
Abstract
Background
Human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS) counselors play a crucial, albeit challenging, role in preventing and controlling HIV. People living with HIV (PLHIV) need emotional support in addition to clinical treatment. Counseling is more difficult for female counselors, considering the psychological and emotional aspects of HIV counseling.
Methodology
A qualitative study design was used to understand the complexity of the challenges faced by female HIV counselors. Interpretative phenomenological analysis (IPA) was employed as the research design. A small, homogeneous sample was purposively selected, comprising all 11 female HIV counselors in the Kashmir province and one female counselor in Leh (Ladakh). The IPA methodology was utilized, which emphasizes meaning-making and understanding the counselor's perspectives. The study was conducted from December 2022 to January 2023, with data collected through in-depth interviews at the counselors’ workplaces and via Zoom for the Leh participant. Data were analyzed thematically using the IPA approach, revealing the counselors’ real-life experiences, perceptions, and challenges.
Results
The analysis generated two superordinate themes with multiple overarching themes and sub-themes: Intrusive emotional and psychological experiences: Counselors experienced significant emotional strain, including emotional exhaustion, burnout, and stigma. Inadequate skills for effective counseling of people who inject drugs (PWID): Limited training hindered effective counseling for substance users and PWID, highlighting the need for specialized training.
Conclusion
Female HIV counselors in Kashmir face numerous psychological and emotional challenges, including emotional exhaustion, burnout, and stigma. Additionally, there is a lack of adequate training for counseling substance users. Addressing these issues through specialized training, stigma reduction initiatives, and mental health support is crucial for improving HIV counseling services and the overall HIV/AIDS response in the region.
Plain Language Summary
Background
HIV/AIDS counselors are essential in preventing and controlling the disease. Female counselors, in particular, face many psychological and emotional challenges.
Methodology
To understand what female HIV counselors in Kashmir and Leh go through, a qualitative study was done using a method called Interpretative Phenomenological Analysis (IPA). Twelve female HIV counselors took part in the study, which ran from December 2022 to January 2023.
Results
The analysis revealed two main themes: Emotional and psychological challenges: Female HIV counselors often experience emotional exhaustion, burnout, and stigma. They deal with a lot of stress and emotional strain in their work. Inadequate skills for counseling people who inject drugs (PWID): These counselors also feel they lack proper training to effectively counsel people who inject drugs, making their job even harder.
Conclusion
Female HIV counselors in Kashmir face significant psychological and emotional challenges. The lack of proper training, especially for dealing with substance users, worsens these issues. There is a need for better support and training to help these counselors manage the complex issues of HIV counseling, psychological health, substance use, and stigma.
Keywords
Introduction
In India, HIV prevalence in adults (15–49 years) is estimated at 0.22%. 1 The prevalence has declined from an estimated 0.54% in 2000–01 to the current levels—an estimated decline of 33.3%. 1 Early testing and diagnosis are essential for HIV prevention, treatment, care, and other support services. This needs increased access to and uptake of HIV testing among at-risk groups. HIV counseling and testing services include pre-test and post-test counseling, informed consent, privacy, and confidentiality, among other services. 2 An HIV/AIDS counselor thus plays a crucial, albeit challenging, role in preventing and controlling HIV. People living with HIV (PLHIV) need emotional support in addition to clinical treatment. Counseling such patients comes with varied challenges, especially in the cultural and social context of Kashmir. Counseling is more challenging for female counselors considering the psychological and emotional aspects of HIV counseling. Conducting a study on the mental or psychological well-being of female HIV counselors had a ground for several reasons. These include the distinctive emotional challenges they encounter, the professional expectation to manage emotions while providing support for those affected by HIV and AIDS, the stigmatization and fear of infection associated with their work, and the stress arising from personal connections to the issue. Additionally, the study recognizes the need to address the unique challenges faced by female counselors, considering gender-specific factors and responsibilities. Understanding the mental health of female HIV counselors is crucial for identifying support needs, enhancing job satisfaction and performance, and developing targeted interventions to promote their well-being. HIV/AIDS counselors are confronted with the unique circumstance of being aware that HIV/AIDS is a protracted and lethal disease taking a heavy mental toll on the patients; also, counseling such patients does have a psychological impact on the counselors themselves.3,4 Despite knowing these potential mental health challenges, they are impelled to continue counseling HIV and AIDS-infected patients, offering emotional and psychological support to them by counseling. The existing literature also highlights the significant psychological challenges faced by HIV counselors worldwide. Research from various regions indicates the high prevalence of emotional burnout, vicarious trauma, and compassion fatigue among counselors.5,6 These difficulties are intensified by the dual roles of counselors as both empathetic listeners and agents of behavior change. Female counselors, in particular, encounter unique obstacles due to societal expectations, gender roles, and the cultural stigmatization associated with discussing sexual health and HIV/AIDS.7,8 Additionally, fear of infection, workload stress, and societal judgment exacerbate the psychological burden for female counselors, especially in low- and middle-income countries. 9 In the context of Kashmir, these challenges are further compounded by societal and cultural factors. Discussing sexual health and HIV/AIDS remains heavily stigmatized, placing significant emotional and social strain on female counselors who are often the main contact for at-risk individuals and people living with HIV (PLHIV). Despite these challenges, there is a notable lack of research on the mental health and lived experiences of female HIV counselors in Kashmir. To our knowledge, no study has specifically explored the psychological well-being of these counselors or the unique challenges they face. This research gap limits our understanding of how cultural and societal dynamics influence their mental health and professional responsibilities. This study seeks to provide insights into their lived experiences, identify their support needs, and suggest targeted interventions to enhance their well-being and job satisfaction.
The very nature of counseling has high potential that counselors become overly engaged with patients, eventually reaching a point where they find it difficult to cope with their psychological issues, sometimes resulting in their decision to leave their jobs. Consequently, this research aims to investigate the psychological challenges that impact counselors during HIV/AIDS counseling sessions, shedding light on the complexities they face in balancing personal mental health concerns with professional responsibilities. With this study, we intended to explore HIV/AIDS counselors’ lived-experience perspectives on the various psychological and emotional challenges faced during the process of counseling an HIV/AIDS patient in the workplace arena. Therefore, this study aimed to address this gap by investigating the psychological and emotional challenges faced by female HIV counselors in Kashmir. By grounding this research in existing global and regional literature, we aim to place their experiences within the broader discourse on the mental health of HIV/AIDS counselors.
Methodology
Interpretative phenomenological analysis (IPA) was used as a qualitative research design for the present study.10,11 According to the IPA methodology,12–14 a representative small, homogeneous sample was taken. Thus, all 11 female HIV counselors in the Kashmir province and one female counselor in Leh (Ladakh UT) participated in the study. The research occurred in the Kashmir valley from December 2022 to January 2023. Ethical approval for the study was granted by the Institutional Review Board (IRB) of the Government Medical College, Srinagar, under reference number IRBGMC/PSM43, dated March 28, 2023.
Participants were selected purposefully adopting purposive sampling based on the inclusion criterion that only those female HIV counselors could participate in the study who are willing to give consent. In-depth interviews were conducted with 12 female HIV counselors from different districts of the Kashmir Valley and Leh (Ladakh UT) at their workplaces, except the interview with the Leh (Ladakh) HIV counselor, which was conducted via a Zoom meeting on December 21, 2022, as the period being winter (Table 1). Due to harsh winter conditions and heavy snowfall, the Srinagar to Ladakh road gets blocked during this period (Table 1). The study focused primarily on female counselors due to their predominance in the region's HIV counseling services, with all integrated counseling and testing centers (ICTC), except one staffed exclusively by female counselors (Table 1). Another key factor was the sensitivity required in counseling HIV-positive patients, which poses unique challenges for female counselors in Kashmir, where discussing sexual health and HIV/AIDS is socially unacceptable. To facilitate the interview, an interview guide focusing on specific areas of interest was created ahead of time, and each interview began with information about educational qualifications and background characteristics (Supplementary file: Annexure I). All interviews were conducted by the female researcher in the English language; however, interviewees were free to speak in English, Urdu, or Kashmiri. The primary researcher, a woman with extensive healthcare research experience and significant involvement in HIV sentinel surveillance and community-based research, had a deep understanding of the professional and gender-related challenges in HIV counseling and conducted the interviews. This background helped the researcher to establish rapport with participants, fostering open dialogue during the interviews. Throughout the research process, the researcher engaged in continuous self-reflection to ensure personal views did not influence the participants’ narratives. Reflexivity was maintained through memo writing by another researcher, who documented reflections during and after each interview to ensure transparency in the analysis.
Profile of female HIV counselors at ICTC centers in Kashmir and Leh (Ladakh UT).

Note: ICTC: Integrated counseling and testing center; SKIMS: Sher-i-Kashmir Institute of Medical Sciences, Soura, the only hospital providing antiretroviral therapy in the Kashmir province, and only this center had both male and female HIV counselors, but the in-depth interview was conducted only with a female HIV counselor; JLNM: Jawahar Lal Nehru Memorial Hospital, District Hospital of Srinagar; LD: Lal Ded, an associated Gynaecology & Obstetrics Hospital of Government Medical College, Srinagar; SMHS: Shri Maharaja Hari Singh Hospital, an associated hospital of GMC Srinagar.
Interviews were audio-recorded after written informed consent, and audio-recorded consent was obtained from the respondents. The interviews started with the introduction of the interviewers, followed by an explanation of the research purpose, method, and content. The interviewer asked questions appropriately according to the interview guide, and another researcher recorded the key points and perceptible changes in the interviewees’ mood and tone during the interview and wrote memos15,16 during the interview process. The researcher responsible for taking memo notes was present during the interviews alongside the interviewer. Furthermore, the interviewer researcher and memo note-taking researcher were also visible during the Zoom interview with one interviewee (female HIV counselor from Leh) to the interviewee. This ensured transparency and reflexivity also allowed for real-time documentation of the discussions.
The interviewees were not interrupted during the interview. The maximum duration of the interview recorded was 1 h and 10 min, while the minimum duration was 35 min. Data saturation was achieved after eight interviews, as recurring themes began to surface. Despite this, in-depth face-to-face interviews continued with all 11 participants to ensure inclusivity and capture a comprehensive range of perspectives from HIV counselors involved in the project. Extending the interviews beyond the initial saturation point was crucial for several reasons. Firstly, it enriched the data, collecting detailed and nuanced insights necessary for an interpretative phenomenological approach. 17 Additionally, it reinforced the consistency of themes across participants, mitigating the risk of premature conclusions and enhancing the reliability of the findings.18,19 This method also allowed for exploring outlier perspectives and subtle variations, which might have been missed, thereby broadening the overall understanding of the phenomenon. 20 Furthermore, involving all participants ensured ethical and methodological rigor by allowing each counselor to share their experiences, thus preventing any potential exclusion. 19 Finally, conducting additional interviews increased the credibility and transferability of the findings by providing a thorough and transparent dataset, adhering to best practices in qualitative research.19,20 This methodological decision was also important for capturing the complete spectrum of lived experiences, thereby enhancing the robustness of the results.
Transcripts were assigned in MS Word files, and data analysis started as a process of carefully scrutinizing data by placing it into inductively created code structures, categories, sub-themes, and themes. The two researchers did the whole process of data analysis. The two researchers well-versed in qualitative data analysis did the whole process of data analysis well-versed in qualitative data analysis. In our analysis, the lead analyst developed a preliminary coding scheme for each set of six interviews. The intercoder agreement was evaluated for every third interview by calculating combined segment-based Kappa scores on two double-coded transcripts. 21 Any coding discrepancies (individual codes with Kappa scores of 0.5 or lower) were addressed through team discussions, the codebook was subsequently updated, and necessary recoding was conducted to ensure consistent code application. 21
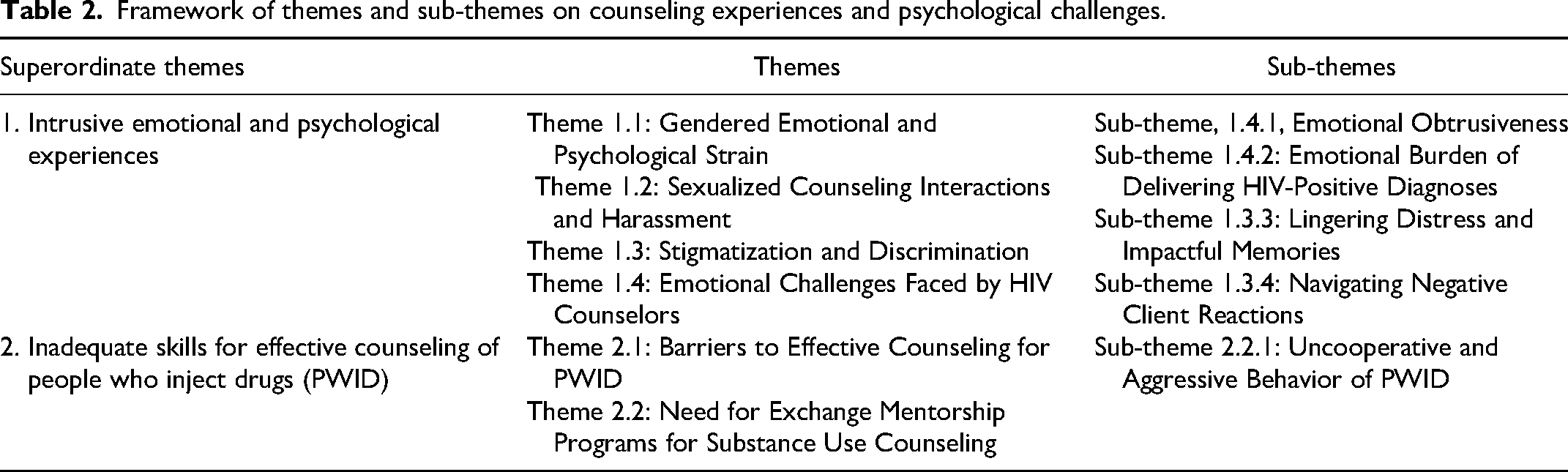
Data were analyzed by adopting an interpretive-phenomenological approach, as outlined by Smith and Osborn, 13 and final codes were organized into sub-themes, themes, and superordinate themes (Table 2). The parenthesis of all superordinate themes along with respondent excerpts was written in detail under each theme heading after an external qualitative research expert reviewed the thematic framework, validating the findings. The reporting of this study conforms to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines 22 (Supplementary file: Annexure II).
Framework of themes and sub-themes on counseling experiences and psychological challenges.
Results
A total of 12 female HIV counselors participated in the study and their profile is given in Table 1. The qualitative data analysis generated two overarching superordinate themes, many themes, and sub-themes (Table 2).
Superordinate Theme 1: Intrusive Emotional and Psychological Experiences
Theme 1.1: Gendered Emotional and Psychological Strain
The respondents described a range of emotional and psychological challenges, particularly stemming from the gendered nature of their roles as female HIV counselors in a culturally sensitive environment. They reported significant emotional distress, including anxiety, fear, and feelings of humiliation, resulting from stigmatizing behaviors by colleagues and clients. These experiences deeply affected their mental health and sense of self-worth.
Verbatim Quotes: … They used to call me ‘HIV (name)’… whenever we moved around, it felt bad, and I remember our colleagues whispering in disdain about us… … My husband told me not to talk about my experiences at home. I told him about one antenatal case that had been positive due to a blood transfusion, but he didn’t accept it (pauses). He believed it was due to immorality and just didn’t listen to me. I just swallowed my tears and got intense repulsion… … A lady from some NGO came to me and started shouting foul language and all my colleagues and peer healthcare professionals heard it. It was extremely nasty and left an ineffaceable impression on my mind… … I was alone that day in my room when one attendant of the client came for a test report too close to me with doubtful intentions. His unsavory advances towards me made me feel psychologically disturbed and dented…
Theme 1.2: Sexualized Counseling Interactions and Harassment
Respondents provided detailed accounts of male clients sexualizing HIV counseling interactions, which caused considerable psychological trauma. The inappropriate and sexualized behavior from male clients often included lewd gestures, intrusive questions, and advances that left the counselors feeling uncomfortable, vulnerable, and unsafe. This type of harassment, experienced during counseling sessions, significantly affected their emotional well-being and professional identity.
Verbatim Quotes: … He even sat unnecessarily close to me and made some lewd gestures. So, I got scared of this guy. I couldn’t even say anything (numbed due to fear) to him then. He asked questions that he should not have asked, he was lewd, and I felt embarrassed. Maybe he had done such things before as well. It is still vividly in my mind, and it doesn’t remain very pleasant… … I remember one episode of Polytechnic College where we had a health camp, and I was there as a female counselor. The male students were deliberately seeking counseling sessions with me and were making dirty hand gestures toward me during the interaction. They were asking for anything indecent, dirty, and unrefined in their minds. The students were asking lame questions with vulgar language, which gave me an extremely unpleasant feeling…
Theme 1.3: Stigmatization and Discrimination
The respondents (80%) gave a recount of experiencing stigmatization and discrimination on different occasions at their workplaces, communities, and homes, which triggered impassioned negativity among them, leading to psycho-emotional purging.
Verbatim Quotes: … Healthcare workers within the hospital have given us the label “HIV-positive person” disparagingly. They do call us by prefixing HIV to our name, like HIV (name) and HIV (name). Even though they are medical professionals, it feels cheap of them… … One day in Kulgam (the place), a boy shouted “AIDS, AIDS” as I passed by on the road. I was unmarried then. I was down awfully and had the creeps. I lowered my gaze and walked through shrunken hearts with a grubby feeling.
Theme:1.4: Emotional Challenges Faced by HIV Counselors
The theme explores the emotional difficulties HIV counselors encounter in their line of work, which is elaborated in the sub-themes. The overarching emotional challenges faced by HIV counselors stem from the weight of disclosing life-altering diagnoses, coping with distressful memories, and managing difficult client reactions. These experiences often leave a profound emotional impact, highlighting the need for support systems and coping mechanisms for counselors as was echoed in their statements.
Sub-theme 1.4.1: Emotional Obtrusiveness
Respondents (80%) shared many narratives, which had clear implications for their inner emotional well-being. They felt emotional obtrusiveness and at times were visibly shaken up.
Verbatim Quotes: …My husband is very strict, and he has an indifferent attitude toward my job; once, when I made a nameplate as an HIV counselor, he asked me to write “ICTC counselor” instead… “I never tell him (my husband) that we have a condom supply or that I distribute them. It's difficult to explain my job profile to my in-laws, too… I was walking in the market for some shopping when I eavesdropped on two women discussing my job in a degrading fashion. They had a very unwelcome and inferior impression of me, and it gave me an unpleasant feeling.
Sub-theme 1.4.2: Emotional Burden of Delivering HIV-Positive Diagnoses
Female HIV Counselors experience significant emotional strain when disclosing HIV-positive results to clients, fearing the reactions and repercussions that follow. This emotional toll is amplified by the need to maintain composure and professionalism. I get palpitations when I have to declare the HIV-positive status of the client; I have to take pauses till the patient understands, and their concerns and queries increase. It's like giving them a death certificate. I even cry at home. I tried politely declaring his HIV-positive result to him, but he shouted at us in rage; we were terrified and felt it was because he was guilty of having contracted HIV through sexual terms in Rajasthan. He wasn't comfortable accepting his HIV-positive result in front of his wife. He hurled abuse at us, kicked furniture, and pushed my laboratory technician, but we didn't give up.
Sub-theme 1.3.3: Lingering Distress and Impactful Memories
Certain cases leave a lasting emotional imprint on counselors, especially when involving families or vulnerable populations. Despite employing coping strategies, such distressful memories continue to affect them deeply.
Verbatim Quotes: “Once, I felt very bad when a couple from Uranhama (place) came out positive, and their 3 kids came out positive as well: one 7-year-old girl, another 4-year-old girl, and a younger daughter also came out positive. That day, I cried and became very emotional. What was their (the kids’) fault if they (the parents) did wrong?” “He was coming, again and again, saying, ‘I am feeling addiction symptoms; what should I do?’ I was scared, and I told him to go to his doctor, a psychiatrist, who can give him medication for these symptoms and will guide him until the test results come in. With IV drug users, the counseling is scary.”
Sub-theme 1.3.4: Navigating Negative Client Reactions
Counselors often face aggressive or resistant behavior from clients who struggle to accept their diagnosis. These situations challenge the counselor's emotional resilience and professional boundaries.
Verbatim Quotes: Once we counseled a lady, she complained to her husband about us scaring her off and discussing immoral things. Later, her husband came and asked us why we had told her about HIV in detail, like its mode of transmission, and how come you are sharing bad stuff that can cause emotional strain. Whenever anyone tests positive, I get so emotional; sometimes I even cry and cry, but somehow, I carry on, as it's my routine now
Superordinate Theme 2: Inadequate Skills for Effective Counseling of People who Inject Drugs (PWID)
Theme 2.1: Barriers to Effective Counseling for PWID
Counseling People Who Inject Drugs (PWID) presents unique challenges that require specific skills, which counselors often find themselves lacking. Barriers to effective counseling, as reported by respondents, include limited training in handling PWID cases, inadequate practical experience, and the psychological strain of managing emotionally charged and sometimes confrontational situations. These barriers often lead counselors to provide only basic education rather than engaging in comprehensive, supportive counseling. The findings reflect counselors’ recognition of these limitations and their desire for further training and skill enhancement.
Verbatim Quotes: Since the establishment of ATF, we have received patients who are advised for screening by a local psychiatrist who comes twice a week… You can never trust a person who injects drugs (PWID). They use inappropriate words that can’t be tolerated, especially around my colleagues. I believe it is very tough to counsel them; we just give them a bit of education… We try to speak to them once they are in their full senses, and we tell them to use oral drugs instead, which might decrease their chances of getting this infection (HIV)… I have seen a PWID patient that was kicking people. What if a female gets injured?
Theme 2.2: Need for Exchange Mentorship Programs for Substance Use Counseling
Respondents highlighted the need for mentorship and exchange programs to enhance their ability to counsel PWID effectively. A significant number (54%) expressed that their current training was insufficient to address the complexities of substance use and mental health counseling. They recommended cross-state exchange programs and collaborations with substance abuse experts to build practical skills and learn advanced counseling techniques. This would allow counselors to better address the intersection of substance use, mental health, and HIV prevention.
Verbatim Quotes: Cross-state programs related to PWID would be of much use. We can learn from Manipur, which ranks first in drug addiction, by participating in an exchange program with counselors from such a place. If they can give us some training or knowledge sharing… The latest counseling methods should be taught, skills and techniques that make work easier and more presentable, the way of putting theory into practice… I think counselors involved in de-addiction centers can share their experiences; we need to get psychiatry counseling and PWID counseling; peer learning and observation can make us more learned and prepared… I believe there should be new training for 2–3 days every year, proper demonstrations should be done, and we should have more access to technology. In a way, we can be more accessible to our patients…
Sub-theme 2.2.1: Uncooperative and Aggressive Behavior of PWID
Female HIV counselors frequently reported challenges in managing uncooperative and aggressive behaviors displayed by PWID during counseling sessions. This behavior, often linked to the psychological and physical effects of substance use, made it difficult for counselors to engage effectively. Respondents shared concerns for their safety during such sessions, particularly when handling highly impulsive or confrontational clients. While these experiences highlight the need for skill-building and safety protocols, counselors also expressed a commitment to improving their capabilities to address the unique needs of PWID.
Verbatim Quotes: I always keep two male technicians with me in the same room before I counsel a PWID case… Sometimes the patient who is high on drugs violates the protocol, and we have to skip the counseling session despite his testing positive for HIV… Since the establishment of ATF, we have received patients who are advised for screening by a local psychiatrist who comes twice a week… Once a PWID was brought to us, about 25 men were not able to control him… How is it possible for a single female counselor to handle such patients? I never do it alone. This is common sense! He was shouting in foul language…
Discussion
The study examined the specific challenges faced by female HIV counselors in Kashmir, a region with distinct socio-cultural norms, significant stigma surrounding HIV/AIDS, and limited mental health resources. Through various dimensions—physical, emotional, psychological, and psychosocial—the research explored their experiences working with people living with HIV (PLHIV), counseling substance users, and managing a complex professional environment. These challenges are shaped by the peculiar socio-cultural context of Kashmir, where traditional gender roles and societal norms significantly influence the work of female counselors.
Challenges in the Cultural Context of Kashmir
In Kashmir, traditional gender roles and societal norms significantly shape the experiences of female counselors. Many participants reported facing judgment and stigma from the community for their work, with HIV counseling perceived as taboo. This societal stigma extends to the workplace, where female counselors encounter biases and discrimination. These findings are consistent with the other studies that have highlighted the additional burden of stigma and limited social support faced by women in health-related fields in culturally conservative settings.23,24
Emotional Exhaustion and the Need for Supportive Supervision
The study revealed that female counselors experience significant emotional exhaustion and burnout, especially when conducting HIV counseling sessions with substance users. In Kashmir, where substance abuse is increasing due to social and political instability, counselors encounter unique challenges requiring specialized training and emotional resilience. Many counselors expressed feeling unprepared to handle confrontational or resistant clients, aligning with findings from other regions facing similar crises.25,26
Lack of Training for Counseling Substance Users
The rising prevalence of substance use in Kashmir adds complexity to the role of HIV counselors. Many participants felt unprepared to address the challenges of counseling people who inject drugs (PWID). This lack of specialized training negatively impacts their professional confidence and the quality of their counseling. Similar findings in previous studies indicate that inadequate training in managing substance use cases significantly affects counseling outcomes. 27
Stigma and Discrimination
Another significant challenge identified was the dual stigma associated with HIV/AIDS and substance use. Female counselors reported experiencing stigma from clients, colleagues, and community members, creating barriers to effective counseling and contributing to emotional distress. These findings are consistent with studies from other conservative societies where stigma against both HIV and substance use is prevalent. 28
Our study identifies several crucial interventions to address the unique challenges faced by female HIV counselors in Kashmir. Firstly, comprehensive training programs are essential, particularly for handling complex cases involving people who inject drugs (PWID). These programs should incorporate evidence-based approaches to counseling substance users and techniques for managing emotional stress. Refresher courses and mentorship programs can further enhance counselors’ confidence and skills. Secondly, establishing regular supervision sessions can provide a platform for counselors to debrief and seek guidance. Structured emotional debriefing has been shown to reduce burnout and improve professional efficacy.29,30 Thirdly, addressing stigma through community awareness campaigns and workplace sensitivity training can help mitigate the stigma associated with HIV counseling, fostering a supportive work environment for female counselors. 30 Incorporating mental health professionals into HIV counseling teams can provide timely support for counselors and clients. Building emotional resilience through mindfulness training and peer support groups can further enhance their well-being.
Strengths of the Study
The use of the interpretive phenomenological approach allowed for a deep and nuanced exploration of the lived experiences of female HIV counselors. This qualitative method facilitated a rich understanding of their challenges from the perspective of the counselors themselves. The study comprehensively examined physical, emotional, psychological, and psychosocial challenges faced by female HIV counselors. This holistic approach contributes to a more complete understanding of the complex factors influencing their professional lives.
The study specifically delved into the challenges encountered by counselors in the context of substance user counseling. This targeted focus provides valuable insights into a critical aspect of HIV counseling that may require specialized attention and training. By focusing on the experiences of counselors in real-world settings, the study enhances the external validity of its findings. The study contributes to the professional development of HIV counselors by highlighting the importance of psychological and emotional well-being, self-regard, and interpersonal relationships. These strengths collectively enhance the credibility and relevance of the study, providing valuable contributions to the understanding of challenges faced by female HIV counselors and potential approaches for improvement in their working conditions to boost their psychological well-being.
Limitations
The study's focus on female HIV counselors of a specific geographic location may limit the generalizability of the findings. Different contexts or cultural settings could influence the experiences and challenges faced by female HIV counselors in unique ways. Moreover, the interpretive phenomenological approach emphasizes depth over breadth; the findings may not be fully generalizable to a broader population of counselors. Also, due to the sensitive nature of the topics discussed, participants may have been inclined to provide socially desirable responses, potentially masking certain principal challenges or experiences. This social desirability bias could influence the accuracy of the reported findings.
Conclusion
The study shows the intricate challenges faced by female HIV counselors in Kashmir, encompassing physical, emotional, psychological, and psychosocial dimensions. The findings emphasize the pivotal role of emotional well-being in effective counseling, with emotional exhaustion and anxiety affecting the quality of counseling provided. The emotional adaptability issues and inefficiencies in addressing substance user counseling further underscore the need for targeted interventions for the psychological well-being of these HIV counselors. Furthermore, the study highlights the impact of emotional exhaustion on counseling abilities, leading to burnout and suboptimal outcomes. The challenges faced by female HIV counselors in Kashmir and Leh (Ladakh), including stigma and discrimination, both in the workplace and communities, add layers of complexity to their psychological health. The findings underscore the urgent need for comprehensive training programs, supportive supervision, and stigma reduction initiatives to enhance the professional efficacy and emotional well-being of these counselors. By integrating mental health support and fostering community awareness, healthcare institutions can better support female counselors, ultimately improving the quality of HIV counseling services. Addressing these challenges is crucial not only for the counselors’ well-being, but also for the broader efforts to combat the HIV/AIDS epidemic in this region.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251321035 - Supplemental material for Psychological and Emotional Challenges Faced by Female HIV Counselors in Kashmir—A Phenomenological Study
Supplemental material, sj-docx-1-jia-10.1177_23259582251321035 for Psychological and Emotional Challenges Faced by Female HIV Counselors in Kashmir—A Phenomenological Study by Khalid Bashir, Inaamul Haq, Mariya Amin Qurieshi and S. Muhammad Salim Khan in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251321035 - Supplemental material for Psychological and Emotional Challenges Faced by Female HIV Counselors in Kashmir—A Phenomenological Study
Supplemental material, sj-docx-2-jia-10.1177_23259582251321035 for Psychological and Emotional Challenges Faced by Female HIV Counselors in Kashmir—A Phenomenological Study by Khalid Bashir, Inaamul Haq, Mariya Amin Qurieshi and S. Muhammad Salim Khan in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We would like to express our gratitude to the National AIDS Control Organization (NACO) and the J&K AIDS Control Society (JKACS) for their contribution and support during the project. We would like to sincerely thank all-female HIV counselors of the Kashmir Valley and female HIV counselors in Leh (Ladakh UT) for their cooperation in sharing quintessential necessary information.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All audio recorded data and verbatim transcripts are in our repository.
Ethical Statement
The ethical approval was obtained from the Institutional Review Board (IRB) Government Medical College, Srinagar, vide letter No. Ref. No: IRBGMC/PSM43, Dated: March 28, 2023.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Our acknowledgment regarding the funding of this project work by the National AIDS Control Organization (NACO/JKACS), without which accomplishment of this project was not possible. Only Rs. 80,000/(eighty thousand rupees) was received for the purpose of data collection and travel data entry (utilization letter no. Spm/1163, dated September 19, 2023).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.