
Abstract
Globally, gay, bisexual, and other men who have sex with men (GBMSM) are disproportionately affected by HIV, but few interventions address mental health and HIV outcomes among GBMSM living with HIV. The purpose of this study was to pilot a multicomponent intervention, integrating emotional well-being (EW) and health navigation for GBMSM living with HIV in Guatemala City. We implemented a 12-month intervention, including a four-session EW component and a health navigation component among newly diagnosed and reengaged GBMSM with HIV (n = 112). We conducted socio-behavioral surveys at baseline and endline to measure patient characteristics and HIV, and mental health outcomes as well as viral load testing. We documented participation in EW sessions and used a smartphone application to track navigation mode, frequency, and content. Using first-difference estimation modeling, we assessed associations between participation in EW and navigation and mental health (depression and anxiety symptoms) and HIV outcomes (HIV treatment adherence, viral suppression). Acceptability was high for EW (86%) and navigation (99%). During the intervention, viral suppression increased significantly and anxiety and depression decreased significantly. Participation in EW sessions and greater navigation frequency and duration were associated with being suppressed, whereas higher emotional navigator support was associated with being unsuppressed. Participation in EW sessions was associated with reduced anxiety. Findings suggest that multicomponent interventions integrating individual counseling and navigation may promote EW and sustained viral suppression. Future intervention research is needed to confirm whether HIV and mental health outcomes are attributable to the intervention and to assess mechanisms of influence.
Keywords
Gay, bisexual, and other men who have sex with men (GBMSM) are disproportionately affected by HIV. Globally, the risk of acquiring HIV is 25 times higher among GBMSM than the general adult population (UNAIDS, 2021a). In Latin America, GBMSM accounted for 46% of new HIV infections in 2020 (UNAIDS, 2021b).
Despite significant advances in treatment and care, the emotional impact of HIV diagnosis and managing life with HIV can be substantial and is exacerbated by intersectional stigma related to HIV, sexual orientation, gender, and limited social support (Barrington et al., 2016; Cloete et al., 2008; Davis et al., 2017; Kennedy et al., 2013; Moore et al., 2019 J. P. Yang et al., 2018; X. Yang et al., 2020). A recent meta-analysis found a pooled prevalence of depression among GBMSM with HIV of 43%, who were 1.46 times more likely to be depressed compared with GBMSM without HIV (95% CI = [1.05, 2.03]; Xiao et al., 2020). The mental health consequences of HIV can negatively affect HIV care and treatment outcomes, including retention in care, adherence to antiretroviral treatment (ART), and viral suppression. After diagnosis, psychological distress from HIV and sexuality-related stressors is a significant risk factor for delayed initiation of HIV care and abandonment among GBMSM (Beyrer et al., 2013; Hussen et al., 2015; Mayston et al., 2014; Rane et al., 2018; Sprague & Simon, 2014). Furthermore, anxiety and depression are associated with lower ART adherence, viral suppression, and quality of life among GBMSM (Crim et al., 2020; Downing et al., 2016; Penedo et al., 2003).
The period following HIV diagnosis or reengagement in care is a key opportunity to offer informational, instrumental, and emotional support to reduce feelings of fear, doubt, and shame, among others, and promote emotional well-being (EW). EW is the ability to adapt to adversity or change and achieve and sustain positive mental health outcomes (National Institutes of Health [NIH], 2022). Interventions for GBMSM with HIV developed in the 1990s included counseling and support services after diagnosis. The focus of these interventions was on grief and acceptance as limited treatment options existed (Lutgendorf et al., 1994, 1998). Subsequently, there was an added component of patient-centered approaches to risk reduction and preventing ongoing transmission, guided by the “positive prevention” and “Positive, Health, Dignity, and Prevention” frameworks (Koblin & Team, 2004; Sikkema et al., 2011, 2014).
In this era of improved access to ART and “treatment as prevention” and “U=U” (undetectable = untransmittable) frameworks, there is increased recognition of the need for interventions to support sustained and EW as a key component of sustained viral suppression (van Luenen et al., 2018). Programs combining motivational interviewing–based counseling and continuous peer support to promote EW were acceptable to GBMSM in two settings in Kenya (Graham et al., 2015, 2020; Kunzweiler et al., 2018) and significantly improved viral suppression (Graham et al., 2020). A recent pilot of a three-session cognitive-behavioral therapy skill-based intervention for newly diagnosed GBMSM (n = 10) in China was also acceptable to participants and initial results suggested improved mental health and resilience, key determinants of HIV outcomes (J. P. Yang et al., 2018). There is a need for applied research to continue developing an evidence base for strategies to promote EW and optimal HIV outcomes among GBMSM.
The HIV epidemic in Guatemala reflects global and regional trends; adult HIV prevalence at the national level in Guatemala is estimated to be less than 1% (Miller et al., 2010), compared with 10.5% among GBM (Guardado Escobar et al., 2017). Although GBMSM are the target population of HIV prevention efforts in Guatemala, there is no holistic programming tailored to promote EW and optimal HIV outcomes among GBMSM with HIV. The purpose of this study was to assess acceptability and initial effects of a multicomponent intervention integrating individual counseling and health navigation to promote mental health, ART adherence, and viral suppression among recently diagnosed and reengaged GBMSM with HIV in Guatemala City.
Materials and Method
Study Design and Intervention
We implemented a 12-month pilot study of a multicomponent intervention to promote EW and viral suppression among GBMSM with HIV in Guatemala City. Intervention components included (1) EW, and (2) HIV care navigation.
The EW component included four sessions guided by an intervention manual and facilitated by a trained psychologist. Based on insights from formative qualitative research in Guatemala (Barrington et al., 2016), we adapted two intervention manuals developed by our team in other settings (Carcaño et al., 2015; Donastorg et al., 2014). Across all EW sessions, the psychologist offered tools to cope with emotions and raise self-esteem. Each session had a specific focus: Session 1 focused on social support and stigma; Session 2 focused on general information about HIV, adherence to ART, and substance use; Session 3 focused on sexual health, partnerships, and disclosure; and Session 4 focused on developing a life plan.
Participants were not receiving other support interventions as part of standard HIV care during this time. Each session lasted approximately 1 hour and was held in a private office in the Roosevelt hospital, usually on the same day as participants’ HIV care appointments, which occurred every 3 months during the 12-month intervention. During each session, the psychologist and participant identified situations that were causing worry or stress and appropriate strategies to address these situations.
The second intervention component was HIV care navigation (hereafter referred to as navigation), a strengths-based model to support people with HIV to promote sustained engagement in care and adherence to ART (Bradford et al., 2007; Mizuno et al., 2018). Nine navigators were trained to support participants to (1) address barriers to care, (2) develop strategies to use existing resources, (3) cultivate resources to maintain health and well-being, and (4) advocate for their rights. Most navigators had experience working with HIV or other health-related programs; some were peers in terms of HIV status and sexual orientation, but this was not a requirement. The average navigator age was 28 years and most had completed some university education; the most common area of study was psychology. Each navigator was assigned 30 to 60 participants. Beyond providing appointment reminders, navigators were expected to maintain, at a minimum, monthly communication with each participant. Navigators provided reminders and accompaniment to HIV appointments, assisted with HIV status disclosure, sent motivational messages, and discussed personal, professional, and HIV-related issues with participants. Navigation interactions occurred in person, through phone conversations, and through virtual texting/chatting. Additional details of the navigation component are described elsewhere (Alvis-Estrada et al., 2021; Davis, Angeles, et al., 2021).
Sample Recruitment and Retention
From January to June 2017, we recruited 112 GBMSM with HIV at the Roosevelt Hospital in Guatemala City. Eligibility included being at least 18 years old, assigned male sex at birth and identified as male, self-reported ever having sex with men, Spanish-speaking, and diagnosed with HIV or reengaged in HIV care within the past 12 months and currently receiving HIV care at Roosevelt. All participants provided informed consent. Participants were approached and screened when they came for regular HIV care appointments. Ten participants were lost to follow-up, resulting in 91.8% retention at 12 months. This study was reviewed and approved by the institutional review boards of the University of North Carolina at Chapel Hill and the Universidad del Valle de Guatemala.
Assessment
We conducted socio-behavioral surveys and viral load testing at baseline (January–June 2017) and end line (January–June 2018). Surveys were administered in Spanish by trained interviewers in private locations in the clinic, using tablets. We collected data on navigation from an app-based monitoring system of participant–navigator interactions. The navigation monitoring system allowed navigators to document information about each interaction with participants, including mode of interaction (in person or remote), duration of the interaction (in number of minutes), and content of the interaction (e.g., appointment reminder, HIV education, and emotional support; Alvis-Estrada et al., 2021). The study psychologist documented the number of EW sessions attended by each participant.
Measures
Outcomes
Viral Load and Suppression
We obtained viral load count (measured as copies of virus/mL) at baseline and end line. Participants with a viral load of 400 copies/mL or less were defined as virally suppressed. Participants with <20 copies/mL were recoded as 0 copies/mL.
HIV Treatment Behaviors
We asked participants to respond “yes” or “no” to whether they had suspended ART (ART interruption) in the past 6 months. For ART adherence, we used the AIDS Clinical Trials Group (ACTG) adherence measure and asked whether they had missed any ART doses in the past 4 days (Fletcher et al., 2005); we categorized anyone who had missed a dose as non-adherent.
Anxiety and Depressive Symptoms
We screened for symptoms of anxiety during the past 2 weeks, using the two-item Generalized Anxiety Disorder assessment (GAD-2; Plummer et al., 2016), and depressive symptoms during past 2 weeks, using the two-item Patient Health Questionnaire (PHQ-2; Kroenke et al., 2003). Scores for both measures were summed (range = 0–6), with a score of 3 considered the optimal cut point for screening purposes.
Intervention Acceptability and Participation
We assessed acceptability based on whether participants decided to enroll in each component (yes/no).
We used monitoring data from the study psychologist and the navigation monitoring system to create measures of intervention participation (Alvis-Estrada et al., 2021; Davis, Angeles, et al., 2021).
EW Participation
We dichotomized participation based on attending all four sessions (high) compared with attending zero to three sessions (low). This categorization was based on our interest in assessing the experience of the individual who completed all intervention sessions, which was roughly half (52.1%) of the sample.
All navigation variables were calculated over the 12-month intervention period.
Navigation Frequency
A count of the number of documented interactions, remote or in person, between navigator and participant.
Navigation Minutes
A count of minutes reported from every navigator–participant interaction over the 12-month intervention period. Some remote interactions were 0 minutes due to the nature of the interaction, such as appointment reminders or brief text message.
Proportion of In-Person Navigation Interactions
The number of in-person interactions divided by the count of all interactions (in person and remote).
We categorized topics covered in navigator–participant interactions into three forms of social support: emotional, instrumental, and informational (Heaney & Israel, 2008). Levels of low, medium, high, and very high were created based on distribution quantiles for each variable.
Emotional Navigation Support
Interactions categorized by navigators as addressing support for mental health, alcohol, drugs, and concerns related to family, work, or partners. For interpretability, levels of emotional support were assigned using dummy variables: low (0%–50%; 0–4 interactions), medium (51%–75%; 5–9 interactions), high (76%–90%; 10–13 interactions), and very high (91%–100%; 14–55 interactions).
Instrumental Navigation Support
Interactions categorized by navigators as appointment reminders. For interpretability, levels of instrumental support were assigned using dummy variables: low (0%–50%; 0–3 interactions), medium (51%–75%; 4–5 interactions), high (76%–90%; 6–8 interactions), and very high (91%–100%; 9–20 interactions).
Informational Navigation Support
Interactions categorized by navigators as provision of information about HIV, legal framework, STI, sexual health, opportunistic infections, clinic, lab, counseling, and biosecurity. For interpretability, levels of informational support were assigned using dummy variables: low (0%–50%; 0–3 interactions), medium (51%–75%; 4–6 interactions), high (76%–90%; 7–10 interactions), and very high (91%–100%; 11–38 interactions).
Data Analysis
We used chi-square tests to assess whether mental health and HIV outcomes were significantly different between baseline and end line (p < .05). We used first-difference estimation to assess whether having attended all four EW sessions and navigation characteristics were associated with HIV and mental health outcomes. Proportion of in-person navigation interactions was excluded from models as preliminary analyses showed it was not significantly associated with any outcomes. First-difference estimation is an extension of fixed effects regression used to control for all stable characteristics of individuals, observed or unobserved, in longitudinal analyses (Allison, 2005). For each outcome, we ran three models: Model 1 examined the association between attending all four EW sessions and outcomes, Model 2 examined the association between characteristics of navigation and outcomes, and Model 3 examined the combined effect of attending all four EW sessions and characteristics of navigation on outcomes. We assess the beta coefficient estimate and the associated p value (<.05 considered significant). All analyses were conducted using SAS Version 9.4.
Results
Sample Baseline Characteristics
The mean age was 26 years (range = 18–58 years; Table 1). Most participants self-identified as gay (74.9%) and Mestizo/Ladino (mixed Indigenous, European, and African ancestry; 92.8%). More than 40% (41.1%) had at least some college education and the majority (70.5%) were employed at the time of the survey. It is possible that some participants who had part-time or informal employment responded “no” to the current employment question, despite doing some paid work. The median monthly income was US$352 (range = $0–$2,632). The median number of days since HIV diagnosis was 114.5 (range = 1–2,294); most participants (86.6%) had been diagnosed with HIV in the previous 12 months while 13.4% had been reengaged in HIV care.
Baseline Sociodemographic Characteristics and Changes in Mental Health and HIV Outcomes Among GBMSM Living With HIV in Guatemala (N = 112).
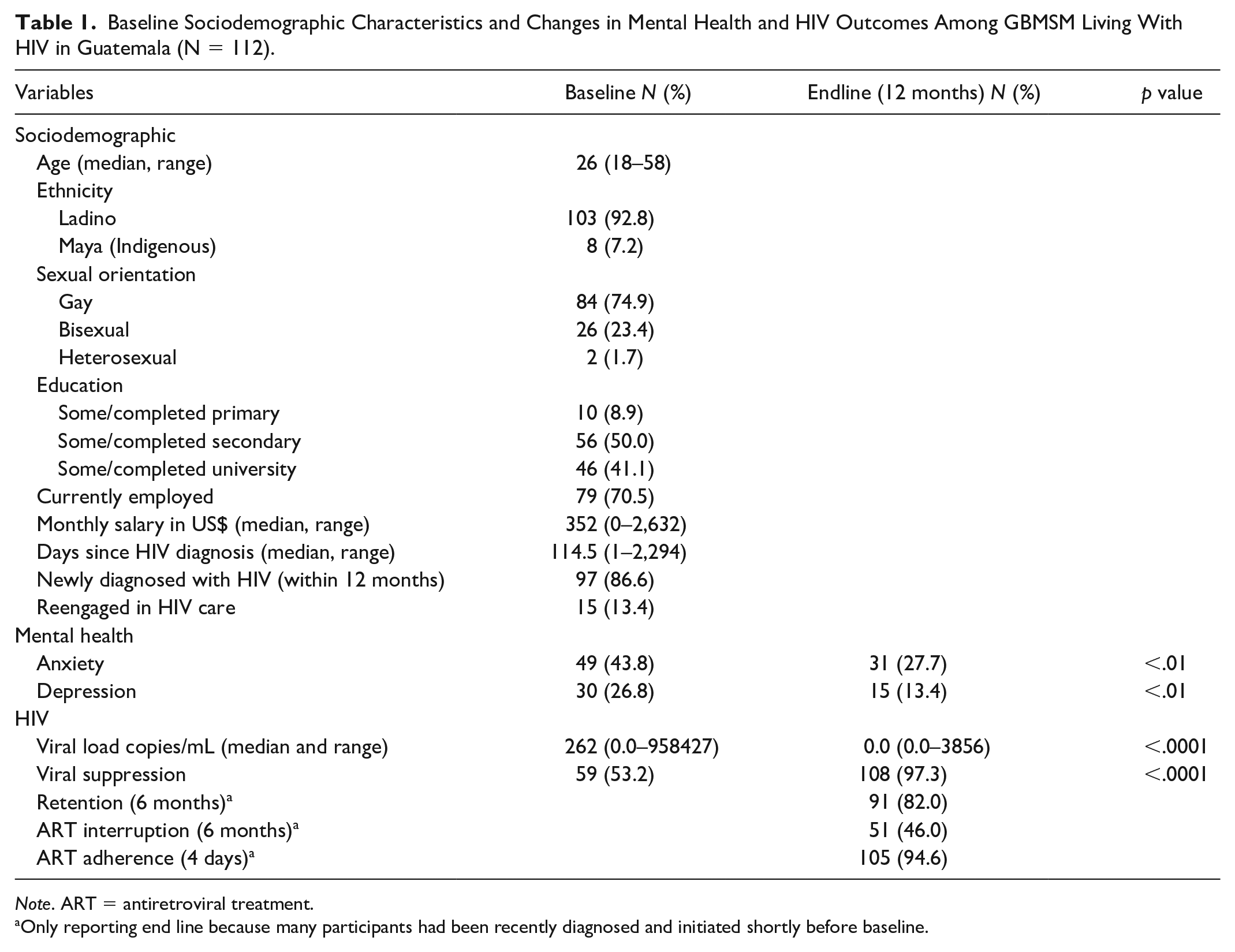
Note. ART = antiretroviral treatment.
Only reporting end line because many participants had been recently diagnosed and initiated shortly before baseline.
Intervention Acceptability and Participation
Of the 112 participants enrolled in the intervention, 96 (85.7%) accepted participation in the EW component (Table 2). The reasons for not accepting participation included feeling emotionally well and lack of time. Over half of those who accepted participation (n = 50, 52.1%) attended all four EW sessions, 17 (17.7%) attended three sessions, 16 (16.7%) attended two sessions, 11 (11.5%) attended one session, and two (2.1%) attended no sessions. The reasons for not attending all four sessions was mostly due to time limitations due to work; of note, however, being employed was not correlated with number of sessions attended (data not shown). All but one participant accepted participation in the navigation component (99.1%). The median number of navigation interactions during the intervention period was 11 (range = 1–46) and the median portion of in-person navigation interactions was 0.33 (range = 0.0–1.0). The median duration of total navigation interactions was 918 minutes (range = 0–3,440).
Emotional Well-Being and Navigation Participation Among GBMSM Living With HIV in Guatemala (N = 112).
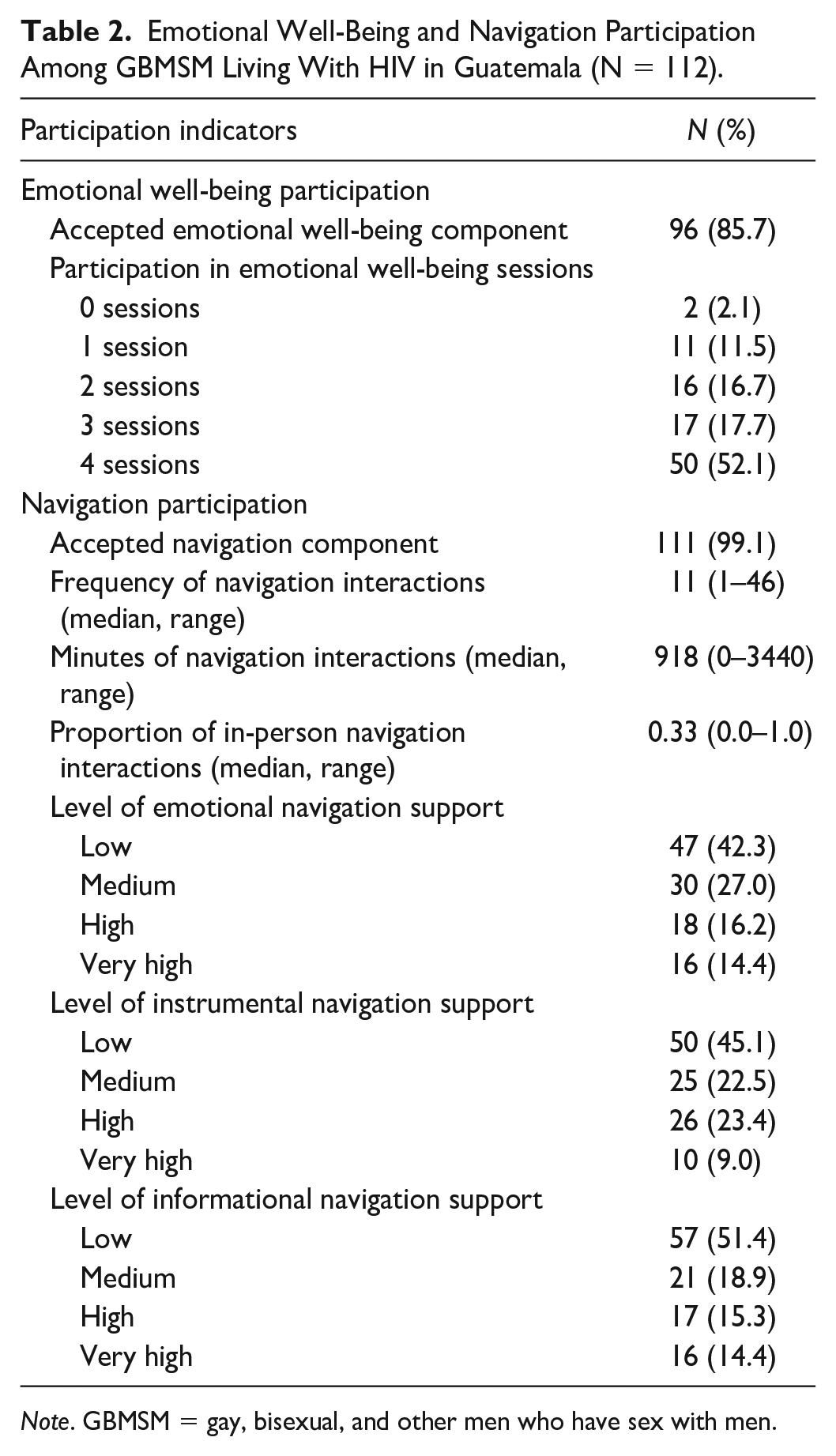
Note. GBMSM = gay, bisexual, and other men who have sex with men.
Changes in HIV and Mental Health Outcomes
Overall, participants experienced significant improvements in mental health and HIV outcomes between baseline and end line (Table 1). Fewer participants screened for anxiety (43.8%–27.7%; p < .01) and depressive symptoms (26.8%–13.4%; p = .01). In addition, median viral load decreased significantly from 262 copies/mL to 0 copies/mL (p < .001) and the proportion of participants who were virally suppressed significantly increased (53.2%–97.3%; p < .001). At end line, nearly half of the sample (46.0%) reported having interrupted their ART treatment in the past 6 months but most reported perfect adherence in the past 4 days (94.6%).
Multivariable Analyses
EW Model
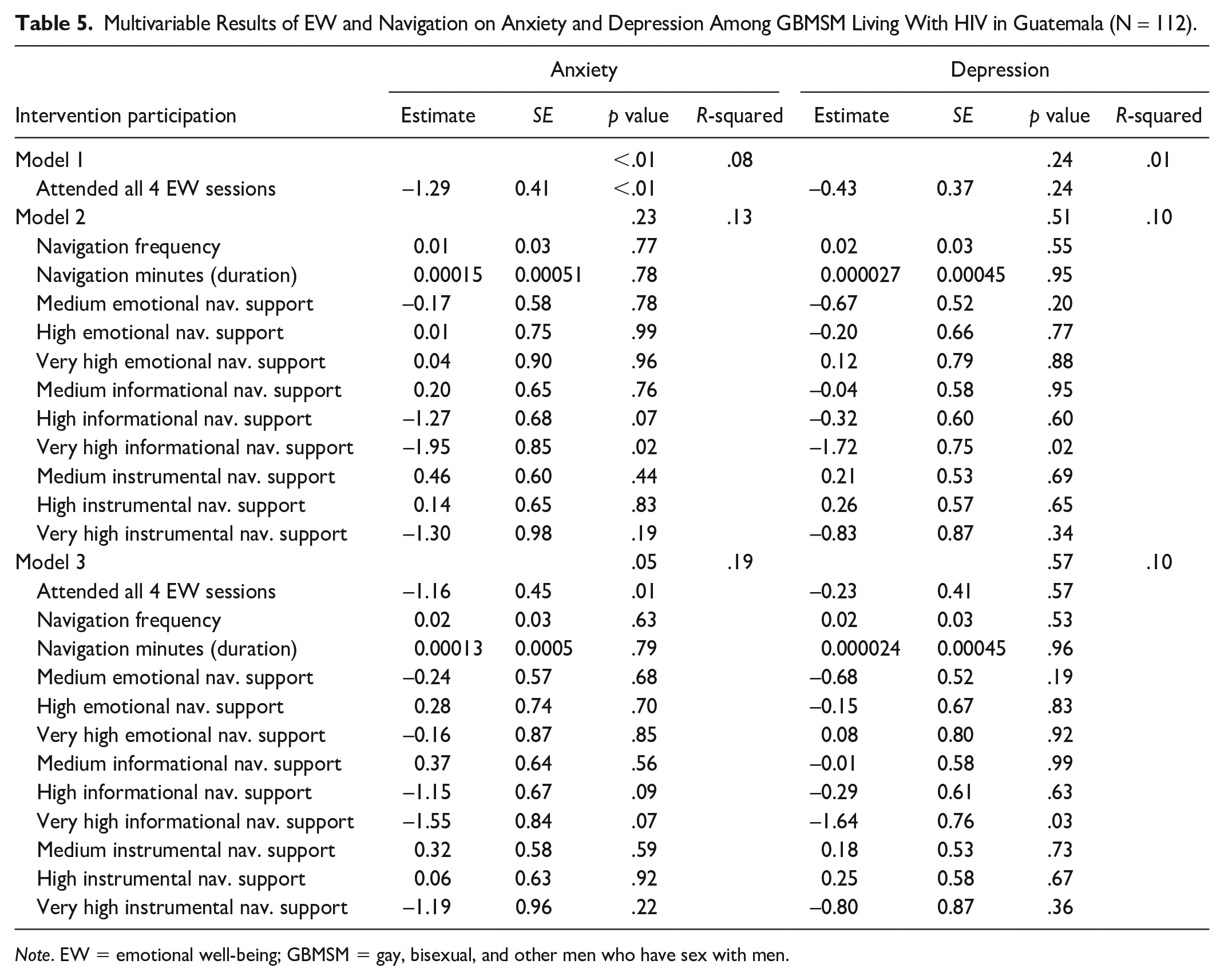
Attending all four EW sessions was significantly associated with a reduction in viral load (B = −50,381, SE = 20,071, p < .01), being viral suppressed (B = .26, SE = .10, p < .01), and an improvement in anxiety (B = −1.29, SE = 0.41, p < .01) compared with participants who attended three or fewer sessions (Tables 4 and 5). Participation in four EW sessions was not associated with depression, ART interruption, or ART adherence.
Navigation Model
Navigation characteristics were significantly associated with ART interruption (p = .04; Table 3). Participants with more navigation minutes were significantly more likely to report ART interruption (B = 0.00044, SE = 0.00012, p < .001); however, participants were less likely to have interrupted ART if they reported medium (B = −0.31, SE = 0.14, p = .03), high (B = −0.55, SE = 0.16, p < .001), and very high levels of instrumental navigation support (B = −0.54, SE = 0.24, p = .02) compared with participants with low levels of instrumental navigation support. Navigation was significantly associated with viral load (p < .01). Participants who received very high levels of emotional navigation support experienced a 104,734 copies/mL reduction in viral load (SE = 40,326, p = .01) compared with those with low levels of emotional navigation support. In addition, participants who received very high levels of instrumental navigation support experienced a 126,639 copies/mL reduction in viral load (SE = 44,337, p < .01) compared with those with low levels of instrumental navigation support. Navigation was also significantly associated with viral suppression (p = .01). Participants with higher frequency of navigation interactions (B = 0.01, SE = 0.01, p = .05) and more minutes of navigation interactions (B = 0.00026, SE = 0.00012, p = .03) were more likely to be virally suppressed. However, participants who received very high levels of emotional navigation support were less likely to be suppressed (B = −0.42, SE = 0.21, p = .05). Navigation characteristics were not significantly associated with ART adherence, anxiety, or depression (Tables 3 and 5).
Multivariable Results of EW and Navigation on HIV Outcomes Among GBMSM Living With HIV in Guatemala (N = 112).
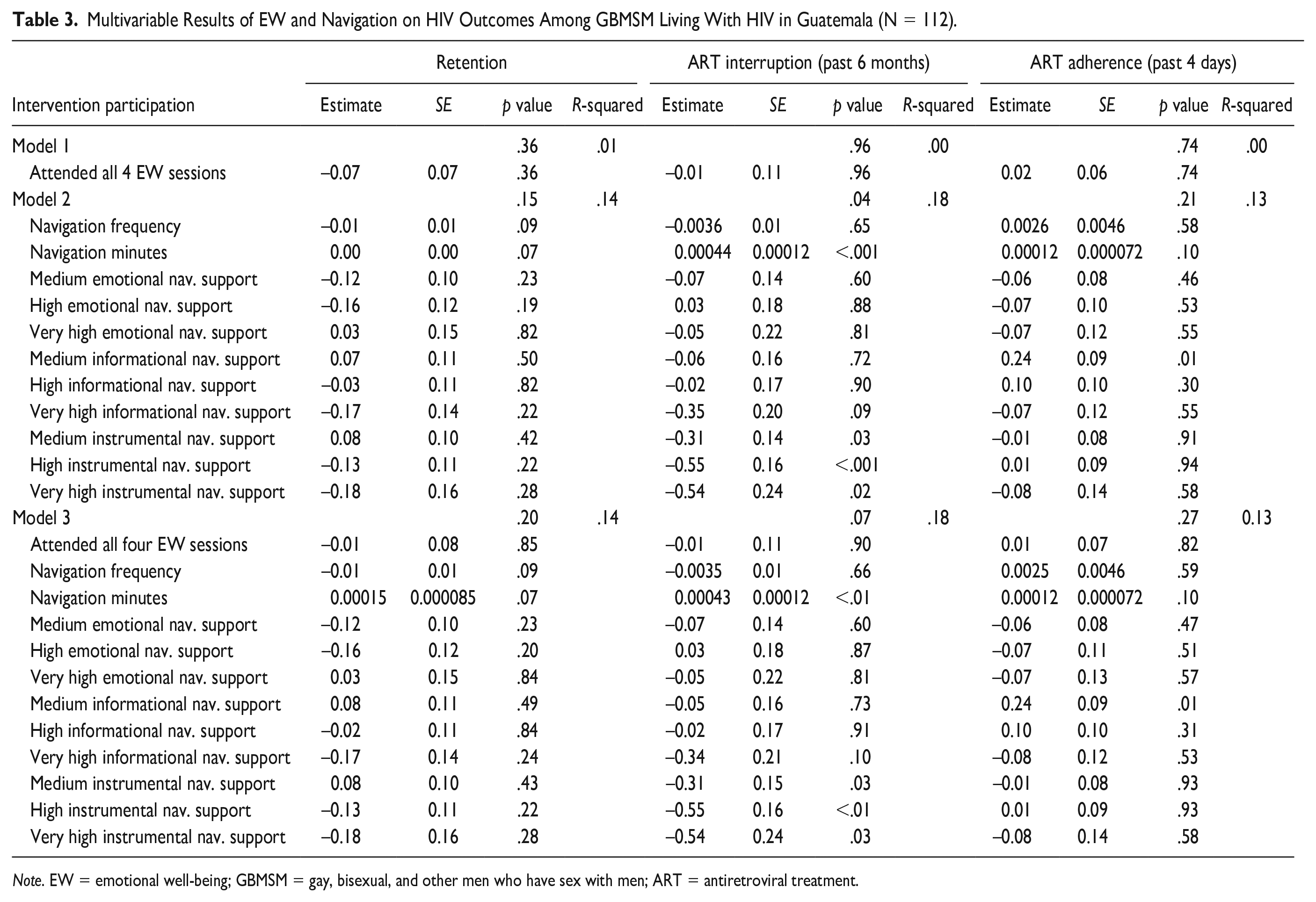
Note. EW = emotional well-being; GBMSM = gay, bisexual, and other men who have sex with men; ART = antiretroviral treatment.
EW and Navigation Model
The multivariable model, including both EW and navigation, was significantly negatively associated with viral load (p < .001; Table 4). Viral load was lower by 60,761 copies/mL (B = −60,761, SE = 20,253, p < .01), among participants who attended all four EW sessions compared with participants who attended zero to three sessions. In addition, receipt of very high levels of emotional navigation support was associated with a 115,013 copies/mL reduction in viral load (SE = 38,895, p < .01) and receipt of very high instrumental navigation support was associated with a 119,830 copies/mL reduction in viral load (SE = 42,658, p < .01) compared with participants who received low levels of emotional and instrumental support, respectively. The full model was also significantly associated with viral suppression (p < .01). Participants were more likely to be virally suppressed with more minutes of navigation interactions (B = 0.00026, SE = 0.00012, p = .03). The full model was also significantly associated with anxiety (p = .05) (Table 5). Participation in all four EW sessions was associated with a reduction of 1.16 points (B = −1.16, SE = 0.45 p = .01) in anxiety compared with participants who attended zero to three sessions. The combined model was not significantly associated with depression, ART interruption, or ART adherence.
Multivariable Results of EW and Navigation on HIV Outcomes Among GBMSM Living With HIV in Guatemala (N = 112).
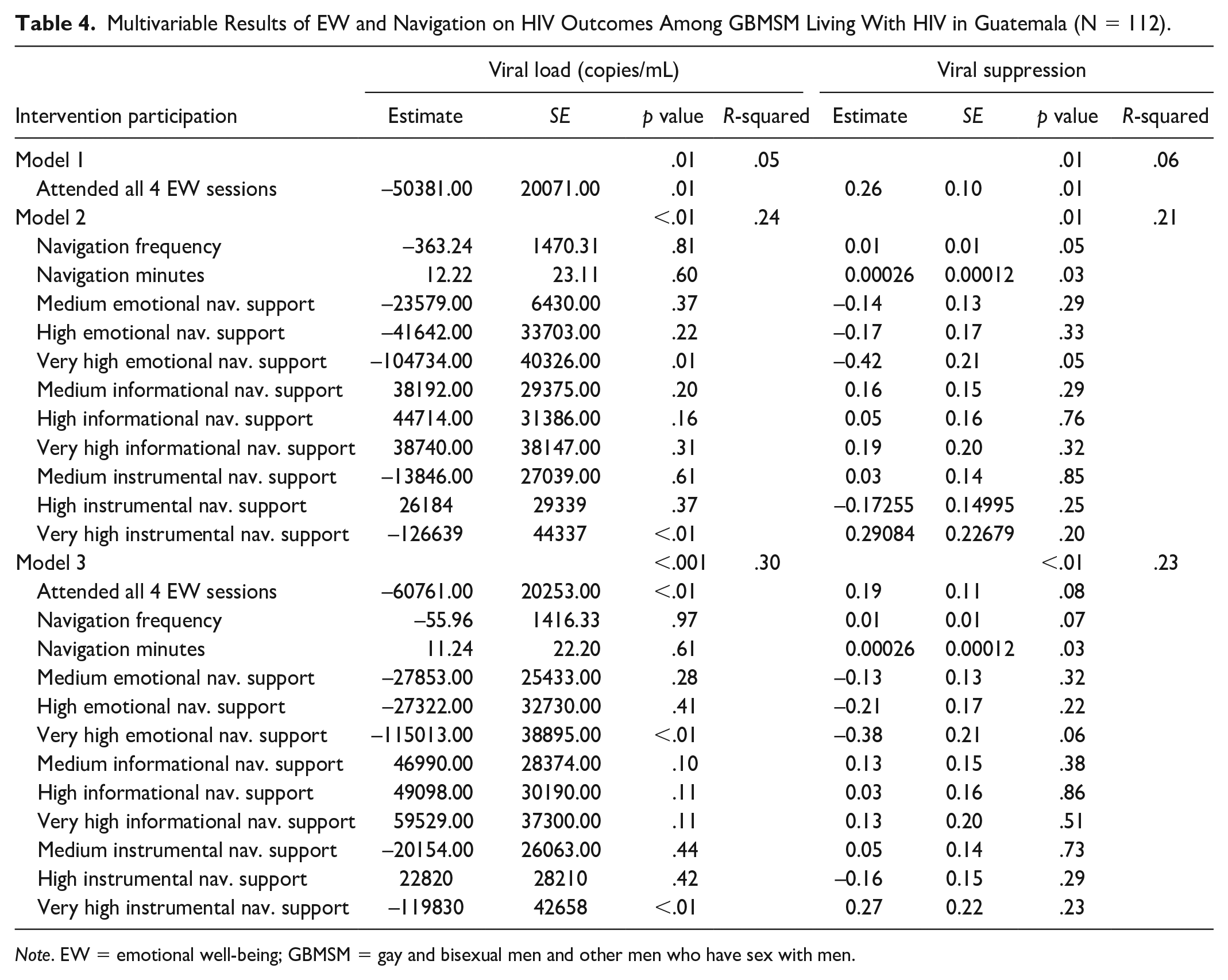
Note. EW = emotional well-being; GBMSM = gay and bisexual men and other men who have sex with men.
Multivariable Results of EW and Navigation on Anxiety and Depression Among GBMSM Living With HIV in Guatemala (N = 112).
Note. EW = emotional well-being; GBMSM = gay, bisexual, and other men who have sex with men.
Discussion
We documented significant improvements in viral load and mental health (anxiety and depression symptoms) among newly diagnosed and reengaged GBMSM living with HIV who participated in a multicomponent intervention, including EW sessions and navigation. Reductions in viral load and improvements in suppression were significantly associated with participation in EW sessions and engagement with navigators. Reduced anxiety was significantly associated with participation in EW sessions. Together, these findings provide encouraging support for the use of multicomponent interventions to promote EW and viral suppression among newly diagnosed and reengaged GBMSM.
Overall, intervention acceptability was high for both EW (85.7%) and navigation (99.1%) components. Although study retention was also high (91.8%), there was variation in the intensity of participation in EW sessions, with approximately half (52.1%) of participants who enrolled in the EW component completing all four EW sessions. A few (approximately four or five) participants requested an additional ad hoc session with the psychologist, reflecting the range of needs for this kind of support; these additional sessions were provided. Time was the main barrier to participation, highlighting a need to maximize time while also attending to patients’ holistic needs beyond clinical care. As HIV care is increasingly delivered in decentralized models with reduced numbers of appointments, there may be an opportunity to dedicate some of the time saved to EW without overly burdening patients and providers.
A subgroup of participants (n = 10) who also participated in qualitative interviews indicated that the sessions helped them reach diagnosis acceptance, improve self-esteem, and gain self-efficacy for managing life with HIV, which may explain the significant association between participation in EW sessions and reduced anxiety (Bartels et al., 2022). They also appreciated clarifying life goals and developing a life plan in the final session. Collaborative, problem-solving approaches were also acceptable and effective in a multicomponent intervention, including individual sessions and peer navigation with GBMSM living with HIV in Kenya (Graham et al., 2020) and trans women living with HIV in the Dominican Republic (Barrington et al., 2020).
The median number of navigator interactions during the 12-month intervention period (n = 11) was in-line with our target of one interaction per month. Beyond tracking the number of interactions, our navigation monitoring system also allowed for calculating duration (minutes of interaction), mode, and types of support, which provides more nuanced understanding of this component. Overall, participation in navigation was associated with HIV outcomes more than mental health outcomes; only very high informational support was associated with reduced anxiety and depressive symptoms. Informational support from navigators was also a key component of an intervention with MSM living with HIV in Kenya (Graham et al., 2020). In qualitative interviews, participants in our study explained that navigators facilitated access to information about HIV in general and specifically about the process of receiving care at the clinic, which, they explained, reduced fear and worry (Davis, Muessig, et al., 2021).
We found associations between both navigation duration and type of support and HIV treatment outcomes. The significant association between more navigation minutes and ART interruption in the past 6 months may reflect that navigators spent more time engaging with these participants to support treatment reinitiation. In contrast, increased navigator minutes was positively associated with being suppressed, which may reflect the overall positive impact of having the support of a navigator. All levels of instrumental support were associated with less ART interruption; as instrumental support was a proxy for accompaniment to appointments, it is possible that this association reflects that such support was more likely to be provided to participants who were engaged in care. Participants who received very high levels of emotional navigation support had significant reductions in viral load but were less likely to be suppressed, which may be due to the higher viral load at baseline or greater challenges with adherence. Individuals with higher viral load may require more support as they adapt to their diagnosis and integrate care and treatment into their lives. In a study of rapid ART initiation among MSM in several West African countries, one third of participants were not retained over a 2-year period, highlighting the need for low-cost and accessible forms of support, such as navigation, to sustain ART use (Dah et al., 2021). Even among individuals who are engaged in care and adherent to ART, acute crises and life challenges can lead to interruptions in care and treatment and navigators may be well positioned to provide support at such times (Davis, Muessig, et al., 2021).
Future research is needed to improve understanding of the mechanisms underlying the associations between EW, navigation, and mental health and HIV outcomes. It is important to explore the role EW and navigation play in supporting treatment initiation, adherence, and viral suppression. Implementation science to determine the minimum dose of EW sessions and navigation could improve targeting and enhance cost-effectiveness and sustainability. Finally, navigators included individuals who were peers with participants in some aspect of their identity (sexual orientation, gender identity, or HIV status), but not all navigators were peers. More research is needed on the role of peer navigators versus non-peers to identify essential characteristics of effective navigators.
Our study had limitations. We lacked a comparison group, limiting our ability to attribute outcomes to the intervention. Notably, we did not find significant changes in anxiety or depression among the 18 participants who did not participate in any individual sessions (data not shown), which supports the possibility that the intervention contributed to these outcomes among those who did participate. Related, our sample was predominantly newly diagnosed and did not include enough reengaged participants to support stratified analyses, which would have provided more nuanced understanding of their intervention experience and outcomes. Finally, as nearly all participants accepted both components, we are not able to look at the two components separately, although this was not the intention of the multicomponent model.
Conclusion
Newly diagnosed and reengaged GBMSM living with HIV had reductions in anxiety and depressive symptoms and viral load while participating in a multicomponent intervention integrating EW sessions with navigation. Findings support the potential for multicomponent interventions to holistically address the distinct needs and challenges of GBMSM living with HIV to promote well-being and sustained viral suppression.
Footnotes
Acknowledgements
The authors are grateful to the study participants for providing their time and sharing their experiences. The authors would also like to acknowledge colleagues at the Universidad del Valle de Guatemala, the Unidad de Atención Integral del VIH e Infecciones Crónicas del Hospital Roosevelt, and the University of North Carolina who contributed to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The presentation of this material was supported by the Presidential Emergency Plan for AIDS Relief (PEPFAR) through the U.S. Centers for Disease Control and Prevention (CDC), under the terms and conditions of the Cooperative Agreement with the Universidad del Valle de Guatemala No. 1U01GH001003-05. Dr. Shelus was supported by NICHD of the National Institutes of Health, under award number P2C HD05092, and Dr. Barrington by NIA, under award number P30 AG066615. Dr. Davis was supported by the National Institutes of Health Ruth L. Kirschstein National Research Service Award, under award number 5T32AI007392. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agencies.