
Abstract
Purpose
Chronic systemic inflammation from human immunodeficiency virus (HIV) may cause metabolic abnormalities in lipid metabolism. Additionally, the development of metabolic syndrome has been associated with specific anti-retroviral therapy, particularly dolutegravir. This study aimed to determine the prevalence and associated factors of metabolic syndrome among people living with HIV on dolutegravir-based anti-retroviral therapy.
Methods
This was an analytical cross-sectional study conducted between October 1, 2022, and March 31, 2023, among 312 people living with HIV. A structured questionnaire was used to collect socio-demographic and clinical characteristics including anthropometric indices and a blood pressure reading. A blood sample was collected to measure plasma glucose levels and serum lipid levels. The outcome being metabolic syndrome, odds ratios were evaluated using logistic regression analysis, and a P-value of <.05 was considered statistically significant.
Results
The prevalence of metabolic syndrome was 42.3%. Waist circumference (73%) and reduced high-density lipoprotein cholesterol (59.9%) were the most prevalent components. Factors associated with metabolic syndrome were patients aged 18–44 years (aOR: 3.10; 95% CI: 1.24–7.79; P = .016), female gender (aOR: 5.40; 95% CI: 2.07–14.13; P = .001), no physical activity (aOR: 4.00; 95% CI: 1.05–15.10; P = .042), and patients who earned >300 000 Tanzanian shillings per month (aOR: 2.15; 95% CI: 1.07–4.32; P = .032).
Conclusion
The prevalence of metabolic syndrome among patients on dolutegravir-based therapy is high. There is a need to adhere to routine screening of metabolic syndrome among people living with HIV on dolutegravir-based anti-retroviral therapy.
Introduction
Metabolic syndrome (MetS) is a form of metabolic deregulation, including insulin resistance, a deranged lipid profile, abdominal obesity, and high blood pressure. 1 Untreated MetS increases the risk of developing cardiovascular and diabetic conditions; thus, it is important to investigate the possible causes and the role played by MetS to reduce the burden of the disease. 2
Human immunodeficiency virus (HIV) itself causes chronic systemic inflammation, which may cause metabolic abnormalities in lipid metabolism and transportation, specifically the elevation of triglycerides and reduced high-density lipoprotein cholesterol (HDL-C), which predisposes them to an elevated risk of acquiring cardiovascular diseases (CVD) compared to the general population.2,3 On the other hand, chronic systemic inflammation may cause hypercoagulability and platelet activation, together leading to endothelial injury. 1 The above-mentioned factors may predispose a patient to have atherosclerosis, hence CVD. Reports have mentioned that MetS predisposes to the development of CVD, estimated at a two-fold increased risk compared to those without MetS. 4
Several studies have shown an increased possibility of MetS with specific anti-retroviral therapy (ART), particularly integrase strand transfer inhibitors (INSTI), as compared with other classes. 5 INSTIs are well tolerated, with higher durability and lower rates of virologic failure. The underlying mechanism causing MetS is not well understood, but there are proposed mechanisms.
Dolutegravir (DTG), one of the drugs in the INSTI class, causes faster viral load suppression, leading to a pronounced return to health changes. As a result, there is exaggerated weight gain as a result of reduced resting energy expenditure. 5 On the other hand, DTG use causes a reduction in adiponectin hormone, which is produced by adipose tissue. Its function is to regulate glucose and lipid metabolism; hence, once adiponectin is reduced, insulin resistance and weight gain occur, leading to MetS. It is pro-adipogenic and pro-lipogenic and also promotes oxidative stress, mitochondrial dysfunction, and insulin resistance. DTG inhibits the binding of radiolabeled alpha-melanocyte-stimulating hormone to the human recombinant melanocortin-4 receptor, which helps in the regulation of energy and food intake. Also, DTG directly interferes with the melanocortin signaling system, causing appetite stimulation, and leading to obesity and MetS. DTG may have an unintended off-target effect by chelating magnesium and manganese, which are required for the process of viral integration. This may later bring about insulin resistance and weight gain, leading to MetS. 5
People living with HIV (PLHIV) have 1.6 times higher odds of having MetS than uninfected individuals. 6 However, it is challenging to determine whether the prevalence of MetS in PLHIV and the general population is comparable given the variations in the definitions of MetS used, 2 as observational studies in Europe and America have yielded estimates ranging from 7% to 52%, while a meta-analysis in Africa reported values ranging from 13% to 58%. 7 The estimated global prevalence of MetS is between 16.7% and 31.3% among PLHIV, 4 with a recent meta-analysis revealing an overall pooled prevalence of 25.3%, 25.6% among PLHIV on ART and 18.5% not on ART. 6
Meta-analyses in sub-Saharan Africa have suggested that MetS may be more prevalent in PLHIV with a prevalence of 21.5%–23.4% in PLHIV compared to 12% in uninfected populations.8,9 Data on the impact of MetS at the regional and national levels is thus required. Even though CVD is disproportionately prevalent in Africa, there is little information on the scope of MetS and its risk factors in sub-Saharan Africa, especially among PLHIV.2,7 Additionally, many ART programs in the region do not routinely address MetS and its components. 10 Reliable epidemiological data on the risk factors for CVD will be necessary for programs to successfully reduce the growing CVD burden among PLHIV. Moreover, INSTIs are highly effective, with favorable outcomes in viral load suppression and a high genetic barrier to drug resistance. Therefore, it has become an integral part of ART worldwide. 11
In Tanzania, DTG is the preferred drug in formulating the default first-line ART regimen. 12 However, there is a growing concern about metabolic deregulation, including dyslipidemia, weight gain, and elevated blood glucose associated with DTG. 13 This study aimed to evaluate the prevalence of MetS and its associated factors among PLHIV receiving DTG-based ART at Kilimanjaro Christian Medical Centre (KCMC).
Materials and Methods
Study Design and Setting
This was an analytical cross-sectional study conducted among PLHIV aged 18 years and above who were on DTG-based ART attending the care and treatment clinic (CTC) at KCMC from October 1, 2022 to March 31, 2023, to determine the prevalence of MetS and its associated factors. The number of PLHIV currently on treatment at CTC was 2,649, with two distinct clinics operating thrice a week to accommodate PLHIV in the region. To not overburden the clinics, patients with undetectable viral load were given intervals of three months, while those with ≥1000 copies/ml were since every month. The study included PLHIV who were 18 years of age and above on DTG-based ART for at least 6 months, ensuring coverage of a maximum number of patients in the study. Pregnant women, PLHIV with opportunistic infections (such as tuberculosis), and patients on psychotropic drugs and immunosuppressants were excluded from the study.
Operational Definitions
According to the International Diabetes Federation criteria, MetS was assessed using waist circumference (WC) (≥94 cm for men or ≥80 cm for women), triglycerides (≥1.7 mmol/L or specific treatment for this abnormality), HDL-C (≤1 mmol/L for men or ≤1.3 mmol/L for women or specific treatment for this abnormality), elevated blood pressure (BP) ≥ 130/85 mm Hg or treatment of previously diagnosed hypertension), and elevated fasting blood glucose (FBG) ≥ 5.6 mmol/L or treatment of previously diagnosed diabetes mellitus. 14
Sample Size Estimation
A minimum sample size for this study was estimated based on a study done in Tanzania looking at the prevalence of MetS among PLHIV. 10 Therefore, a hypothetical proportion of 25.6% was used to estimate the sample size using the formula n = Z2P(1−P)/d2. The estimated minimum sample size calculated was 297. Purposive sampling was used as enrolled PLHIV were only those who had not eaten (fasted) within the past 8 h before enrollment and sample collection. A total of 358 PLHIV on DTG-based ART met the criteria for being recruited in the study from October 1, 2022 to March 31, 2023. A total of 46 were excluded from the study because they had incomplete investigations due to either hemolyzed blood samples, insufficient blood samples or no blood samples received, as only 312 PLHIV on DTG-based ART (87.2%) were enrolled in this study.
Data Collection and Procedure
On each clinic day, all eligible patients who attended CTC at KCMC during the study period were informed about the study and asked for their consent to participate in the study. Those who met the eligibility criteria and consented to participate in the study were enrolled.
The outcome was MetS, and the independent variables included age, gender, marital status, education level, work status, marital status, income, anthropometric characteristics, which include height, weight, and WC, and behavior factors such as alcohol use, cigarette smoking, and physical activity, which were collected using the World Health Organization (WHO) stepwise approach. 15 Other independent variables, such as age, which was categorized according to WHO under the United Nations 2015, were 18–44 as young age, 44–60 as middle age, and 60 and above as old age. 16
Clinical variables included the duration since HIV diagnosis, and viral load suppression, where undetectable viral load was ≤50 copies/ml or detectable viral load was >50 copies/ml, 17 which was tested by Cobas 4800 (Roche Diagnostics Ltd, CH-6343 Rotkreuz, Switzerland), duration on the DTG-based ART regimen, comorbidities, current and previous ART regimes, BP, and body mass index (BMI) on the enrollment day. Laboratory investigations included FBG, glycated hemoglobin (HbA1c), lipid profiles, including total cholesterol, low-density lipoprotein cholesterol (LDL-C), HDL-C, and triglycerides.
Data collection tools included a BP machine (Omron), a glucometer (Glucoplus), a weighing scale, a tape measure, a structured questionnaire, and a CTC information card. After receiving written informed consent, a structured questionnaire with open- and closed-ended questions using REDCap was filled out. Blood pressure was measured as the average of the last two of three measurements, taken at intervals of at least five minutes after the patient had been seated for five minutes. Anthropometric measurements of WC were taken with a flexible inelastic tape placed on the midpoint between the lower rib margin and the iliac crest in a perpendicular plane to the long axis of the body, as described in WHO guidelines. 15 Height was determined without shoes using a stadiometer. Weight was measured using a weighing scale, and patients were fully dressed without heavy clothing or shoes. Physical activity was categorized into vigorous-intensity activity and moderate-intensity activity, this was looked at during working or sports activities. 10
Blood samples were then taken, and vacutainer tubes were clearly labeled and packaged in a cooler box for transportation to the laboratory for analysis. The collected samples for FBG (mmol/L), HBA1c (%) were about 2 cc of blood, LDL-C (mmol/L), HDL-C (mmol/L), triglycerides (mmol/L), and total cholesterol (mmol/L) were about 2 cc of blood in a lithium heparin tube. Glucoplus (Glucoplus Inc., Saint Laurent, QC H4S 1S3, Canada) glucometer was used for the assessment of the patient's FBG. The pre-analysis phase of the lithium heparin tube sample involved centrifuging samples for 10 min at 10 000 relative centrifugal forces. Thereafter, the lipid tests were analyzed using a Cobas Integra 400 Plus (Roche Diagnostics Ltd, CH-6343 Rotkreuz, Switzerland). All patients were provided with feedback on their results and advised accordingly. Data was cross-checked before finalizing the structured questionnaire. Confidentiality was observed, and all data were stored unlinked to patient identifiers.
Statistical Analysis
The obtained data were organized into a suitable format to enter into Statistical Package for the Social Sciences version 26 for analysis. Quantitative data from questionnaires was analyzed using descriptive and inferential analysis. Frequency and proportion were used to summarize the categorical variables and the mean for numerical data. A chi-square statistic was used to associate DTG and MetS among PLHIV. Logistic bivariate and multivariate analyses were used to obtain odds ratios and adjusted odds ratios to determine the associated factors for MetS among PLHIV on DTG-based ART attending CTC at KCMC. Associated factors with a P-value of <.05 were used to declare statistical significance.
Results
Socio-Demographic and Clinical Characteristics of PLHIV on DTG-Based ART
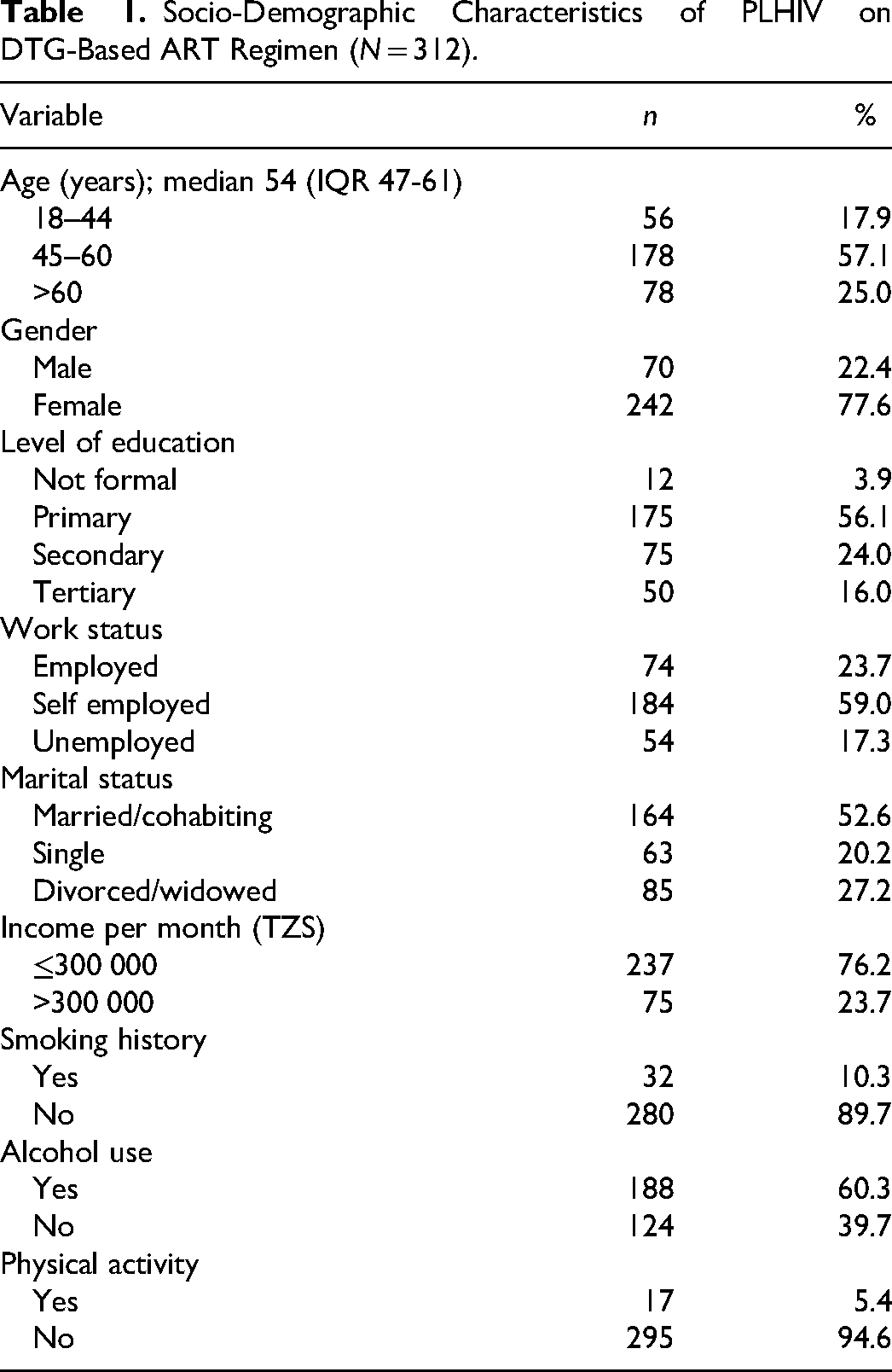
As summarized in Table 1, 77.6% were female, and more than half of patients (57.1%) were aged between 45–60 years, with a median age of 54 (IQR: 54–61) years. Those who had primary school education were 56.1%, and 52.6% were married or cohabiting. More than two-thirds (76.2%) had a monthly income of ≤300 000 Tanzanian shillings, of which 59.0% were self-employed. Thirty-two (10.3%) patients had a history of cigarette smoking, and out of them, 46.8% were current smokers. Those with a history of alcohol consumption were 60.3%, and 34.9% of the patients were drinking alcohol 1–4 times per week. The majority (94.6%) were not involved in vigorous-intensity physical activity.
Socio-Demographic Characteristics of PLHIV on DTG-Based ART Regimen (N = 312).
The median duration since HIV diagnosis was 13 (IQR: 8-17) years, and more than half (59.6%) of the patients were in WHO HIV disease clinical stage III or IV. The majority (88.8%) of patients had an undetectable viral load, and more than half (53.5%) were on a combination of Tenofovir (TDF), Lamivudine, and Efavirenz (EFV) before being on a DTG-based ART regimen. At the time of initiation of DTG-based ART, 57.7% had an elevated BMI. However, after being on DTG for at least 6 months, 71.8% of the patients had an elevated BMI. More than half (63.1%) of the patients had elevated HbA1c, 27.9% had elevated LDL-C, and 29.9% had elevated total cholesterol (Table 2).
Clinical and Drug-Related Characteristics of PLHIV on DTG-Based ART (N = 312).
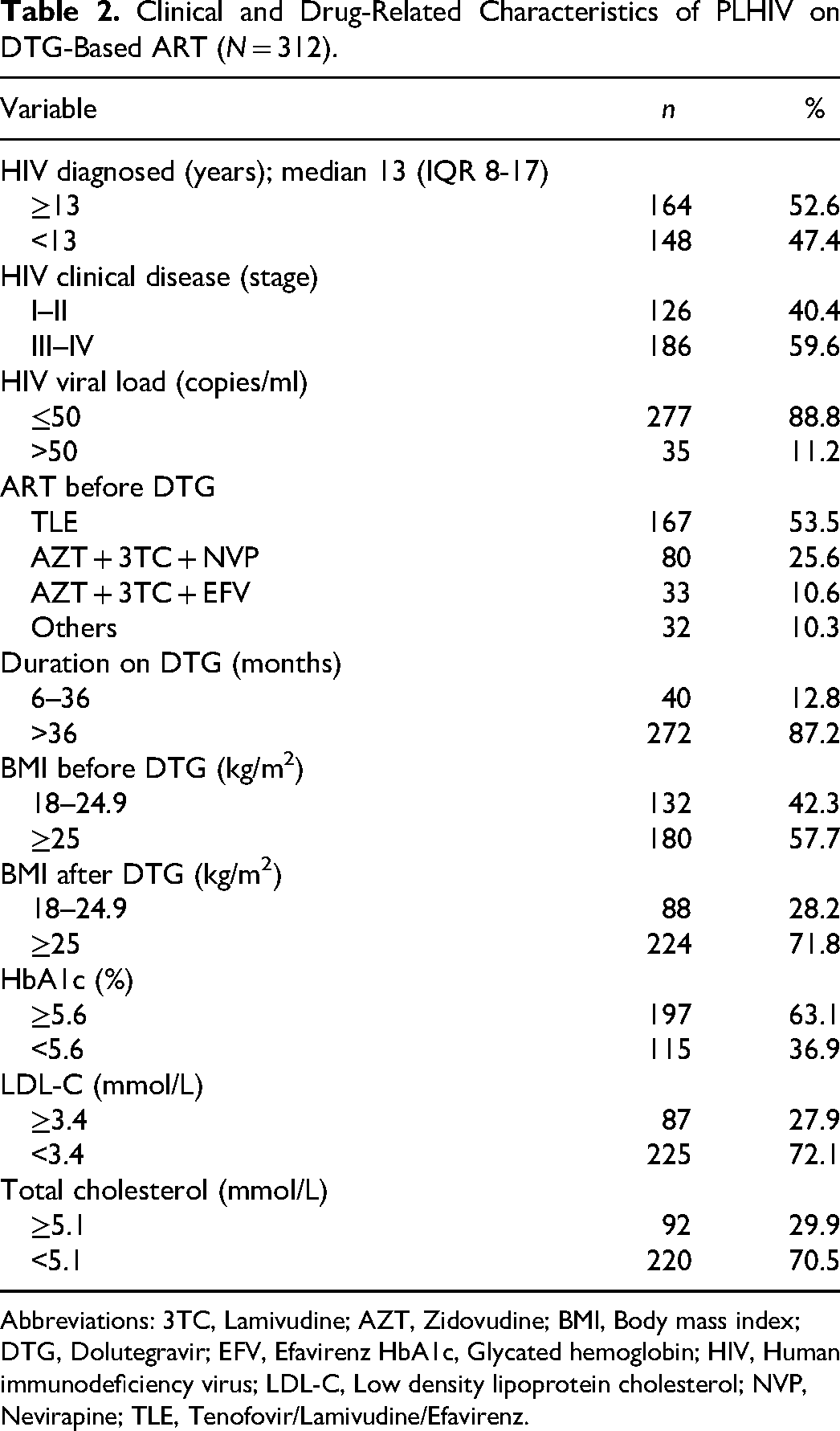
Abbreviations: 3TC, Lamivudine; AZT, Zidovudine; BMI, Body mass index; DTG, Dolutegravir; EFV, Efavirenz HbA1c, Glycated hemoglobin; HIV, Human immunodeficiency virus; LDL-C, Low density lipoprotein cholesterol; NVP, Nevirapine; TLE, Tenofovir/Lamivudine/Efavirenz.
Prevalence of MetS among PLHIV on DTG-Based ART
The overall prevalence of MetS was 42.3%. The most common components of MetS in all patients were elevated WC (73.1%) and low HDL-C (59.9%), followed by elevated BP (36.2%), TG (29.5%), and FBG (24.7%). MetS was more prevalent in the age group >60 years (48.7%), among females (48.3%), among those who were divorced or widowed (54.1%), and among those with physical inactivity (43.7%). MetS was more prevalent among those diagnosed with HIV for ≥13 years (47.6%), with a longer duration of DTG use of ≥36 months (45.6%) (Table 3).
Univariate and Multivariate Logistic Regression for Factors Associated with Metabolic Syndrome (N = 312).
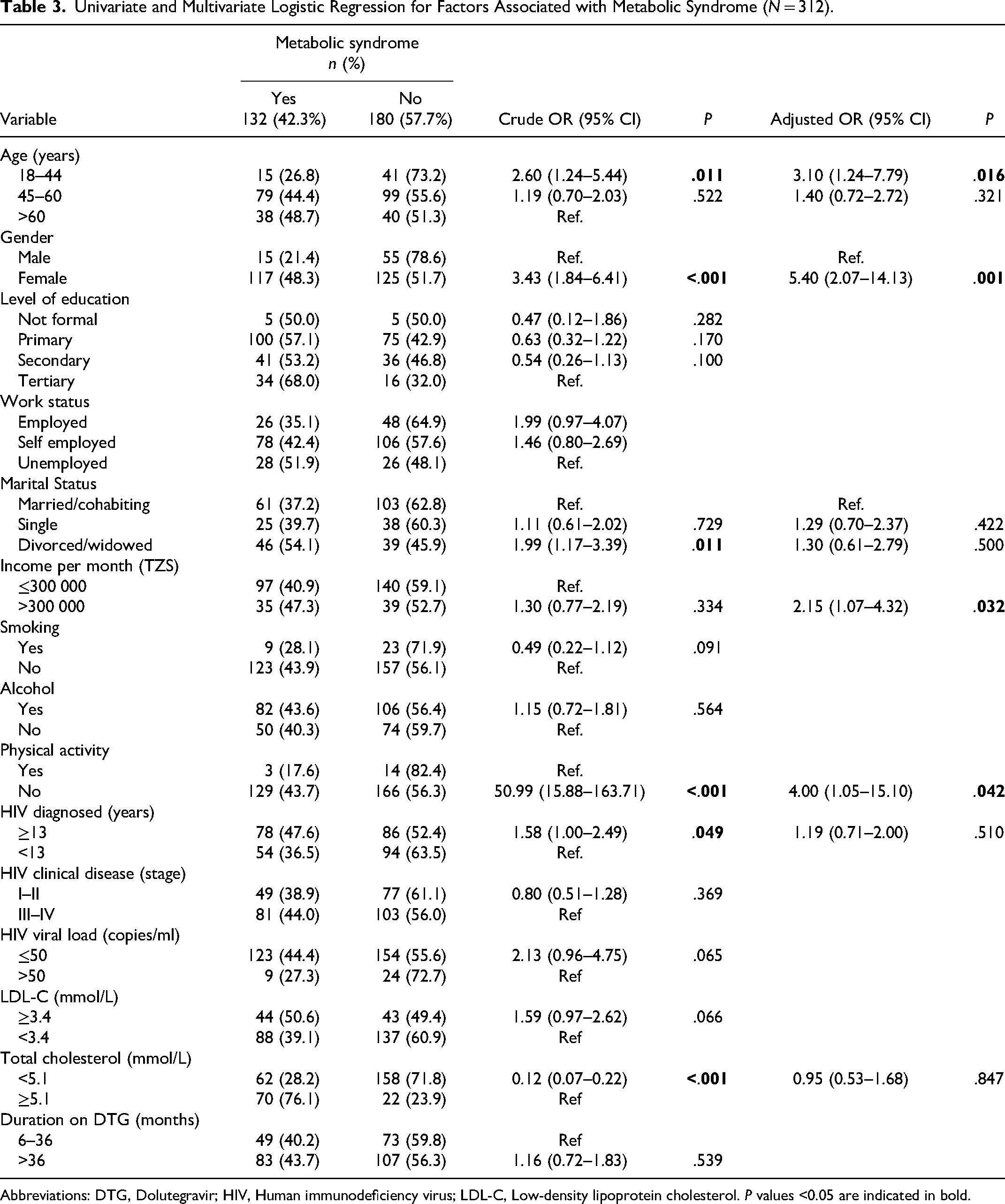
Abbreviations: DTG, Dolutegravir; HIV, Human immunodeficiency virus; LDL-C, Low-density lipoprotein cholesterol. P values <0.05 are indicated in bold.
Factors Associated with MetS among PLHIV on DTG-Based ART
In the multivariate analysis, patients aged 18-44 years (aOR: 3.10; 95% CI: 1.24-7.79; P = .016), females (aOR: 5.40; 95% CI: 2.07-14.13; P = .001), no physical activity (aOR: 4.00; 95% CI = 1.05-15.10; P = .042), and patients who earned >300 000 Tanzanian shillings per month (aOR: 2.15 95% CI: 1.07-4.32; P = .032), were predictors for MetS among PLHIV (Table 3).
Discussion
In this study, the majority of the patients were females, and the age group 45-60 years, which corresponds to the higher HIV prevalence in females and within the age group with the highest HIV prevalence in Tanzania. 18 The prevalence of MetS was 42.3%. The high prevalence could be attributed to several factors, such as the MetS criteria used, which have been shown to increase the ability to identify patients with MetS. 19 Moreover, the study included PLHIV on DTG, which has been shown to increase the likelihood of developing MetS. 13
Similar findings were observed in hospital-based cross-sectional studies done in Nigeria and Malaysia, where the prevalence of MetS among PLHIV on ART was 50.3% and 43.4%, respectively, 20 despite both studies using different criteria. Although the study done in Ethiopia used the Joint Interim Statement MetS criteria, the reported MetS among PLHIV on ART was low at 27.9%. 1 The observed difference could be due to differences in the ART studied, diet, lifestyle, genetics, environmental factors, and cultural work-related activities. Furthermore, the study done in Dar es Salaam, Tanzania, had different findings, where the prevalence of MetS among PLHIV on ART was 25.6%. 10 The possible reasons for different findings include the difference in the study population, as the other study enrolled patients from two different regions involving urban and rural areas, but also the difference in ART used, as none of the patients in the previous study were on INSTI-based ART. Also, the MetS criteria for diagnosis were different. 10
In Sub-Saharan Africa, two randomized controlled trials (the NAMSAL 21 and ADVANCE 22 trials) compared DTG- and EFV-based ART in ART-naïve PLHIV. Patients being randomized to either DTG- or EFV-based ART found that those in the DTG arm gained more weight than those on EFV. A retrospective cohort in Ethiopia showed that patients on a DTG-based ART had a mean weight gain of 3.8 kg in 1 year compared to those on EFV-based ART (2.3 kg). Proposed mechanisms of DTG-associated weight gain include a decrease in energy expenditure following rapid reduction of viral load, 23 or there may be impaired appetite regulation in the central nervous system, particularly the melanocortin-4 receptor, which regulates caloric intake through modulating leptin signaling and affects energy homeostasis and appetite regulation. 24
However, the study observed that the proportion of PLHIV with a high BMI increased from 57.7% before the initiation of the DTG-based ART regimen to 71.8% after at least 6 months of using the DTG-based ART regimen. This may be explained by the association between DTG use and increased body fat with subsequent weight gain due to interference with lipid, glucose, and adipose tissue metabolism, hence the predisposition to MetS. 25 These patients were on DTG-based ART, which increased the likelihood of having increased weight. 26 Similarly, the study done in Zambia, which included patients on DTG-based ART, showed individuals with MetS (using criteria other than BMI) had a significantly higher BMI. 2 However, the baseline BMI before initiation of the DTG-based regimen was not an independent factor associated with MetS in our study.
In the current study, WC was the leading component of MetS, followed by reduced HDL-C (60%). The study in Nigeria had similar findings of reduced HDL-C and WC, with a prevalence of 68% and 50%, respectively. 20 The study done in Zambia had similar findings, where WC was the most prevalent component of MetS (76.8%), followed by reduced HDL-C (69.3%). 2 WC was the leading component because most of the patients were females, and increased WC is the leading component among females. 15 Reduced HDL-C was the second leading component because HIV infection itself causes a reduction in HDL-C; this appears to be the first change after acquiring the infection. 27 DTG causes changes in the structure of fat cells that may promote insulin resistance and has been linked to increased production of collagen types linked to adipocyte fibrosis and obesity. In adipocytes, cells exposed to DTG have higher levels of lipid accumulation, lower levels of leptin and adiponectin, and a lower uptake of glucose compared to control samples in-vitro studies. Additionally, DTG also promotes lipid accumulation when added to already-differentiated mature adipocytes. This suggests that DTG enhances adipogenesis and lipogenesis in differentiated adipose stem cells and mature adipocytes. 28
In addition to WC and reduced HDL-C levels, almost two-thirds of the patients had abnormal HbA1c in this study. This may be explained by the use of DTG, which has been associated with poor glycemic control. 25 In the longitudinal cohort study done in the USA, patients who were switched to INSTIs had an increased likelihood of developing elevated HbA1c (P = .03). 13 A study done in Uganda had similar findings, where patients on INSTIs had poor glycemic control. 26
In this study, patients aged 18–44 years had 3.10 higher odds of having MetS. This may be different because other studies show older age is generally associated with MetS, as shown in the study done in Zambia among PLHIV on ART. This study reported an increase in age by 1 year to have 7% increased odds of acquiring MetS. 2 Additionally, in the previous study done in Tanzania, patients aged ≥40 years had 2.71 times higher odds of having MetS. It may be possible that in this study, patients aged ≥40 years likely influenced the age group. In Ethiopia, patients aged >40 years were significantly associated with MetS. 1 However, there is a difference in the age categories and MetS criteria used in these studies, because with aging, there is a decrease in physical activity and metabolism.26,29
Females were strongly associated with MetS, with 5.40 higher odds of having MetS. In the African Cohort Study, women had a greater weight gain one year post DTG-based ART switch, but this difference was not significant after the first year. 30 Similarly, in the ADVANCE trial, women on DTG-based ART gained more weight than men. 22 This could be because females take sedentary work with low physical demand; on the other hand, females embrace weight gain as a sign of prosperity to avoid being stigmatized. 26 Genetic and hormonal factors, history of previous pregnancy, and oral contraceptive use could contribute to these findings; however, these were not among the variables studied.
This study identified that patients who did not partake in vigorous-intensity physical activity had 4.00 higher odds of having MetS. Patients who had some sort of weekly physical activity showed significantly lower levels of fasting glucose, HDL-C, and WC as components of MetS compared with patients who did not participate in any physical activity. 31 Notably, patients who were earning >300 000 Tanzanian shillings per month were 2.15 times more likely to have MetS. This denotes the difference in the quality of life for patients who are earning better, as they can live a lavish lifestyle, leading to factors that increase the chances of MetS.
Existing studies have estimated the weight gain on TDF- and EFV-based ART to range between 2–3 kg over 96 weeks. In sub-Saharan Africa, studies have confirmed obesity as a determinant of hypertension in PLHIV, with the incidence of hypertension ranging from 5.4 to 16.0 per 100 patient-years. 32 In addition to MetS increasing CVD risk, studies have noted that patients on TDF-based ART have an increased risk of hypertension. In the RESPOND cohort, the use of TDF- and DTG-based ART was associated with incident hypertension and dyslipidemia, suggesting the need for screening in PLHIV as the burden of CVD risk is growing. 33 There may be a need to combat the growing CVD risk in the near future, as a cohort showed that treatment with semaglutide was associated with an average weight loss of 6.5 kg and HbA1c reduction of 1.07% at one year in PLHIV. 34 Future studies may implore the use of semaglutide to counter the weight effect of DTG-based ART among PLHIV, especially in sub-Saharan Africa where there is limited access, the cost is substantial, and these medications can be manufactured and sold profitably at low costs. 35
The limitations of this study were that it was a single-center hospital-based study, which may not be representative of the burden and characteristics of MetS in PLHIV in the whole population. Although the study investigated MetS after 6 months of DTG-based ART use, it could not elicit MetS before initiation of DTG-based ART. Genetic and hormonal factors, diet, history of previous pregnancy, oral contraceptive use, and psychological implications of DTG-based ART were not assessed in association with MetS.
Conclusion
MetS is common among PLHIV on DTG-based ART. WC, reduced HDL-C, and high BP, as components of the five MetS criteria, were more prevalent in our study population. The study revealed that younger age, females, no physical activity, and better income earners were associated with MetS among PLHIV on DTG-based ART at KCMC. Protocols should be in place for routine screening and subsequent management of MetS among PLHIV on DTG-based ART regimens, as more focus should be given to PLHIV in the middle ages, females, those with no physical activity, and better income earners. The implementation of integrated care for PLHIV and non-communicable diseases is essential for addressing the high burden of MetS in PLHIV. Also, there is a need for more robust study designs, such as longitudinal studies to assess MetS as patients start DTG-based ART and observe for metabolic-related outcomes among PLHIV in this setting.
Footnotes
Authors’ Contributions
TEM, KGK, AMS, EWM, ERS, GBN, HFA, VRK, NGC, and FSL conceptualized the manuscript; TEM, IAIM, NJ, AAM, SKG, and ARC were involved with data collection; TEM, AMS, and JSN were involved with data analysis; TEM wrote the first draft; all authors reviewed drafts and provided substantial edits; all authors read and approved the final version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
The study obtained the approval of the Research and Ethics Committee of Kilimanjaro Christian Medical University College (No. PG 114/2022). Written consent was obtained from the patients after being informed of the purpose and benefits of the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The corresponding author received funding from the Minneapolis Heart Institute Foundation.