum wage (25 250 NTD, approximately 840 USD, at an exchange rate of 1 USD ≈ 30 NTD). Relationship status (in a relationship, not in a relationship) and self-reported HIV status (PLWH, not PLWH) were also included.
Substance use and Sexual Behaviors
Participants reported their drug use in the past year at the baseline questionnaire including ketamine, alcohol, marijuana, mephedrone, rush poppers, ecstasy, prescription sedative-hypnotics, amphetamine/methamphetamine, GHB/GBL, sildenafil (Viagra®), tadalafil (Cialis®), or other erectile dysfunction medications, cocaine, lysergic acid diethylamide, psilocybin mushroom or other hallucinogens, drug-laced coffee-packets (multiple unknown substances mixed with instant coffee powder). Polydrug was defined as the use of more than one kind of substance from the list above (binary variable).
Two sexual behavior variables were constructed: Multiple sex partners and receptive condomless anal intercourse in the past six months. First, participants were asked about the number of anal sex partners in the previous six months in the baseline questionnaire, with the following response options: 0, 1, 2–5, 6–10, and more than 10. Participants with two or more anal sex partners were classified as having multiple sex partners (binary variable). Second, participants reported the frequency of receptive condomless anal intercourse (CLAI) with the following options: once, twice, three to four times, five to nine times, more than ten times, and never. The answers were dichotomized into once or less and twice or more.
Statistical Analysis
We applied group-based trajectory modeling (GBTM) to identify the trajectories of chemsex over the follow-up period. GBTM is a semiparametric approach for longitudinal data used to identify subgroups of individuals following a similar path. 32 For the purpose of trajectory analysis, one follow-up wave was set as three months, with a maximum of seven waves in two years. We chose three months as the cutoff to minimize missing data, as many people undergo HIV testing or return for treatment every three months. If there were more than one measurement within one wave, the measurement closest to the center of the wave was adopted. The maximum of seven waves over two years (24 months) was chosen to allow for 3-month intervals, with the baseline included, resulting in 8 total waves.
To determine the best model fit of trajectory, a series of models were created, and the model fit was tested by gradually increasing the number of trajectory groups and the order of polynomial growth factors (intercept, linear, quadratic, and cubic). Determinants of model fit were as follows: (1) smaller values of Bayesian information criteria (BIC) and Akaike information criterion (AIC), (2) average posterior probabilities of group membership greater than 70%, and (3) a priori knowledge. 33
The differences in baseline characteristics between participants with moderate to severe depressive symptoms and those without were tested by Pearson's χ2 or Fischer's exact test for categorical variables, and Student's t-test or Wilcoxon signed-rank for continuous variables to determine the risk factors of depression. Significant covariates were included in the subsequent multivariable analysis.
We further examined whether chemsex trajectories were associated with moderate to severe depressive symptoms over time using a mixed effects logistic model. The logistic mixed model to be fitted can be written as
All the above statistical analyses were conducted using Stata/SE version 15.1 (College Station, TX, USA). We considered a two-sided p-value less than .05 as statistically significant. When nonsignificant results were observed in mixed effect logistic regression, Bayes factors (BFs) were used to distinguish inconclusive data. BFs were calculated with an online calculator: http://bayesfactor.info/, which was developed using R code with open source on Github. Parameters needed for the calculator include odds ratio, upper 95% CI of odds ratio, hypothesized odds ratio and a two-tailed test. The effect size of the alternative hypothesis was set as 1.47 based on previous research. 26 A BF value between 0.34 and 3.0 indicates inconclusive evidence of an effect, and a value of less than 0.33 means no evidence of an effect. 34 The reporting of this study conforms to the Strengthening the reporting of observational studies in epidemiology (STROBE) statement for cohort studies 35 (Supplemental File 2).
Results
Study Participants and Sociodemographics
Between November 2017 and December 2021, 2573 clients consented to and completed at least one questionnaire. After excluding those who provided neither baseline questionnaires (N = 268) nor more than one wave of follow-up questionnaires (N = 1895), 410 participants were recruited and assessed for eligibility. Finally, a total of 262 participants were included for analyses, contributing 675.40 person-years of follow-up (see Figure 1).

Flow diagram of study participants.
Table 1 shows the sociodemographics and sexual behaviors at baseline of enrolled participants. Among these, the median age was 30; the majority were in full-time employment; one in six were living with HIV. Over half reported having multiple sex partners, and more than a quarter claimed more than two times of receptive CLAI. Over a fifth of the sample reported chemsex engagement. Polydrug use was reported in 21.76% of the participants. Among the sexualized drugs, methamphetamine was the most commonly reported (18.32%), followed by GHB/GBL (9.54%), ecstasy (7.25%), and ketamine (3.44%).
Baseline Characteristics of Enrolled Participants (N = 262).

CLAI, condomless anal intercourse; HERO, Healing, Empowerment, Recovery of Chemsex; NTD, New Taiwan Dollar; PLWH, people living with human immunodeficiency virus; SHIP, Sexual Health Integrated Polyclinic.
The baseline prevalence of moderate to severe depressive symptoms was 17.18% (45/262). Participants who reported moderate to severe depressive symptoms at baseline were more likely to be part-time employees or unemployed (55.56% vs 23.50%; p < .001), be living with diagnosed HIV (28.89% vs 12.90%; p = .007), and reported ever engagement in chemsex (33.33% vs 20.28%; p = .033), compared to those who did not have such symptoms or did not answer the questions.
Different Chemsex Trajectories Over the two-Year Follow-up
Using the dataset of participants’ self-reported engagement in chemsex (specifically the proportion of their sex involving drugs) across the two-year follow-up period, we identified three distinct chemsex trajectory groups: “never or rarely engaged,” “consistently engaged,” and “high, decreasing and reinitiated” (Figure 2). The final model with two linear terms and one quadratic term was selected because of the best model fit overall (BIC = −319.48; AIC = −296.72, as well as average posterior probabilities of group membership exceeding 80%). This model also provided clear and interpretable trajectories. The model selection process is detailed in Supplemental File 3.

Trajectories of chemsex over 2-year of follow-up (N = 262).
The “never or rarely engaged” group accounted for most of the sample (n = 229; 87.40%) reporting no chemsex engagement at baseline and throughout the follow-up period. Approximately one in 11 clients (n = 23; 8.78%) were classified as the “consistently engaged” group characterized by consistent chemsex engagement reported during the study period. The “high, decreasing and reinitiated” group comprised a small portion of the sample (n = 10; 3.82%). Of note, this trajectory group represented those who reported the highest proportion of chemsex at the initial visit and then declined after three months, but reinitiated by the end of the follow-up period.
The Association Between Moderate to Severe Depressive Symptoms and Chemsex Trajectories
The association between moderate to severe depressive symptoms and chemsex trajectories was analyzed using a multivariable mixed effects logistic model in Table 2.
Mixed Effects Logistic Regression of Association of Chemsex with Moderate to Severe Depressive Symptoms (N = 262).
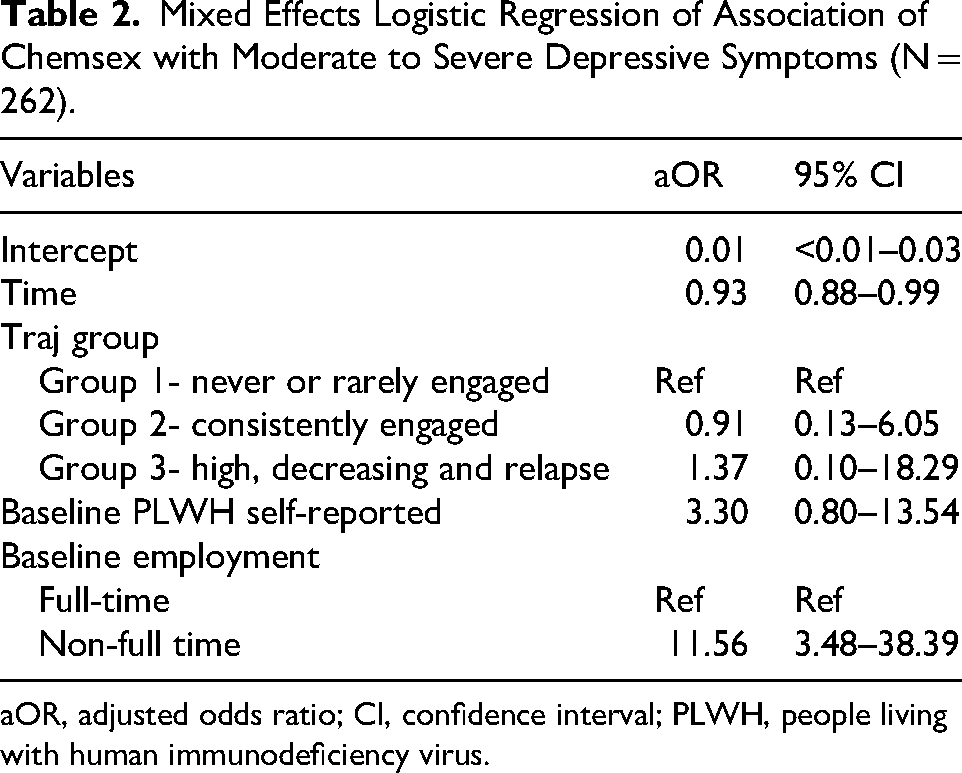
aOR, adjusted odds ratio; CI, confidence interval; PLWH, people living with human immunodeficiency virus.
The odds of moderate to severe depressive symptoms comparing the three chemsex trajectory groups were not significantly different. Specifically, the comparison between the consistently engaged group and the never or rarely engaged group yielded an aOR of 0.91 (95% CIs [0.13, 6.05]), while the comparison between the high, decreasing, and reinitiated group and the never or rarely engaged group yielded an aOR of 1.37 (95% CIs [0.10, 18.29]). These findings were further deemed inconclusive by BFs (0.93 and 0.96, respectively). Those who were not in full-time employment status at baseline had greater risks of depression (aOR = 11.56, 95% CIs [3.48, 38.39]).
Discussion
We used a longitudinal design to identify the different patterns of chemsex engagement and to investigate the association between chemsex trajectory and moderate to severe depressive symptoms among GBMSM attending sexual health clinics in Taiwan. According to the GBTM, three distinct groups were identified: “never or rarely engaged,” “consistently engaged,” and “high, decreasing and reinitiated.” We found that the majority of participants were categorized as never use or rarely engaged. Furthermore, our data suggest that there was inconclusive evidence in the association between chemsex trajectories and moderate to severe depressive symptoms over the 2-year follow-up period. To the best of our knowledge, our study provides the first analysis examining the trajectories of chemsex engagement among GBMSM, as well as the longitudinal association between chemsex trajectory and depressive symptoms at an individual level.
Longitudinal studies on chemsex are not commonly seen in the literature. In contrast with the studies that used baseline data to categorize participants for their longitudinal observation of chemsex behavior, 26 we were able to categorize different chemsex patterns and observe changes within heterogeneous groups by using data from all time points. Besides this, we provided more informative results on longitudinal change than the studies that used data of one point, and thus reduced our risk of misclassification.
We categorized a small proportion of GBMSM as high, decreasing and reinitiated in terms of their engagement in chemsex. These individuals reported a decline in chemsex after enrollment but reported reinitiation at the last few visits of the follow-up period. The initial high proportion of chemsex engagement might reflect a possibility of heightened substance use at baseline. Since the study sample was recruited at two healthcare facilities with either chemsex support care or referral services, the decline in proportion may suggest the use of a chemsex intervention or support groups. Yet, future studies are needed to examine the effectiveness of chemsex care services. Relapse is not an uncommon phenomenon in relation to substance use36,37; however, research addressing relapse in the context of chemsex engagement is scarce. Our findings reinforce the importance of incorporating relapse prevention strategies into the intervention aiming to reduce the harm related to chemsex, especially in clients showing significant decline within a few visits.
The consistent users identified in our analysis reported a stable proportion of chemsex engagement throughout the follow-up period. The proportion of chemsex in this group, although lower than the initial proportion of the high, decreasing and reinitiated group, still consisted of a considerable amount of their sex lives. Considering that this group maintained their levels of chemsex over time, this finding may imply that some GBMSM derived pleasure from the use of the drugs and felt able to do so in ways that did not cause harm to themselves or others. 38
Our inconclusive finding regarding the association between chemsex trajectories and moderate to severe depressive symptoms contributes to the nuanced literature, where findings among GBMSM on the relationship between chemsex and depression have yielded mixed results. The studies that suggested a positive association are predominant. 13 These inconsistent findings may be due to the potential correlation between chemsex and depressive symptoms being more likely to occur when chemsex behavior is more frequent, severe, or when people are more dependent on chemsex. For example, a longitudinal study in the United Studies found that frequent substance use was associated with an increase in depressive symptoms in MSM, and that heavy use of methamphetamine—a drug commonly used in chemsex practice—was an influential predictor of persistent symptoms of depression. 39 In a cross-sectional context, a large online survey conducted in Australia revealed dependent methamphetamine users had a higher risk of moderate to severe depression than nondependent users. 19
Our study categorized chemsex according to the self-reported proportions of their sex lives involving drugs. Being classified as chemsex trajectories of consistently engaged or high, decreasing and reinitiated may have indicated heavy engagement but not necessarily dependent use. This may be a possible reason for not having a statistically significant association; in addition, the small sample size of some trajectory groups could have limited the power to detect an increase in the risk of moderate to severe depressive symptoms. Our study, however, assessed the association between chemsex behaviors and moderate to severe depressive symptoms from a community sample with a wide variation of chemsex behaviors, and was not limited just to people who were potentially dependent on chemsex.
The relationship between depression and chemsex is complex, influenced by both individual vulnerabilities and structural factors in Taiwan. In our sample of 262 GBMSM living with or without HIV from two large sexual health clinics in Taiwan, nearly one in six (17.2%) had clinically significant depressive symptoms at baseline. This prevalence was comparable to the observed among GBMSM living with HIV in Taiwan, 40 but substantially higher than that of the general population. 41
Additionally, previous research has indicated that some GBMSM in Taiwan experience severe psychological distress related to substance use and sexual health risks. 42 However, despite this significant burden, mental health and substance use services remain underutilized among GBMSM engaging in chemsex, highlighting structural and individual barriers to care. 11
There are several limitations in this study. First, our study's hypothesis testing was constrained by small group sizes that were slightly below the required sample size, limiting the power to detect significant differences and increases the risk of Type II error. This poses a challenge to interpreting null results, as the findings may be inconclusive or nondefinitive. However, the use of BFs provides insight into a null result from the frequentist hypothesis testing. Our ability to fully assess nuanced differences between chemsex patterns and their relationship with depressive symptoms is limited. Future research with larger and more balanced sample sizes is needed to provide a more robust understanding of these associations.
Second, missing data from follow-up measurements could have affected our findings. The number of observations from follow-up visits is presented in Supplemental File 4. The trajectory method assumes missing at random and applies full-information maximum likelihood correction within the original program. 43 Nonetheless, the high degree of missingness, particularly at later time points, may have introduced bias or reduced the precision of the estimated trajectories.
Third, attrition bias may be a concern because we restricted our sample to those with more than one wave of follow-up. The participants with very severe symptoms of depression requiring medical interventions may have been referred to other psychiatric services and could not be followed up in the original recruitment site. If so, the association between chemsex and depression may have been underestimated. However, moderate to severe depressive symptoms at baseline were not different comparing the study sample included and those who had fewer than two waves of follow-up.
Fourth, given that the study sample was recruited in two healthcare facilities specializing in chemsex, our participants might have received timely referrals and interventions when the clinicians or social workers sensed an urgent need for mental health care. Hence, our study results cannot be generalized to those engaging in chemsex within the community who have not received healthcare services for sexual health, mental health, and substance use. Fifth, the follow-up assessments may not have been frequent enough to detect acute changes in depression. It is possible that episodes of depression occurred between two observations. Future studies may consider using ecological momentary assessment to track depression either with self-reported tools or objective measurements such as a wearable device to record physiological changes.44,45 Sixth, a potential limitation of this study is that the VAS used to measure the extent of chemsex behaviors has not been formally validated for this specific purpose. While the VAS is a commonly used tool for assessing subjective experiences and behaviors in various fields, its application in quantifying chemsex involvement remains unvalidated. Future research should explore the reliability and validity of this approach to ensure its accuracy in capturing chemsex-related behaviors. Additionally, as with all self-reported measures, responses regarding chemsex engagement may be influenced by social desirability bias and recall bias, potentially affecting the accuracy of the data. Despite this limitation, the VAS provides a continuous measure that allows for nuanced assessments of behavioral changes over time.
Conclusions
Our study suggests the heterogeneity of chemsex behaviors among GBMSM but insufficient evidence to reach definitive conclusions on differences in moderate to severe depressive symptoms across the chemsex trajectories. These findings add to the body of knowledge showing the complex and multifaceted relationships between chemsex and depression. By understanding the diverse patterns of chemsex, healthcare professionals can provide person-centered approaches to meet the specific needs of different subgroups. We also found that moderate to severe depressive symptoms were prevalent among GBMSM attending sexual health clinics in Taiwan, which has reinforced the importance of integrating mental health care into sexual health care. These results highlight the importance for HIV healthcare providers acknowledging chemsex as a critical factor in their practice, as addressing it can play a vital role in harm reduction and effective HIV prevention and treatment strategies for GBMSM.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251339906 - Supplemental material for A Longitudinal Investigation of Chemsex and Its Relationship with Depressive Symptoms Among Gay, Bisexual Men and Other Men Who Have Sex with Men in Taiwan
Supplemental material, sj-docx-1-jia-10.1177_23259582251339906 for A Longitudinal Investigation of Chemsex and Its Relationship with Depressive Symptoms Among Gay, Bisexual Men and Other Men Who Have Sex with Men in Taiwan by Shih-Chun Hua, Stephane Wen-Wei Ku, PoYao Huang, Nai-Ying Ko, Chia-Wen Li, Adam Bourne and Carol Strong in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251339906 - Supplemental material for A Longitudinal Investigation of Chemsex and Its Relationship with Depressive Symptoms Among Gay, Bisexual Men and Other Men Who Have Sex with Men in Taiwan
Supplemental material, sj-docx-2-jia-10.1177_23259582251339906 for A Longitudinal Investigation of Chemsex and Its Relationship with Depressive Symptoms Among Gay, Bisexual Men and Other Men Who Have Sex with Men in Taiwan by Shih-Chun Hua, Stephane Wen-Wei Ku, PoYao Huang, Nai-Ying Ko, Chia-Wen Li, Adam Bourne and Carol Strong in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-3-jia-10.1177_23259582251339906 - Supplemental material for A Longitudinal Investigation of Chemsex and Its Relationship with Depressive Symptoms Among Gay, Bisexual Men and Other Men Who Have Sex with Men in Taiwan
Supplemental material, sj-docx-3-jia-10.1177_23259582251339906 for A Longitudinal Investigation of Chemsex and Its Relationship with Depressive Symptoms Among Gay, Bisexual Men and Other Men Who Have Sex with Men in Taiwan by Shih-Chun Hua, Stephane Wen-Wei Ku, PoYao Huang, Nai-Ying Ko, Chia-Wen Li, Adam Bourne and Carol Strong in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-4-jia-10.1177_23259582251339906 - Supplemental material for A Longitudinal Investigation of Chemsex and Its Relationship with Depressive Symptoms Among Gay, Bisexual Men and Other Men Who Have Sex with Men in Taiwan
Supplemental material, sj-docx-4-jia-10.1177_23259582251339906 for A Longitudinal Investigation of Chemsex and Its Relationship with Depressive Symptoms Among Gay, Bisexual Men and Other Men Who Have Sex with Men in Taiwan by Shih-Chun Hua, Stephane Wen-Wei Ku, PoYao Huang, Nai-Ying Ko, Chia-Wen Li, Adam Bourne and Carol Strong in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The authors are grateful to the study participants.
Author Contributions
SCH and CS conceived the data analytic design, analyzed the data, prepared the figures and tables, and wrote and edited the manuscript. SWK, PH, NYK, CWL and AB edited the manuscript.
Data Availability Statement
Data is available upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The study protocol was approved by the Institutional Review Board of National Cheng Kung University Hospital (IRB: B-BR-107-076-T), and all participants provided written informed consent prior to joining the study.
Funding
This study was funded by the National Science and Technology Council (NSTC 112-2636-B-006-007, NSTC 112-2314-B-006-081-MY3) and the Taiwan Ministry of Health and Welfare, Centers for Disease Control (MOHW107-CDC-C-114-000107, MOHW108-CDC-C-114-000106).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.