
Abstract
HIV self-testing (HIVST) has the potential to reduce barriers associated with clinic-based preexposure prophylaxis (PrEP) delivery. We conducted a substudy nested in a prospective, pilot implementation study evaluating patient-centered differentiated care services. Clients chose either a blood-based or oral fluid HIVST kit at the first refill visit. Data were abstracted from program files and surveys were administered to clients. We purposively sampled a subset of PrEP clients and their providers to participate in in-depth interviews. We surveyed (n = 285). A majority (269/285, 94%) reported HIV risk. Blood-based HIVST was perceived as easy to use (76/140, 54%), and (41/140, 29%) perceived it to be more accurate. Oral fluid-based HIVST was perceived to be easy to use (95/107, 89%), but almost all (106/107, 99%) perceived it as less accurate. HIVST improved privacy, reduced workload, and saved time. HIVST demonstrates the potential to streamline facility-based PrEP care in busy African public health facilities.
Introduction
Daily oral HIV preexposure prophylaxis (PrEP) medication is efficacious for individuals with behaviors associated with HIV risk. HIV self-testing (HIVST) improves HIV testing services and is an entry point for PrEP.1,2 Globally, there has been inclusion of PrEP into the national guidelines to increase uptake and effective use.3,4 In sub-Saharan Africa (SSA) countries including Kenya, PrEP is majorly delivered as part of a comprehensive HIV prevention package at HIV clinics to include efficient monitoring, timely risk reduction counseling, and effective documentation. 5 However, there are existing challenges such as; stigma, limited privacy, opportunity costs, and logistical concerns that impede the successful implementation of PrEP in these settings.6,7 Despite these challenges, models of improving PrEP delivery have focused on settings outside the clinic-based setups such as online delivery, pharmacy-based, and community-based.8–10 Improving PrEP delivery services within the context of public HIV clinics is therefore essential for overall health system strengthening.
In 2016, the World Health Organization (WHO) approved HIVST as a novel testing approach that is a safe, accurate, and effective way to reach people who may not test. 11 In addition, the Kenya Ministry of Health HIV testing guidelines now include a self-testing manual that supports HIVST as a supplementary strategy for the identification and establishment of ongoing eligibility for PrEP. 12 However, in the current HIV testing protocols, HIV testing is conducted by healthcare providers. Given that HIV testing is necessary to reduce the risk of antiretroviral resistance, and is required prior to PrEP initiation and ongoing follow-up while on PrEP, it has a tremendous potential to optimize the delivery of PrEP. 13
The Efficiency Study was a prospective pilot implementation study that incorporated the unified theory of acceptance and use of technology (UTAUT) which describes issues with technology acceptance. 14 We used both qualitative and quantitative approaches in a substudy nested in the pilot implementation study to explicate the acceptability and feasibility of HIVST use in public HIV clinics in Kenya.
Methods
Study Design and Procedures
Between March 2021 to March 2022, we conducted a mixed-method study nested within the Efficiency Study (clinical.gov number NCT04424524), a prospective, pilot implementation study evaluating patient-centered differentiated care services that involved the use of HIVST and direct-to-pharmacy refill visits at four public health clinics. The key components of the differentiated care strategy included 3 monthly refills, direct-to-pharmacy visits, and HIVST while waiting for refills. The pharmacy provider conducted adherence counseling at the pharmacy during PrEP refills. Participants had the opportunity to request to see a clinician for consultation. Participating clinics implemented either the current PrEP patient flow without any changes or a pilot differentiated pharmacy-based follow-up PrEP refill pathway.
This article focuses on the 2 public HIV clinics that implemented the differentiated direct-to-pharmacy follow-up PrEP care pathway. At these facilities, participants conducted HIVST while waiting for service during their first PrEP refill visit instead of HIV testing by the clinic staff. At PrEP initiation visit, participants were given an opportunity to take a HIVST kit (either Oraquick rapid HIV-1/2 tests or Sure Check blood-based) (ChemBio Diagnostics, Medford, USA) home for practice use. The use of HIVST kits was demonstrated to participants using pictorial instructions translated into a local language Swahili. The instructions included details on how to perform oral swabs or blood-based testing, how long to wait to read the results, and how to interpret the results. During the refill follow-up visits, participants received a HIVST kit of their choice (either oral fluid-based or blood-based) to conduct the test in a private space at the clinic. The pharmacy provider verified the HIVST test results at the pharmacy before dispensing PrEP. HIVST kits were provided for free to clients as part of the standard of care and the study project supported the provision of HIVST kits whenever the clinic ran out of supply. Participants were followed up for 6 months at the first refill visit (M1) second refill visit (M3) and third refill visit (M6).
Study Setting and Population
Clinics were purposively selected based on the volume of clients accessing PrEP and willingness to pilot the intervention. Participants were eligible for the study if they were men and women accessing PrEP services at the 2 public HIV clinics in Central and Nairobi regions of Kenya, HIV-negative based on rapid HIV tests used in the Kenya national guidelines, ≥18 years, and willing to provide written informed consent for the research component of the project. Additionally, healthcare providers were purposively selected for key informant interviews if they worked at the clinics implementing PrEP delivery to represent different cadres such as nurses, pharmacists, clinical officers, and HTS providers. Individuals who did not meet these criteria were not eligible for participation. The study was conducted for a period of 24 months.
Data Collection
Program data was collected by the Kenya Ministry of Health HIV clinic staff who completed a modified clinic encounter form for the study intervention. Study staff abstracted client records including visit attendance, demographics, and HIV risk assessments weekly. In addition, the study research assistants supporting the facilities administered a brief structured survey to collect data on client experiences and satisfaction with HIVST at visit one. Data were uploaded into REDCap, a web-based application hosted at the University of Washington. 15
For qualitative data, we developed a semistructured interview guide using the UTAUT. The UTAUT is derived from behavioral science and health services literature and can be applied to assessments of intervention acceptability and feasibility. 14 We gathered data on acceptability and feasibility by exploring perceptions, experiences, benefits, and challenges related to HIVST in the context of PrEP delivery in HIV clinics. Interview guides were pilot-tested for relevance, accuracy, and completeness. A subset of participants were purposively selected and approached for the interviews at months 3 and 6. Participants were recruited for qualitative interviews from the parent study during their clinic visit. Qualitative interviewers contacted the participants to schedule and build rapport before the interview. Interviews were conducted by female bachelor-level social scientists (Authors VO, EO, and NW) in the participant's preferred language, either English or Swahili, in private clinic rooms at the healthcare facilities with the interviewing staff and participants only. Interviews were recorded using a digital audio recorder, transcribed, and translated verbatim. Debrief reports were provided after every interview for contextual discussions. We interviewed (n = 20) PrEP clients and (n = 20) PrEP providers. The sample size for our qualitative work was determined by theoretical saturation, 16 we stopped the interviews once no new information emerged. All indepth interviews took an average of 1 h.
Data Analysis
Descriptive statistics for quantitative data were used to summarize participant demographics and responses about the acceptability and feasibility of HIVST. Categorical variables were summarized as frequencies and proportion, and continuous measures were summarized using means and standard deviations or medians and ranges, as appropriate. Quantitative analyses were conducted using R statistical software (version 4.3.1) (R Foundation for Statistical Computing, Vienna, Austria). For qualitative data, we used inductive and deductive content analytic approaches informed by the UTAUT to identify key themes related to the acceptability and feasibility of the HIVST from the transcripts. Coding was conducted using Dedoose software (version 8.3.35) (sociocultural Research Consultants, LLC, Los Angeles, California, USA.) The research team (EO, VO, and NW) discussed discrepancies during the first stage of the coding process until a consensus was reached. Analysts (authors VO and EO) read through all the transcripts and coded the interviews using an agreed-upon codebook. Data were categorized into broader themes and subthemes to understand the acceptability and feasibility concepts that described HIVST use. Our qualitative methods adhered to the consolidated criteria for reporting qualitative research. 17 Simultaneous integration of qualitative and quantitative data approaches was achieved by identifying concepts that provided meaning or expanded on the quantitative results.
Ethical Approval and Informed Consent
The study obtained ethical approval from the Scientific and Ethics Review (SERU) Committee of the Kenya Medical Research Institute (KEMRI/SERU/CCR/0151/3980). All participants provided written informed consent.
Results
Participant Characteristics
A total of 285 participants completed the quantitative surveys; 56% (159) were female with the majority (77%) in serodifferent relationships. The median age was 35 years (interquartile range [IQR] 20-75). The majority (94%) reported feeling vulnerable to getting HIV and (47%) reported no condom use from the last visit. Self-reported PrEP adherence was significantly different among those who conducted self-testing and those who did not (Table 1).
Social Demographic Characteristics of Participants in the Efficiency Study.
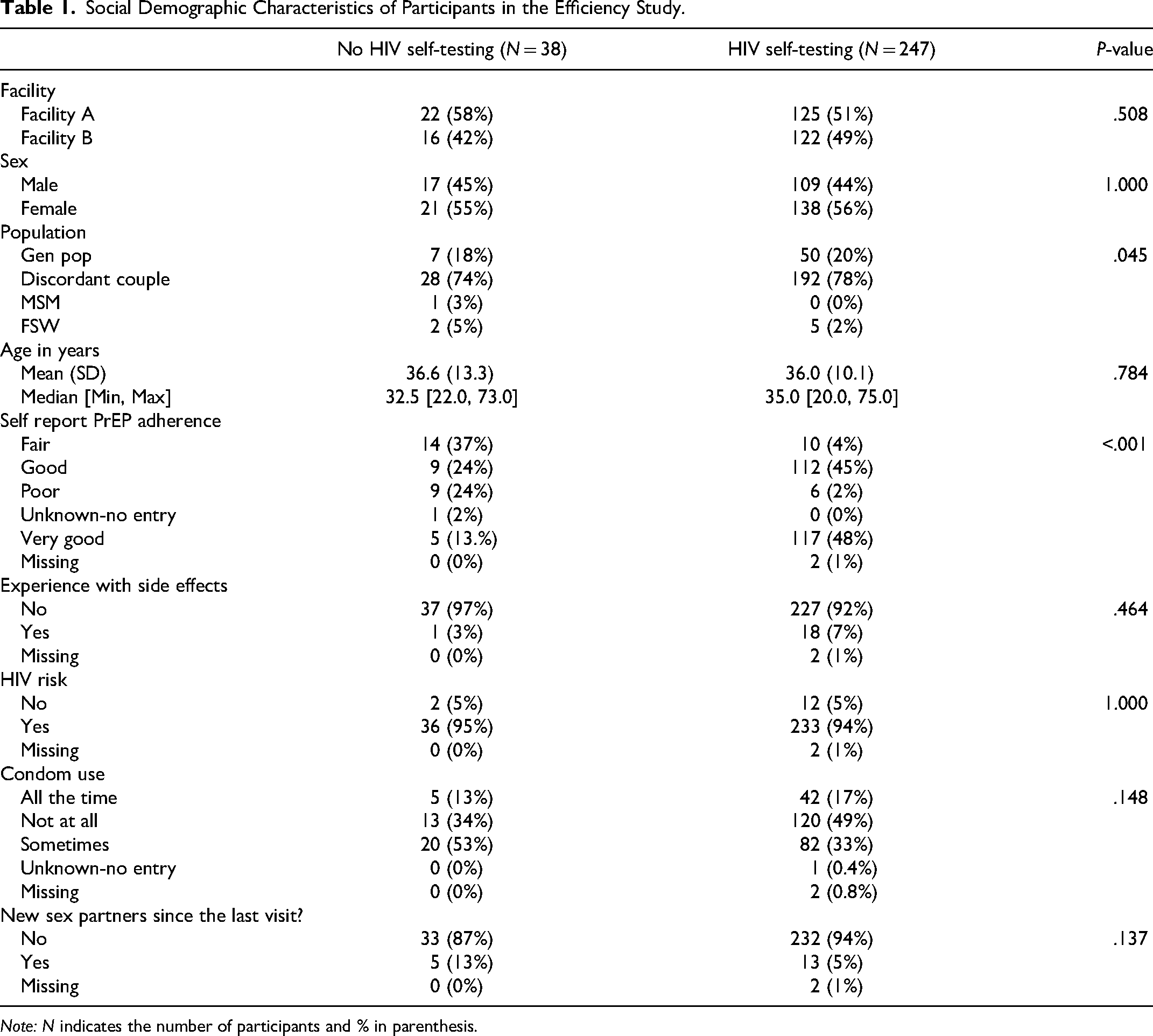
Note: N indicates the number of participants and % in parenthesis.
Feasibility of HIVST for PrEP Services
Overall, 87% (247) participants used HIVST for PrEP services at their first refill visits after initiation, with majority (57%) choosing a blood-based HIVST kit. Among those who used the blood-based HIVST, (54%) felt it was easy to use, while only (29%) perceived it to be more accurate compared to oral fluid-based. On the other hand, (89%) perceived oral fluid-based HIVST to be easy to use, but almost all participants (99%) felt it was less accurate compared to blood-based HIVST. The majority (85%) of the respondents were assisted in conducting both tests at the first PrEP refill visit by a healthcare provider, but those who used oral fluid-based were less likely to need assistance (72%) compared to those who used blood-based (94%) (Table 2).
Proportion of Those Who Used Blood-Based or Oral Fluid Based HIVST (n = 247).
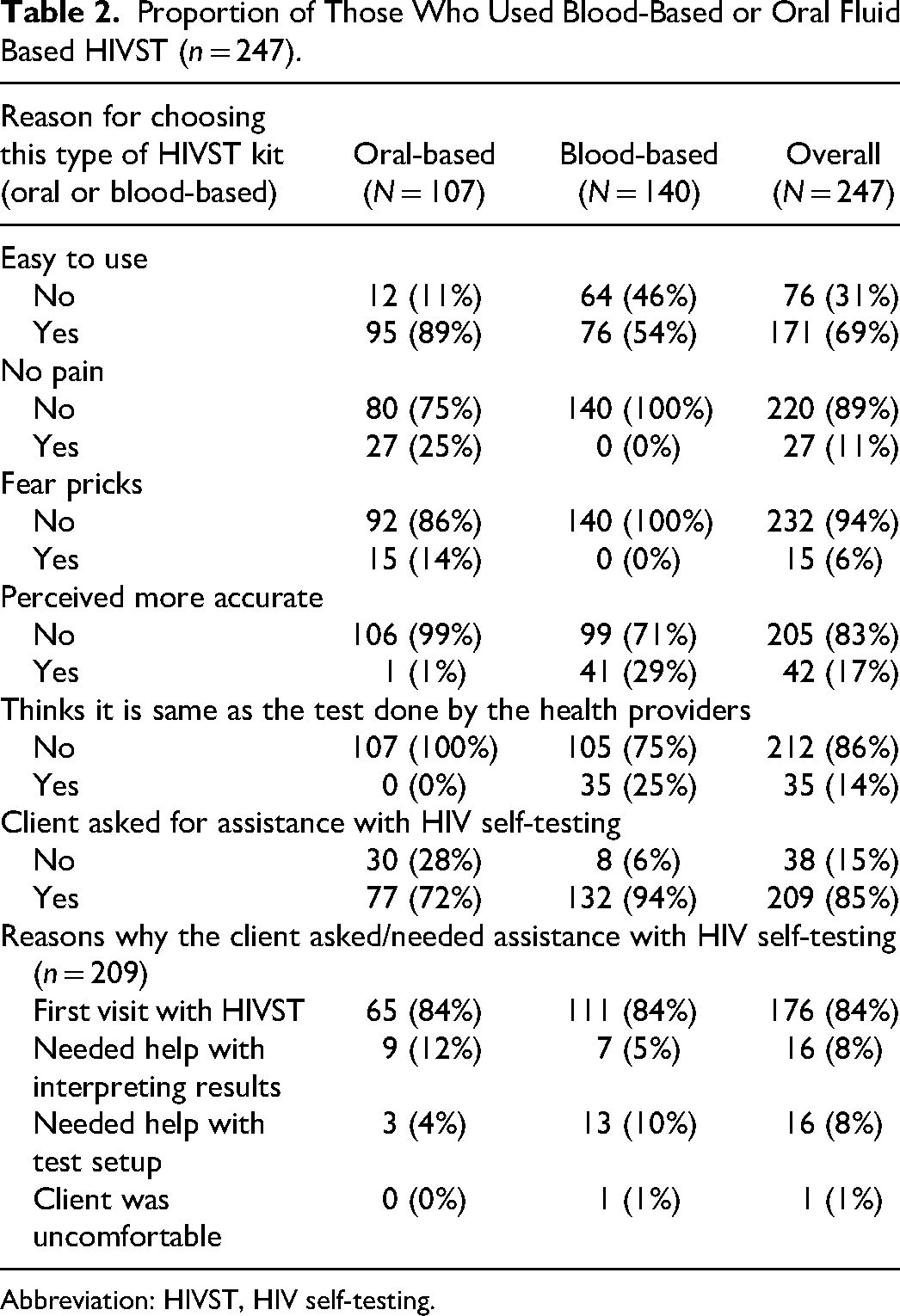
Abbreviation: HIVST, HIV self-testing.
Qualitative Findings
A total of 40 participants completed the qualitative interviews: n = 20 clients and 20 healthcare providers. The average age of clients was 39 years (IQR 33-48) and more than three-quarters (85%) reported being in HIV-serodifferent relationships, with a median PrEP use period of 6 months (IQR 5-26). The average age for healthcare providers was 37 years (IQR 30-41), and providers had been involved in PrEP delivery for an average of 32 months (IQR 12-48). Most (65%) of the healthcare providers were female and half (50%) were HIV testing providers, pharmacists (25%), clinicians, nurses, clinic managers, and social workers (5%) (Table 3).
The Participant's Characteristics in the IDIs and KIIs.
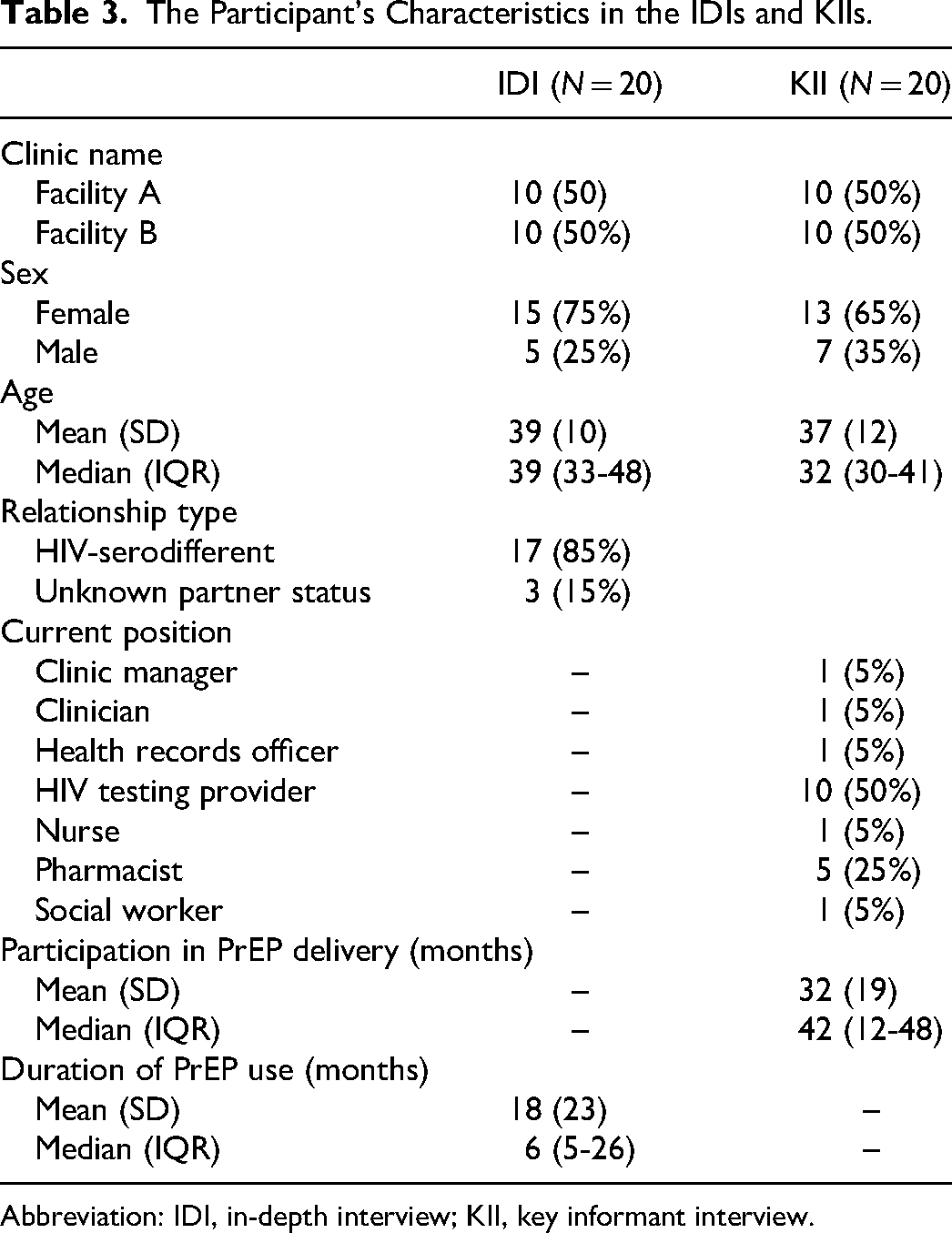
Abbreviation: IDI, in-depth interview; KII, key informant interview.
Overall, there was high acceptability and feasibility of HIVST. Both clients and providers perceived HIVST to be useful as it was private and confidential, reduced stigma, and motivated PrEP use. HIVST was perceived to be convenient by clients, and was also easy to use and interpret the results, although some participants mentioned fear of finger prick as the only challenge for blood-based HIVST. Participants also reported that HIVST helped to improve knowledge of HIV status, disclosure, and self-efficacy. On the other hand, healthcare providers believed HIVST improved work efficiency by reducing workload and saving time allowing them to engage with other tasks. Further, some healthcare providers and clients reported concerns about the accuracy of oral-based HIVST, and limited counseling opportunities compared to provider led testing. Themes and illustrative quotes are described as per the UTAUT constructs namely; perceived usefulness, effort expectancy, social norms or influence and facilitating conditions.
Perceived Usefulness
Privacy and Confidentiality
Clients perceived HIVST to be private and confidential as they conducted the tests and interpreted the results on their own. The perceived privacy reported by clients was because they believed HIVST reduced their chances of “being seen” by other clients seeking antiretroviral therapy (ART) services at the HIV clinics as well as reduced chances of being seen by other providers in different clinic rooms.
One thing I love is privacy, if I test myself and go directly to the pharmacy, they will give me my drugs and I will put them in my bag, and then I leave, so before other people think or see me there, I will have already walked out. [29-year-old female, HIV sero different relationship]
Healthcare providers also echoed the privacy and confidentiality as a key attribute that HIVST provided to clients. Providers mentioned that unlike the provider-conducted HIV rapid testing, the client-led HIV self-testing was not invasive and posed minimal risk for stigma to the client. Mechanistically, providers believed privacy was achieved because clients did not have to queue, but went directly to the private rooms, which reduced their risk of meeting family members or other people known to them. Additionally, providers believed the improved privacy made clients feel safe and secure at the clinic.
For the self-test, it is somehow confidential, you don’t have to test in the presence of the HTS [HIV testing service provider] so it is a friendly test. [Male, social work provider]
Improved PrEP Continuation and Initiation
Providers reported that prior to the intervention, the clinic experienced continuation challenges among PrEP clients due to various reasons such as stigma and long waiting times. Providers felt that clients who conducted HIV tests on their own did not default on their visits because of the reduced waiting time and improved privacy. Providers were particularly happy about this because they were not losing clients and were more confident to show their data on the rising continuation levels. Improved PrEP initiation was due to the fact that PrEP clients referred their peers due to improved services with HIVST.
Yes, it changed so much because previously retention [continuation] was very difficult because they[clients] couldn’t stand those queues because they used to follow the same queue as other HIV patients, which made them feel uncomfortable. Some used to leave even before they received the services and we used to realize that files were retrieved but the clients had already gone. So, when we started self-testing with the direct-to-pharmacy, retention was good and we were able to reach many and we have other more new. [Female, nurse, HIV clinic manager]
Effort Expectancy
Ease of use and Interpreting HIVST Results
Clients reported initial challenges with HIVST use and the need for assistance in the first study visit because HIVST was a new concept to them. However, after illustration and education by providers, several clients felt the HIVST was comfortable, easy to use, and to interpret the results. Clients mentioned that it was easy to learn how to use the kit and very minimal challenges were reported. Among those who reported challenges, fear of finger prick for blood-based kits and the risk of testing HIV-positive in the absence of the healthcare providers were their major concerns. Clients who reported fear of finger prick explained getting used to the test in their subsequent visits.
The first time it was a bit difficult, but today it was easy, because I tested myself and I saw that it was good. [24 year old female, partner of unknown status]
But, the bad thing is, I can test myself, and find that I have the HIV and just leave. Without bothering to tell the doctor because I have already seen. However, if they are present, they will see and give me counseling.[36 year old female, HIV sero different relationship]
Healthcare providers also liked that the HIVST was available in different options to suit individual preferences and reported HIVST was beneficial to clients and easy to use and understand, which minimized unnecessary contact with providers.
It is good especially the Ora-quick [oral fluid based] because we don’t have to keep on pricking. There are so many people who have that fear of finger prick so it is helping them because self-test is easy and it is a bit quick because you don’t have to answer so many questions from the HTS personnel, yeah. [Male, HIV testing service provider]
HIVST Preferences
Participants who were willing to use HIVST were given the option to choose either blood-based or oral fluid-based HIVST. Overall, most clients preferred blood-based HIVST to oral fluid-based HIVST. Clients’ preference for blood-based was because of perceived accuracy, for instance, a client reported that “HIV affects the blood and was counterintuitive to test oral fluids” citing, “I don’t trust saliva.” Blood-based HIVST was also associated with familiarity with the provider-led testing as they felt it was almost similar to the blood-based HIVST and the perception that blood-based HIVST provided results quicker. Clients who preferred the oral fluid-based HIVST associated their preference to it being painless and less worry about finger prick.
I don’t really trust saliva I have not done it before and I don’t know how it works, but if these things [HIV] grow in blood why don’t I just go to the blood direct so that I see. So I prefer the blood so that I can know if I am going strong or anything. And also, the doctor said that if you kiss somebody you cannot infect somebody with HIV, and then when you do a test with saliva it will show if you have HIV, I can never trust that saliva. [40-year-old male, HIV sero different relationship]
Overall, client HIVST was highly supported by healthcare providers. The providers also reported that clients mostly preferred the blood-based HIVST due to perceived accuracy and highlighted that they experienced some challenges initially counseling clients on oral fluid-based HIVST because of clients’ concerns about the results accuracy. However, additional training helped providers to overcome this initial challenge through the use of standardized counseling messages.
The first time, it was hard to convince the client that it is not saliva because most of the clients know it is saliva but there is something you capture. Most clients wanted the one for blood [blood-based] because for the saliva [fliud-based] one is inaccurate. [Female, HIV testing provider]
I have not had any issue with healthcare provider disliking the self-test because of the adequate training and information they have got and by passing the information to the client, interpretation and the testing processes is easy, so no major challenge has been raised. [Male, Social work Provider]
Social Norms/Influence
Improved Disclosure and Client Confidence
Clients generally reported that HIVST improved their confidence and disclosure of PrEP use. Healthcare providers on the other reported that HIVST allowed clients to be involved in their own care, that made them more confident in the PrEP services they received. The HIV pretest counseling offered by health care providers before the HIV test was supplied equipped clients with knowledge that helped improve their confidence.
These days it is so acceptable to the clients, they have accepted it and they feel involved in their care and they have confidence at least we build confidence in them in participating in their care towards PrEP and they really appreciate and the first … the counseling they are being done before they are given the self-test kits, I think with time, it builds their confidence. [Female, Clinic Nurse]
Clients echoed sentiments among providers reporting that they felt more confident with the tests they conducted on their own because they were sure about the results. Some clients felt that provider-led testing may expose them to stigma or discrimination by providers.
So the one for going in different rooms you meet another doctor [health provider] and may be you have become close with them then you start all over again then the shame, but the one that you self-test then you go to the pharmacy and pick the medication is normally okay because you are the one who has self-tested and you have gone to pick the drugs but the one for moving room to room you find different people that one discourages me. [29-year-old female, HIV serodifferent relationship]
Both clients and providers reported that HIVST supported disclosure.Clients especially those in HIV serodifferent relationship reported that HIVST helped to disclose PrEP use to their partners. For instance, clients were given HIVST to take to their partners, and knowing the status of their partners made it easy to disclose PrEP use. In addition, clients who took PrEP because of partner mistrust or partner having other partners had an easy time disclosing their PrEP use whenever their partners tested positive for HIV and they needed assistance from the facility.
I think with disclosure it has been very important for us but you see now if disclosure becomes a challenge to our clients, they may prefer just to carry self-test kits at home and just pretend they don’t know their status and just do a couple of testing and then when they see their partner is negative or see is positive, whichever the results, they are able to come to the facility and get the assistance they need. [Female, Clinical Officer]
Among clients, HIVST helped them to be self-reliant because they did it themselves. Some clients felt it would be a burden to rely on someone else to read and interpret the results for them. Participants added that HIVST also equipped them with the knowledge they needed that could be helpful in the future. For instance, they would be able to buy it and use it at their discretion. A client compared the gained knowledge to “being taught how to eat” and they may not wait “to be fed” to imply they preferred HIVST having gained the knowledge.
You know you do not rely on someone it is your mind concentrating there, and then you get the results you don’t wait for someone to tell you yes or no. You allow someone to think on your behalf it will be a burden and I don’t like it that way. [40-year-old male, HIV serodifferent relationship]
HIVST Reduced Stigma
Providers reported that HIVST helped to reduce stigma because PrEP clients no longer had to queue with ART clients thus reducing their chances of meeting either their friends or family members in the HIV clinic.
Yes, it has been addressed because before, a PrEP client and a client who comes for ARVs used to queue together now this direct to pharmacy with HIVST has helped because when the client comes, he won’t queue, he or she gets tested and thereafter picks the drugs. In a way, it has solved the issue of stigmatization and also, they don’t stay for so long in the hospital. [Female, HIV testing service provider]
Facilitating Conditions
Reduced Workload and Improved Efficiency
Healthcare providers reported that client's HIVST use reduced their workload especially in the triage, social work, and clinician departments and providers also liked that clients did not have to queue and wait for the HIV testing provider. Providers added that they were able to focus on other duties and responsibilities as well as attend to other clients, which led to a “feeling of satisfaction” knowing that the services they offered were acceptable to their clients.
So, it has even improved our work because you can imagine how the five patients queuing there with the others and they all want to be seen by one person, let's say it is triage now they just come and go straight to the HTS even the HTS can tell you today that it is much easier to them because they don’t need to test them, most of them are doing self-testing so they can even take three, give them strategically different areas but all of them are doing it at the same time. So, workload, the workload has been reduced. [Nurse, HIV clinic manager]
Healthcare providers also reported that HIVST improved other services in the hospital such as the assisted partner notification services (APNS) as some clients were able to take the kits to their partners to get tested and reported back to the facility. Through this, providers were able to identify new clients living with HIV who needed care as well as potential PrEP clients. Additionally, providers highlighted initial challenges with clients requesting kits and the availability of self-test kits addressed this challenge.
One thing I like about HIV self-testing is that it has helped us with APNS, I think that is the beauty of HIV self-testing. Because you’ll find they’re those partners that don’t want to come for testing, but once a client tells you ‘Is there a way you can give me a kit … is there a kit that I can go home with and use to test my partner’. So, the HIV self-test has helped us with APNS. [Female, HIV testing service provider]
Time-Saving and Convenient
Clients mentioned that HIVST was convenient and saved time as they did not spend time queuing and waiting for HIV test. It also reduced the time spent in the clinic allowing them to attend to other competing tasks such as work and school. The reduced waiting time at the clinic motivated PrEP use because they were able to attend to other tasks.
This one is much better because doing the HIV self-test is faster. The previous one [provider testing] had long waiting queues and moving from one room to another. Now you just test yourself as you go. [33-year-old, female, HIV serodifferent relationship]
Healthcare providers also reported that client's HIVST improved their work by reducing the queues and helping clients not to spend a long time in the clinic, allowing them to do other tasks.
It is quick, the patient does not delay on the line waiting for a HTS provider. Even when the HTS provider is there, they are able to continue doing other work as the patient is self-testing. [Female, Clinic Nurse]
HIV Self-Testing Concerns
Healthcare providers reported concerns about possibility of missed opportunities for counseling especially related to clients not being able to handle a positive HIV result on their own.
The fact that you can test yourself and maybe find that you are positive, there could be the trauma effect, so most of them would tend to be drastic on themselves because there is no counseling, there is no psychological comfort, yeah, I think it could be stressing. [Female, Pharmacy provider]
A few providers and some clients mentioned concerns with the accuracy of the oral fluid-based HIVST and whether it would produce the same result as the blood-based HIVST. However, providers reported having gained more confidence over time when clients continued to test negative following the provider-led validation tests conducted at month 6 visits.
The first time before I understood it, I didn’t know the relationship between blood and saliva for HIV testing. It was a bit confusing because saliva can give you inaccurate results hence preferred using determine [HIV rapid test]. [Female, HIV testing service provider]
There were also initial concerns about lack of knowledge about the use of HIVST among providers which were addressed through the various trainings that were conducted in the health care facilities. Providers reported that HIVST providers initially felt like they had no work to do and that some worried about job loss, but they quickly adapted to other roles such as screening potential new PrEP clients. Only one HIV testing provider reported fear of losing her job with the introduction of HIVST.
For those working in the HTS, we feel like our jobs could come to an end. Because if people start testing themselves using self-tests, and it is well introduced, then work for HTS providers will not be there. Even if it will be there, for example in our facility there are six of us, we’ll only remain two or three of us. And they will only be acting as guides showing clients what to do. But for the rest, there will be job losses because of the self-test. [Female, HIV testing service provider]
Discussion
In this mixed-method study, we found high acceptability and feasibility of HIVST use to facilitate PrEP delivery in public HIV clinics among both clients and providers. In our quantitative findings, the blood-based HIVST kit was perceived to be accurate while the oral fluid-based HIVST was perceived as easy to use and painless. Majority of the participants required assistance from healthcare providers with the testing during their first study visit which was plausible. However, those who used blood-based HIVST were more likely to request assistance compared to those who used oral fluid-based HIVST which was compounded with a high perception of low accuracy. From our qualitative findings, clients and providers felt HIVST improved privacy and reduced the stigma of being seen at the HIV clinic. HIVST was easy to learn, use, and interpret the results which was also in line with our quantitative surveys. HIVST improved work efficiency by reducing workload and saving time allowing healthcare providers to undertake other tasks. Importantly, HIVST reportedly improved PrEP initiation and continuation.
Our study is unique in focusing on HIVST acceptability and feasibility within the context of facility-based PrEP delivery. The high acceptability and feasibility of HIVST in this study is similar to other studies in different settings.18,19 In addition, research has shown the high acceptability of HIVST among different populations of PrEP users such as female sex workers. 20 However, acceptability within populations, research, and implementation contexts may differ. In addition, there is a paucity of data on acceptability within real-world settings. 21 Blood-based HIVST was preferred over oral fluid-based HIVST as it was associated with a high level of accuracy. Similarly, other studies have shown different levels of specificity and sensitivity for both oral fluid-based and blood-based HIVST.22–24 Studies have shown the accuracy of blood-based HIVST, 25 however, very few describe the accuracy of oral fluid-based HIVST. In our study, oral fluid-based HIVST was perceived to be less accurate, although it was preferred because it was painless and did not require several procedures.
We also found that the use of HIVST reportedly improved privacy, and confidentiality and reduced stigma. HIV stigma has been shown to be associated with provider testing and visiting HIV clinics due to long waiting times and discomfort in the HIV clinic.26,27 A study in Botswana also showed the reduced stigma and testing barriers with the use of HIVST. 28 In our setting, stigma was reduced in the context of facility-based PrEP delivery which has been shown to be a concern among different PrEP populations acessing PrEP at public HIV clinics.27,29 Among providers, the use of HIVST improved the efficiency of their work allowing them to engage in other duties. In Kenya, there have been concerns about high workload and staff shortages in the public HIV clinics due to limited resources, that affect the delivery of PrEP as well as ART. 30 In our study, the use of HIVST addressed some of these challenges by reducing workload and improving work efficiency. Further, PrEP initiation and retention reportedly improved. Several studies have shown barriers to uptake and continuation of PrEP that are either directly or indirectly associated with clinical factors such as stigma and staff shortage.31,32 Our findings, demonstrate the potential of clinic factors addressing these barriers which is key to improving facility-based PrEP delivery.
Clients and providers reported concerns about missed counseling opportunities because of the HIVST. Clients had mixed reactions as some felt counseling was routine and may not be necessary. Providers were concerned about not being able to get counseling opportunities that may not be related to PrEP use such as gender-based violence. It is important to note that in this study, clients were given the opportunity to request counseling services or see the clinician. However, healthcare providers reported that very few sought the service probably because of the need to spend limited time in the facility. On the contrary, several HIV clinic programs have incorporated differentiated care services that bypass counseling and reduce number of ART refills among virally suppressed and stable clients which has shown positive retention outcomes. 33 Admittedly, contexts among ART clients may differ with PrEP clients, and providers may consider innovative counseling approaches with HIVST use among PrEP users.
This study had important strengths and limitations. Principally, a key strength was the use of a mixed-method approach helped us to explain the depth of acceptability and feasibility in our quantitative findings. The primary limitation is that in our quantitative data relied on program data abstracted from client records, which means only variables available in the programmatic ministry of health tools could be analyzed. Additionally, participants were only asked about feasibility of HIVST once at the first refill visit, yet this may vary over time. Secondly, due to the qualitative nature of our study, there may have been a potential of social desirability bias. Acceptability and feasibility of HIVST among PrEP users in the real-world setting may also differ given the divergent healthcare system environments, hence the lack of generalizability of our findings beyond our health system context.
Conclusion
HIVST was highly acceptable and feasible, and improved work efficiency in this study. Framed within the context of facility-based PrEP delivery, interventions improving PrEP delivery services may consider continuous supply of HIVST as well as innovative counseling approaches. Future implementation studies may also explore the acceptability and feasibility of HIVST among PrEP users over time.
Supplemental Material
sj-docx-1-jia-10.1177_23259582241274311 - Supplemental material for HIV Self-Testing for Efficient PrEP Delivery Is Highly Acceptable and Feasible in Public Health HIV Clinics in Kenya: A Mixed Methods Study
Supplemental material, sj-docx-1-jia-10.1177_23259582241274311 for HIV Self-Testing for Efficient PrEP Delivery Is Highly Acceptable and Feasible in Public Health HIV Clinics in Kenya: A Mixed Methods Study by Vallery Ogello, Kenneth Ngure, Paul Mwangi, Emmah Owidi, Njeri Wairimu, Lydia Etyang, Margaret Mwangi, Dominic Mwangi, Simon Maina, Nelly Mugo and Kenneth Mugwanya in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582241274311 - Supplemental material for HIV Self-Testing for Efficient PrEP Delivery Is Highly Acceptable and Feasible in Public Health HIV Clinics in Kenya: A Mixed Methods Study
Supplemental material, sj-docx-2-jia-10.1177_23259582241274311 for HIV Self-Testing for Efficient PrEP Delivery Is Highly Acceptable and Feasible in Public Health HIV Clinics in Kenya: A Mixed Methods Study by Vallery Ogello, Kenneth Ngure, Paul Mwangi, Emmah Owidi, Njeri Wairimu, Lydia Etyang, Margaret Mwangi, Dominic Mwangi, Simon Maina, Nelly Mugo and Kenneth Mugwanya in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-3-jia-10.1177_23259582241274311 - Supplemental material for HIV Self-Testing for Efficient PrEP Delivery Is Highly Acceptable and Feasible in Public Health HIV Clinics in Kenya: A Mixed Methods Study
Supplemental material, sj-docx-3-jia-10.1177_23259582241274311 for HIV Self-Testing for Efficient PrEP Delivery Is Highly Acceptable and Feasible in Public Health HIV Clinics in Kenya: A Mixed Methods Study by Vallery Ogello, Kenneth Ngure, Paul Mwangi, Emmah Owidi, Njeri Wairimu, Lydia Etyang, Margaret Mwangi, Dominic Mwangi, Simon Maina, Nelly Mugo and Kenneth Mugwanya in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgment
We thank the study participants who participated in this project, the entire staff at implementing health facilities, and all the project staff for their motivation and dedication.
Authors’ Contributions
Study conceptualization and funding acquisition: KM; qualitative component study design: KN; data collection: DM, SM, LE, MM, VO, EO, and NW; project administration: KM, KN, and NM; data analysis: PM, EO, NW, and VO; writing—original draft: VO. All authors reviewed and edited the manuscript and approved the final version.
Data Availability
Deidentified data will be available upon author request and under appropriate data-sharing agreements to those who provide a methodologically sound proposal by contacting the International Clinical Research Center at the University of Washington (icrc@uw.edu).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The study obtained ethical approval from the Scientific and Ethics Review (SERU) Committee of the Kenya Medical Research Institute (KEMRI/SERU/CCR/0151/3980). All participants provided written informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute of Mental Health of the U.S. National Institutes of Health (Grant Nos. R00MH118134 and R01MH123267).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.