
Abstract
In 2022, a community-academic collaborative team published 5 key recommendations for developing a national action plan to advance the sexual and reproductive health and rights (SRHR) of women living with HIV in Canada. In 2023, a national gathering was convened to strategize implementation of the recommendations across policy, practice, and research settings. Discussions highlighted that meaningful engagement of women living with HIV (recommendation 1) is foundational to implementing the other recommendations. Meaningful engagement requires SRHR stakeholders to: actively dismantle power differentials; commit to engagement as an ongoing process; learn about regionally specific epidemiology and sociostructural forces that create and sustain vulnerability for HIV among women; invest in creating supportive infrastructure; and integrate Equity, Diversity, and Inclusion principles to call diverse groups into the conversation. This Canadian initiative demonstrates how global guidelines can be transformed into nationally tailored action plans to advance the SRHR of women living with HIV, grounded in meaningful engagement.
Plain Language Summary
In 2022, a Canadian team of women living with HIV, researchers, community advocates, global program managers and policymakers, clinicians, and social service providers developed five key recommendations for a national action plan to advance the sexual and reproductive health and rights of women living with HIV. To ensure that this national action plan impacts practice, the team organized a community gathering to discuss implementation. Discussions highlighted that meaningful engagement of women living with HIV (recommendation 1) is foundational to implementing the other recommendations. Meaningful engagement is understood as involvement that goes beyond participation, where community members have real impact and decision-making power on the work. The attendees identified specific elements of meaningful engagement of women living with HIV for those working in sexual and reproductive health and rights: (1) Acknowledge and actively dismantle power differentials; (2) Commit to meaningful engagement as an on-going process; (3) Learn about how HIV impacts women in your region and what factors contribute to women being at risk of getting HIV; (4) Spend time and money to create supportive systems, clear policies, and leadership (5) Integrate Equity, Diversity, and Inclusion principles to ensure that diverse groups, voices, and priorities are called into the conversation This Canadian initiative is an example of how global guidelines can be transformed into nationallytailored action plans to advance the sexual and reproductive health and rights of women living with HIV, grounded in meaningful engagement.
Keywords
Introduction
In 2017 the World Health Organization (WHO) published the Consolidated guideline on sexual and reproductive health and rights of women living with HIV. 1 This guideline, created in collaboration with women living with HIV globally, 2 summarizes the multiple influences that impact women living with HIV's access to health and healthcare, including individual, relationship, community, and societal factors. Recognizing these varying influences, the guidelines and a subsequent implementation checklist 3 focus on advancing the sexual and reproductive health and rights (SRHR) of women living with HIV through creating enabling environments—which centers efforts to address environmental and systemic barriers rather than individual behaviors. This approach is aligned with the reality that progress towards SRHR for all requires a holistic and comprehensive approach that grapples with the social, legal, and economic environments that create barriers to wellbeing. 4
The Consolidated guideline is particularly relevant in Canada where women comprise approximately one-quarter of all people living with HIV 5 and 25.2% of all incident HIV diagnoses. 6 Canada has made fair progress toward the 90-90-90 global HIV targets, achieving both the first goal with 90% of people living with HIV diagnosed and the third goal with 95% of those on treatment virally suppressed, while being just short of the second goal with 87% of those diagnosed on treatment. 7 National data in Canada is only disaggregated by sex and not by gender, however, the sex-disaggregated data shows that the percentage of females at each stage of the HIV care continuum (88% diagnosed, 85% on treatment, and 90% suppressed) lags behind the percentage of males (90% diagnosed, 87% on treatment, and 96% virally suppressed). 7 Data from a national cohort study of women living with HIV also indicates that trans women have lower rates of antiretroviral treatment (67%) 8 compared to estimates in the total population of people living with HIV (87%). 7 Together, these data indicate that women living with HIV in Canada have less access to timely HIV diagnosis, antiretroviral treatment, and viral suppression. Women living with HIV in Canada are advocating for their SRHR, as HIV-related stigma and gender-related norms of womanhood act as barriers to safely navigating sexual relationships, fulfilling sexual rights, 9 accessing comprehensive medical and social care,10,11 and attaining rights to reproductive autonomy. 12
The experiences of women living with HIV in Canada, including prevalence, incidence, and stigma, are shaped by intersecting inequities along social axes, including Indigenous ancestry, African, Caribbean, or Black (ACB) ethnicity, poverty, incarceration experience, injection drug use, sex work history, refugee and newcomer status, rural location, transgender identity, and gay, bisexual, Two-Spirit, or queer sexual identity.6,13–15 Given Canada's colonial roots, Indigenous women's experiences of HIV especially must be understood in the context of historical and ongoing colonial legacies that have stigmatized and attempted to erase Indigenous peoples’ languages, cultures, and identities.16,17 The resulting environment of racism, sexism, and stigma creates additional barriers for Indigenous women living with HIV to fully realize their SRHR that can only be addressed with Indigenous leadership.
Despite the fact that there are over 15 000 women living with HIV in Canada, 7 prior to the Consolidated guideline disproportionately little HIV care, research, and community services in Canada focused specifically on women.1,18,19 To develop strategies to implement the Consolidated guideline and drive development of women-centered programming and research, a team of women living with HIV, researchers, community advocates, global programming and policymakers, and clinical and social care providers came together to develop a national action plan to advance the SRHR of women living with HIV in Canada. Details of this process, beginning in 2017, have been previously described.20,21 In brief, this process involved co-hosting a national webinar series with the WHO on best practice and examples of the Consolidated guidelines within a Canadian context across 4 community-identified priority topics: (1) Trauma- and Violence-Aware Care/Practice (TVAC/TVAP); (2) Supporting Safer HIV Disclosure; (3) Reproductive Health, Rights, and Justice; and (4) Resilience, Self-efficacy, and Peer Support. 20 National stakeholders and WHO representatives convened in person at the annual Canadian Association for HIV Research (CAHR) conference in April 2018 to develop a national action plan. Data from the event discussions and from a linked online survey were analyzed and refined to identify 5 key recommendations for developing a national action plan to advance the SRHR of women a living with HIV in Canada (shown in Figure 1). After stakeholder validation, the planning process, a description of the 5 key recommendations, and examples of best implementation practices in Canada were published in Women's Health. 20 The key recommendations presented in the national action plan have alignment with strategies outlined to achieve SRHR by a global team of women living with HIV. 22

The 5 key recommendations for a national action plan to advance the sexual and reproductive health and rights of women living with HIV in Canada. 20 (1) Meaningfully engage women living with HIV across research, policy, and practice aimed at advancing the sexual and reproductive health and rights by, with, and for all women living with HIV. (2) Centre Indigenous Women's priorities, voices, and perspectives in all efforts to advance sexual and reproductive health and rights of women living with HIV. (3) Use language and terminologies that are actively destigmatizing, inclusive, and reflective of women living with HIV's strengths and experience when discussing sexual and reproductive health and the rights of women living with HIV. (4) Strengthen and expand Knowledge Translation initiatives to support access to and uptake of relevant and contemporary sexual and reproductive health and rights information for all stakeholders. (5) Catalyze the reciprocal relationship between evidence and action such that action on sexual and reproductive health and rights is guided by research evidence, and research is guided by what is needed for effective action.
Further national stakeholder dialogues were held to discuss how to increase the visibility, support uptake, and advance implementation of the key recommendations. Several strategies emerged, including creating and promoting an endorsement pledge that individuals and organizations could sign to indicate their support of and commitment to the recommendations and the SRHR of women living with HIV in Canada. The pledge reads: “We are committed to the ongoing involvement of women living with HIV in the work we do and the services we provide. We commit to implementing the 5 key recommendations to advance the sexual and reproductive health and rights of women living with HIV.” The endorsement campaign was distributed starting in December 2022 via email to a nation-wide stakeholder list, social media posts, and word-of-mouth. The stakeholder list included researchers, community-based service organizations (CBOs, including AIDS Service Organizations, harm reduction and sexual health centers, and women's and family services, and Indigenous health-specific organizations), HIV clinicians and other medical practitioners, with contacts in all provinces and the Yukon. The campaign not only helped increase awareness of the key recommendations and provide supportive resources to those working towards implementation, but also served as an important advocacy tool to demonstrate to policymakers and funders that the distinct SRHR rights of women living with HIV are an important priority in delivering funding and developing initiatives.
While this campaign is a useful advocacy and knowledge sharing tool, the core team recognized that a signature campaign without support for implementation would fall short in tangibly advancing the SRHR of women living with HIV in Canada. Thus, the team convened another community gathering to co-produce an implementation strategy across diverse settings. Hosting a preconference ancillary event at the 32nd Canadian Conference on HIV/AIDS Research (CAHR 2023) offered a venue to bring together leaders in HIV across Canada in-person for this discussion.
The objectives of this article are to (1) describe and share our findings from the in-person community gathering at CAHR 2023 and (2) present principles for implementing the 5 key recommendations to advance the SRHR of women living with HIV across settings, focusing on meaningful engagement.
Methods
The CAHR 2023 Community Gathering
Our community-academic collaborative team hosted an in-person and online preconference meeting at CAHR 2023 entitled “Implementing the Key Recommendations to Advance the Sexual and Reproductive Health and Rights of Women Living with HIV across Policy, Practice, and Research.” The purpose of the meeting was to generate strategies for implementing the 5 key recommendations across diverse settings.
A broad invitation to register for the event was sent out over social media, through CAHR platforms, and direct email invitations to those who had already signed the endorsement and other past collaborators. Representatives from the Federal Initiative to Address HIV/AIDS in Canada were also directly invited to attend.
On April 27, 2023, key stakeholders convened for the event (agenda included in Supplemental material). There were 42 attendees in-person and 4 who joined virtually. There was representation from diverse geographic areas across Canada, including attendees from BC, Alberta, Manitoba, Ontario, Quebec, and Nova Scotia. A diversity of voices was included in this conversation, including women living with HIV, clinicians, researchers, social service providers, policy analysts, funders, and representation from the Canadian Institutes of Health Research (CIHR) HIV/AIDS and STBBI Research Initiative, leading to a rich and productive discussion.
Opening remarks highlighted the importance of centering women living with HIV in this work, provided important background information on the WHO Consolidated guideline, and described Canada's leadership in developing a national action plan to advance the SRHR of women living with HIV. The foundational background knowledge of the opening panel ensured that all attendees understood the history and intent of the key recommendations, preparing them for discussion on implementation. The next section of the program was a facilitated panel discussion that explored how the key recommendations can be implemented across diverse settings, particularly those that are not women-specific services. The 3 panelists represented perspectives from a woman living with HIV, a researcher, and a clinician. Their discussion emphasized that women-centered HIV care means doing person-centered work, understanding womanhood as one piece of a person's identity within the context of her life and all the intersectional identities she holds (eg, family, career, and culture). This is consistent with descriptions of women-centered care from women living with HIV, who have emphasized the importance of a “whole person” conceptualization.21,23
The panel discussion set the stage for small group discussions, providing ideas for deeper discussion around implementation during the smaller groups. Each of the 5 small groups focused on 1 of 3 settings (AIDS Service Organization, clinical, or research) to discuss the 2 questions: (1) How can we implement the 5 key recommendations in our setting? and (2) How can we create an accountability plan to ensure ongoing commitment to the SRHR of the diversity of women living with HIV across Canada? Groups were facilitated in English and French. Notetakers captured key points and provided materials to topic co-leads for review, validation, and synthesis. Co-leads and notetakers summarized and presented their discussions for a large group report-back at the end of the session.
Analysis
All notes were consolidated by the coordinating team and organized by recommendation and location. The priority in the analysis was to highlight the actionable, practical steps for advancing the key recommendations outlined through the facilitated panel, the small group discussions, and the large group report-back.
Findings
Discussion throughout the event revealed that understanding and implementing recommendation 1 “Meaningfully engage women living with HIV across research, policy, and practice aimed at advancing the sexual and reproductive health and rights by, with, and for all women living with HIV,” is essential to successfully undertaking each of the remaining 4 recommendations. As each group discussed how to implement each of the Key Recommendations, meaningful engagement and leadership by women living with HIV stood out as foundational in those processes, consistent with the central principles of Greater Involvement of People Living with HIV (GIPA) 24 and Meaning Involvement of Women Living with HIV (MIWA). 25 For example, when discussing how best to implement recommendation 4 in research, “Use language and terminologies that are actively destigmatizing, inclusive, and reflective of women living with HIV's strengths and experience when discussing sexual and reproductive health and the rights of women living with HIV,” participants highlighted the role of Peer Research Associates (PRAs) b in designing surveys to ensure appropriate and accessible language. For recommendation 5, “Catalyze the reciprocal relationship between evidence and action such that action on sexual and reproductive health and rights is guided by research evidence, and research is guided by what is needed for effective action,” women living with HIV were identified as leaders and crucial bridge-builders between and across stakeholders (eg, between research and CBOs). Considering this over-arching theme, this report focuses on 5 principles identified from the discussion to create supportive, collaborative environments for engagement of women living with HIV that is truly meaningful (Table 1). Each of these principles, discussed in detail below, is a tool can be adapted and used across diverse contexts. Implementation of all 5 Key Recommendations remains essential, informed by the knowledge that meaningful engagement will support the ongoing implementation of the remaining Recommendations. Discussion across the remaining recommendations is summarized in the Supplemental Material.
Principles to Implement Recommendation 1 of the National Action Plan to Advance the Sexual and Reproductive Health and Rights of Women Living With HIV in Canada: Meaningful Engagement of Women Living With HIV Across Sexual and Reproductive Health and Rights Research, Policy, and Practice.

Principles to Implement Meaningful Engagement of Women Living With HIV Across SRHR Research, Policy, and Practice
(1) Acknowledge and actively disrupt power differentials. Attendees emphasized that actively working to dismantle the power imbalances that arise when community and academic, clinical, or social service institutions work in partnership is essential to meaningful engagement. This finding is consistent with previous research that highlights that hierarchal structures and limited decision-making power are barriers to meaningful engagement for women living with HIV. 25 The field of Community-Based Participatory Research (CBPR) has long grappled with the tension that structural power imbalances present in community-academic partnerships.27,28 Central to uprooting and addressing these power differentials is questioning what is defined as “knowledge” and recognizing the value of many ways of knowing, including knowledge from lived and living experiences. 29
Attendees’ insights echoed previous research and they offered specific areas to focus on in addressing power inequities within partnerships with community. These strategies provide pathways that affirm the value of community knowledge. For example, attendees recognized that communication styles can impact the power differentials in a team and suggested the use of round table or Sharing Circle approaches for discussion to ensure all voices are valued, drawing from the wisdom of Indigenous methodologies. 30 Sharing Circles center on sharing stories, creating space for each voice to be heard and drawing on traditions of collective decision making. 31 Compensation practices were also challenged, as attendees highlighted that truly meaningful engagement would value the time of community members and academics equally. The BC Centre for Disease Control (BCCDC) outlines best practices and guidance for peer compensation 32 and was noted as a helpful guide to developing compensation policies for organizations and research teams engaging women living with HIV. Finally, pairing up community members with their collaborators (academics, clinicians, social service providers) to both facilitate skill building workshops was seen as an opportunity to build more reciprocal relationships. Details from the training curriculum of the Canadian HIV Women's Sexual and Reproductive Health Cohort Study (CHIWOS), a well-established community-based research study, provide more insight into how this can be incorporated into training sessions.33,34 These sessions intentionally made space for PRAs to provide insight on the study and approaches from their perspectives, including reflections on barriers for involvement, how they defined success, and their goals for the orientation.
(2) Commit to meaningful engagement as an ongoing, iterative process, not a one-off event. Sustaining meaningful engagement means investing in building trusting relationships and ensuring women living with HIV are involved in all spaces where decisions are being made about their SRHR. The sustained commitment is an important part of avoiding tokenism—sites must be prepared for ongoing engagement before undertaking this work if they want it to be meaningful. In a clinical setting, clinicians can build trust with patients by making their patients feel like they care about them as whole persons—by ensuring there is enough time, openly listening to women's concerns, showing interest in women personally, and using supportive, encouraging, and nonjudgmental communication. 35 When building partnerships in research, academic researchers can build trust in similar ways: by demonstrating interest in partners personally (beyond their role in the specific work or task, while respecting partners’ boundaries with how much they are comfortable to share) and sharing about themselves to their comfort level, being responsive to concerns, and by being actively invested in community issues. 36 Regardless of setting—research, clinical setting, or CBO—it is important to remember that relationship building takes time and a sustained demonstration of commitment and reliability.35,36
Attendees outlined how important the ongoing involvement for women living with HIV is in research. This involves including community members in the whole research process and facilitating access to opportunities usually reserved for formal academics. Women advocated for their involvement in grant writing, designing surveys and choosing language, co-authoring papers, and presenting at research conferences. Teams must provide sufficient training to ensure women can be meaningfully involved in these processes, building beyond data collection skills to expand the breadth of activities women are prepared to support. Research groups in BC33,34,37 and Ontario 38 have examples of detailed community training curricula that can be adapted for a variety of research contexts. Importantly, this may require investment in supplementary and ongoing training that supports peer researchers as their skills develop and career goals change. Women who decide to move out of the HIV space to use their developed skills and training in another field when it aligns with their career goals need to be supported. This is an ongoing commitment to the sustainable involvement of women living with HIV as women grow in their roles and goals.
(3) Learn about the epidemiology and sociostructural forces that create vulnerability for HIV among women in your setting—recognizing that women's whole identities play a role in the kinds of supports they need to engage in this work. All settings, research, clinical, and CBO, must recognize that local needs and priorities are distinct and will inform how community engages. It is incumbent upon researchers, clinicians, and social service providers engaging in this work to understand who the women living with HIV are within their community, including the personal and societal histories and factors that shape their experiences of living with HIV. This is consistent with a “whole-person” approach, acknowledging that womanhood is not the only (or even the main) part of each woman's identity that will shape her experience of HIV and her care needs and desires.
There are a series of resources across Canada that can help understand the epidemiology of HIV among women, both nationally and regionally. Below are some examples of regionally reported statistics that include some disaggregated data, though not all regions have this information available:
National: The Public Health Agency of Canada
7
British Columbia: BCCDC HIV/AIDS reports
39
Alberta: Alberta sexually transmitted infections and HIV reports
40
Saskatchewan: Ministry of Health HIV-AIDS reports
41
Manitoba: Manitoba HIV Program Reports
42
Ontario: Ontario HIV Epidemiology and Surveillance Initiative
43
Quebec: Programme de surveillance de l’infection par le virus de l’immunodéficience humaine (VIH) au Québec
44
However, there are many other types of resources that can provide additional context and information about the experiences of women living with HIV. For example, Indigenous specific groups, like Communities, Alliances, and Networks (CAAN), offer resources to better understand the experiences of HIV among Indigenous peoples across the nation, which is important in the context of historical and ongoing colonization that have led to a disproportionate impact of HIV on Indigenous women.5,6,13,14 CAAN's Fireside Chats series shares research projects from across Canada that focus on Indigenous women and HIV. There are also community-based research studies across the nation that can provide more context and information about the experiences of women living with HIV—including the Canadian HIV Women's Sexual and Reproductive Health Cohort Study, the BC CARMA CHIWOS Collaboration, and Canadian HIV Pregnancy Planning Guidelines Study.45–47 These studies are committed to doing research by, with, and for women living with HIV and their research aims reflect the priorities of women living with HIV. Finally, getting involved in community can help continue learning about the SRHR of women living with HIV—including following social media accounts (eg, CAHR, CAAN, research studies like CHIWOS or the BC CARMA-CHIWOS Collaboration), joining community advisory boards, and seeking out other opportunities to contribute to local CBOs.
Attendees emphasized that part of understanding women's whole identities includes recognizing that there are many social, structural, environmental, and cultural factors that impact women's ability to engage. Thus, any efforts toward meaningful engagement must meet women where they are at. For example, for women who are mothers, availability of childcare may dictate whether they are able to attend programming at a CBO or attend a community advisory board—so extending services to children supports these women. Creating flexible opportunities for engagement is important as well, for instance, creating roles that are modeled after a consultant type role where women can build their own schedules. These more flexible ways to engage will empower women living with HIV to make choices about how and when they participate based on their capacities, desires, financial requirements or restrictions, and other commitments.
Trauma and violence informed employment was also highlighted during the event as an important piece of recognizing women's whole identities and past experiences. In a cohort study of women living with HIV in Canada, 80% of women reported having experienced violence as an adult 48 and almost half had symptoms consistent with posttraumatic stress disorder (PTSD). 49 Employment opportunities that center meaningful engagement must be cognizant that many women living with HIV have had experiences of violence and that a supportive workplace can impact their ability to engage in employment, either as a peer or otherwise. Trauma-informed approaches prioritize safety, transparency, peer support, power-sharing, choice and agency, and intersectional understandings of trauma. 50 Trauma-awareness, which is a recognition of the widespread nature of trauma and its potential impacts on an individual or community, is essential but not sufficient for trauma-informed care and practice. A true trauma-informed approach extends not only to the people receiving services or participating in research, but also to the organization or institution staff. 50
(4) Invest in creating supportive infrastructure, transparent policies and leadership opportunities for meaningful engagement. Intentional development of infrastructure is needed to create spaces where community members are supported, prepared, and safe. Turning to CBPR examples can again provide insight on what this means for meaningful engagement. Previous work among women living with HIV describes the importance of inclusive hiring, comprehensive training, fair compensation, and ongoing support and mentorship for PRAs to create a meaningfully engaged research program or project. 51 Especially in the context of large institutions, transparency about PRA roles and expectations, institutional mandates/requirements, and researcher commitments is integral in creating truly supportive opportunities for meaningful engagement. The CHIWOS research team policies provide an example of transparent and supportive communication around expectations and responsibilities. 52 They include detailed policies around co-authorship, types of activities and compensation practices, the safety and wellbeing of all involved in the study, and many more. For instance, these policies include a detailed list of activities associated with the study and describe whether the activity is paid, volunteer, or if expenses are compensated. CATIE, Canada's source for HIV and hepatitis C information, has detailed guidelines for creating peer health navigation programs that include guidance on roles and responsibilities, management, support, training, compensation, and other strategies for developing peer health navigation programs. 53 Importantly, this document includes a detailed discussion on how to assess an organization's capacity to host a peer support program—an integral first step in developing a peer health navigation program.
Attendees emphasized that for spaces to feel truly supportive, there needs to be a whole team engagement that includes the entire staff. For example, in a clinic, not just the clinicians need to be supportive, but also the receptionist, nurses, medical clerks, and anyone else that is part of the team. Ensuring that all staff are properly trained is an important piece of this process. Trainings focused on Indigenous history, cultural sensitivity, antiracism, and positionality are first steps (eg, San’yas Anti-Racism Indigenous Cultural Safety Training Program or the Indigenous Canada Massive Open Online Course from the Faculty of Native Studies at the University of Alberta).54,55 The Women-centred HIV care toolkit is also a helpful training resource, particularly for those working in a clinical care context.56,57 The toolkits can be supplemented by learning about how the Women-centred HIV Care model can be successfully implemented among trans women and trans feminine people. 58
Advocating the importance of lived and living experience to Human Resources (HR) departments in universities, hospitals, CBOs, and other care setting and ensuring there is buy-in is essential to creating roles for women living with HIV. This is especially important given the loss of women-specific CBOs, especially AIDS Service Organizations, across the country. Attendees emphasized the devastating impact this dearth of resources has generated for many in the community. Given the lack of speciality women's services, the responsibility for providing women-specific programming falls to all organizations providing HIV-related care and services while the fight for funding for specialty women's services continues. Women living with HIV have emphasized that connection with peers is an important piece of meaningful engagement in their clinical care. 25 Attendees added to this idea, highlighting the need for ally support and advocacy for peer-led spaces and research projects that would advance the self-determination and agency of women living with HIV. With support and buy-in from HR departments, roles can be developed that offer both flexibility and opportunities for advancement and leadership. This includes creating spaces for community members to not only be research associates but also step into other research staff roles such as coordinators. Ongoing workshops and training enable community members to grow within their roles. Partnering with HR departments ensures that community members will be fairly compensated for their time and expertise, signaling that community members’ expertise is not valued less than academic expertise. Policies around compensation, expectations/responsibilities for both the employer and the employee, and spaces for career advancement need to be transparently communicated. Integrating clear policies and practices surrounded career expectations, advancement, and compensation can help address some of the tensions that arise for women living with HIV working within the HIV sector, including expectations around unpaid work, navigating shifting roles between a service user and provider, and limitations placed on women about the type and nature of the work they are capable of. 25
Advocacy with HR departments is especially important within academic or clinical settings, where hiring policies can create institutional barriers. Awareness of these policies is essential in being responsive to create supportive employment and leadership opportunities for women living with HIV. Some institutional barriers include caps on how much one person can receive in annual honoraria, specific academic qualifications as a pre-requisite to hiring as an employee, predetermined salary caps that do not recognize the value of lived and living experience, and requirements around the length of time for job postings, which can slow down or impede hiring processes. At some universities, research assistant and coordinator roles are not unionized, which allows for flexible hiring practices but minimal job security. At some institutions, collaborating with HR departments to develop a new role profile that is specifically designed for community members is an option—particularly important is working to develop a role that has appropriate qualifications (ie, does not require certain degrees), but still offers fair compensation that values lived and living experience. In such cases, spending time educating those you are collaborating with on the importance of lived and living experience and peer support/researchers will help advocacy efforts. Further, for those conducting research, highlighting the Canadian Strategy for Patient-Oriented Research, which is an initiative by the Canadian Institutes of Health Research to promote the integration of patient partners in the research process, 59 can illustrate how partnering with community members is a national priority.
(5) Integrate Equity, Diversity, and Inclusion (EDI) principles to ensure that diverse groups, voices, priorities are called into the conversation. Many women living with HIV face barriers to care and meaningful engagement because of intersecting systemic inequities related to their experiences of colonization, racism, or gender discrimination. For example, trans women living with HIV have distinct SRHR priorities and may face distinct barriers to engaging in care, including interpersonal antitrans discrimination and sexual healthcare rooted in cisnormativity.60,61 Integrating EDI principles means taking these distinct barriers into consideration and working to alleviate them so that trans women living with HIV feel welcome and supported to be meaningfully engaged—for instance, ensuring that all staff have training in gender affirming practices. 60 The Women-Centred HIV Care hub can be looked to as an example of how research teams can intentionally work toward integrating diverse voices. 62 This national virtual network of women living with HIV, researchers, healthcare providers, community-based organizations, and community leaders endeavors to support the health of women living with HIV through building capacity and relationships across siloes. The hub is composed of a national steering committee, as well as regional and population specific subhubs. 63 One subhub is focused on the barriers and specific priorities of trans women and gender diverse people in relation to HIV prevention and care. 64 In pursuit of ensuring EDI principles throughout the hub, there is a series of virtual events in the hub titled “Activating Equity in Health Research.” It has featured leadership from the trans women and gender-diverse sub hub to help build capacity among hub members for advancing equity in their research and practice. 65
Another example of a need for equitable solutions to engagement raised by participants was geographical barriers to engagement. Living in rural and northern areas in Canada is associated with higher levels of HIV-related stigma and increased barriers to accessing care and services. 66 While access to services remains a systemic barrier that requires complex solutions, attendees emphasized the need for groups to consider where they could ameliorate these barriers.
Centering EDI principles means not only ensuring diverse groups are invited to the conversation, but that they are able to access that space safely. When engaging with women living with HIV, it is important to ground the work in an anti-oppressive framework, actively challenging, disrupting, and addressing systems of oppression and violence. This includes systemic, institutional, and lateral violence. Lateral violence is when violence is turned onto one's peers, recreating systems of abuse and trauma. 67
Exploring Meaningful Engagement of Women Living With HIV Through Illustrative Vignettes
We acknowledge that many groups are keen to meaningfully engage women living with HIV and may benefit from practical examples and guidance for how to do so. To help imagine what meaningful engagement and each of these key aspects look like, here we include a series of context-specific vignettes that highlight how these can be put into practice. Examining possibilities across clinical, CBO, and research settings, these vignettes are meant to help imagine what implementation might look like, but are not prescriptive. Rather, these vignettes are meant to provide examples of the many different ways to implement recommendations for meaningful engagement. During our in-person event, the 3 panelists discussed their experiences implementing the key recommendations across clinical, CBO, and research settings. The stakeholders present highlighted the usefulness of these practical examples, motivating the co-authors to expand the examples into more detailed vignettes for this article. The vignettes were developed by the lead author (ZO) in partnership with co-authors (EK, MH, and ST) with respective experience within each of the described settings (Figure 2).
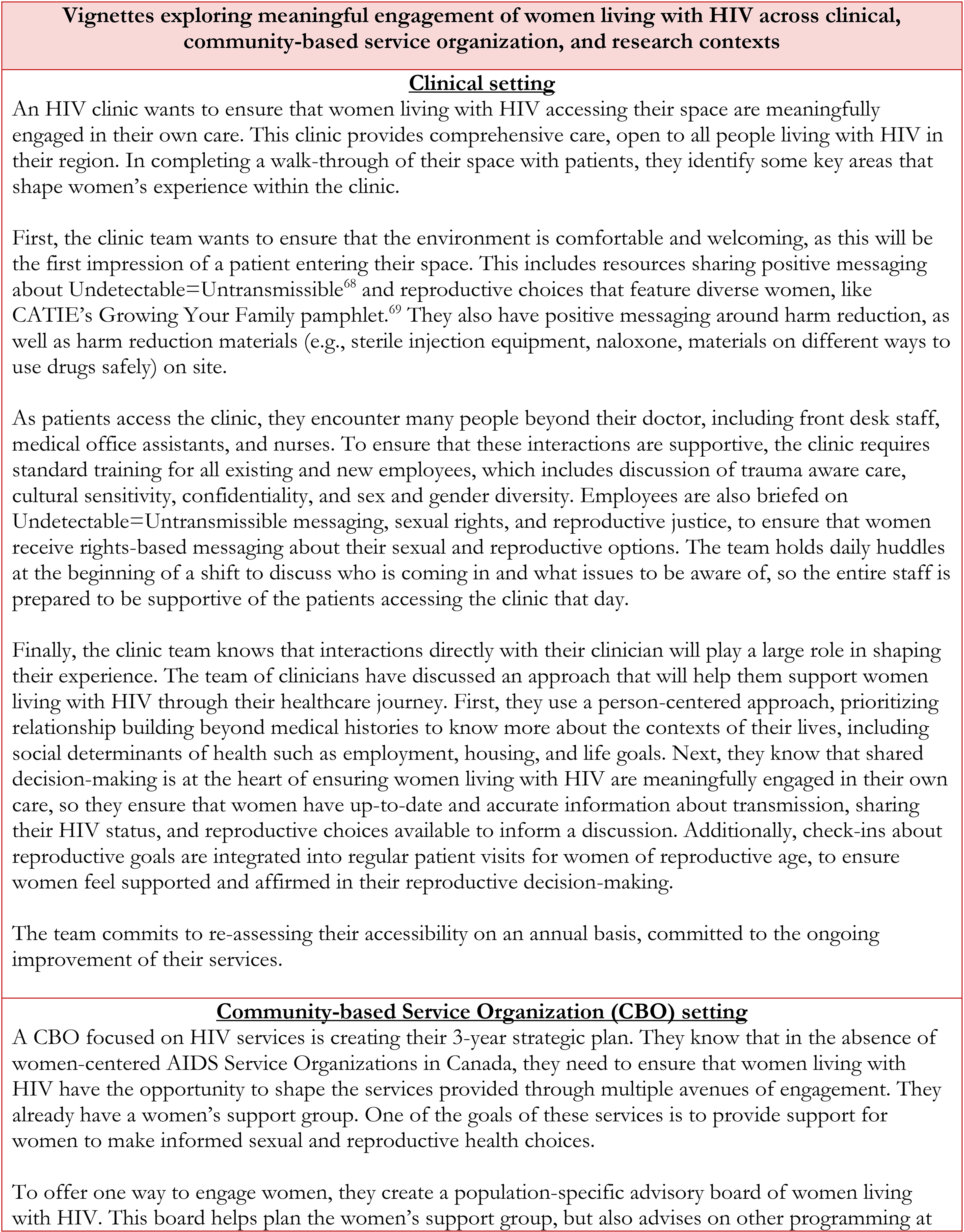
Vignettes Exploring Meaningful Engagement of Women Living With HIV Across Clinical, Community-Based Service Organization, and Research Contexts.
Conclusion
Attendees at the CAHR 2023 in-person community gathering were energized and enthusiastic about continuing to undertake and bring more people into this work together to advance the SRHR of women living with HIV in Canada. Discussion provided foundational insight into implementing each of the 5 recommendations of the National Action Plan: Meaningful engagement of women living with HIV across the sectors involved in SRHR decision making is essential. The principles described here are tools to support the meaningful engagement of women living with HIV and can be adapted across contexts.
Important next steps in implementing the National Action Plan will include ongoing outreach to promote the key recommendations among new groups. It will also entail connecting with key policymakers to advocate for the uptake of the key recommendations into provincial and federal policies. This work is closely aligned with the national Sexually Transmitted and Blood Borne Infection Action Plan in development that centers enabling environments as the foundation of the plan and commits to greater involvement and meaningful engagement of people living with HIV in the STBBI response, providing opportunities for collaboration. 70
We are also working toward collaborative development of an accountability plan for those who have signed the endorsement of the 5 key recommendations. This will include: (1) creating an intentional plan to check in with ourselves and each other for our progress, with guidance from the National Action Plan coordinating team and (2) using opportunities to build accountability mechanisms on the policy and regulation level (eg, Regulation for clinicians at the Public Health Agency of Canada, provincial colleges of clinicians, or health authorities; development of a checklist that can be used in clinical research, similar to other such research guidelines like the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement; 71 creation of online modules that could be completed for Continuing Medical Education credit, providing more incentive for clinicians to familiarize themselves with the key recommendations).
This Canadian initiative serves as a global example for the development of locally tailored action plans to advance the SRHR of women living with HIV, grounded in the centering of meaningful engagement. This work cannot be done alone. In collaboration, we can make a tangible difference in advancing the SRHR of all women living with HIV.
Supplemental Material
sj-docx-1-jia-10.1177_23259582241302773 - Supplemental material for Meaningful Engagement as a Cornerstone for Implementing the Key Recommendations to Advance the Sexual and Reproductive Health and Rights of Women Living With HIV Across Policy, Practice, and Research in Canada
Supplemental material, sj-docx-1-jia-10.1177_23259582241302773 for Meaningful Engagement as a Cornerstone for Implementing the Key Recommendations to Advance the Sexual and Reproductive Health and Rights of Women Living With HIV Across Policy, Practice, and Research in Canada by Zoë Osborne, Muluba Habanyama, Brittany Cameron, Alexandra de Pokomandy, Brenda Gagnier, Elizabeth King, Jill Koebel, Mona Loutfy, Carrie Martin, Renée Masching, Manjulaa Narasimhan, Valerie Nicholson, Neora Pick, Stephanie Smith, Shelly Tognazzini, Wangari Tharao and Angela Kaida in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
This article was co-written by a team of co-authors invested in advancing the sexual health and rights of women living with HIV, including community advocates, academic researchers, clinicians, policymakers, Indigenous Elders, and women living with HIV. We thank moderator Muluba Habanyama, presenters, and participants who attended the in-person community event at the 2023 Canadian Association for HIV Research (CAHR) conference. Thank you to the note-takers and organizing support from Logan Kennedy, Amber Campbell, Shayda Swann, Charity Mudhikwa, and Bluma Kleiner. We are also grateful to Elder Edith Picard for welcoming us and reminding us that, like the Three Sisters, our success in this work is contingent on us weaving together our distinct knowledges, skillsets, and perspectives. We honor women living with HIV across Canada who have shared their experiences and trusted us with their stories.
Author Contributions
ZO was involved in conceptualization, data curation, formal analysis, investigation, project administration, writing—original draft, and writing—review & editing; MH in conceptualization, investigation, writing—original draft, and writing—reviewing & editing; BC, MN, VN, NP, and WT in conceptualization and writing—reviewing & editing; AP, ML, CM, and RM in conceptualization, investigation, and writing—reviewing & editing; BG in conceptualization, investigation, and writing—reviewing & editing; EK in investigation, writing—original draft, and writing—reviewing & editing; JK in conceptualization, investigation, project administration, and writing—reviewing & editing; SS in investigation, writing—reviewing & editing; ST in investigation, writing—original draft, and writing—reviewing & editing; and AK in conceptualization, formal analysis, funding acquisition, investigation, methodology, resources, supervision, writing—original draft, and writing—review & editing.
Ethical Approval and Informed Consent
This project is exempt from Research Ethics Board Review under the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS 2, Article 2.1). Although recommended, the Office of Research Ethics at Simon Fraser University does not require teams to submit applications for exemption.
Declaration of Conflicting Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mona Loutfy is an Editorial Advisor on the JIAPAC Editorial Board.
Funding
The authors received support to host the in-person ancillary event from Simon Fraser University's Provost and Vice-President, Academic Conference Fund (2023/2024). The Scientific Director Grant from CIHR to Angela Kaida supported the research, authorship, and publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.