
Abstract
Despite the prevalence of human immunodeficiency virus (HIV) in Mississippi, access to pre-exposure prophylaxis (PrEP) is mostly limited to urban areas. Remote PrEP care via telemedicine, HIV self-testing, and prescription mail delivery can improve care in underserved communities. This mixed methods study assessed the acceptability and feasibility of using remote PrEP care, compared to alternatives. This consisted of (1) a cross-sectional survey and (2) interviews. PrEP-eligible adults were recruited from community-based organizations across Mississippi while accessing HIV testing between December 2019 and May 2022. Those surveyed (n = 63) indicated the greatest comfort in receiving PrEP via mail delivery (m = 5.14) and telemedicine (m = 4.89) and least comfort at gyms (m = 3.92). Comfort significantly differed between mail delivery and gyms (F = 2.90; P < .01). Those interviewed (n = 26) expressed relatively high comfort with remote PrEP care citing enhanced accessibility, privacy, simplicity, and quality. Remote PrEP services were acceptable and feasible among our sample, thus, should be expanded in Mississippi to address unmet needs.
Introduction
Human immunodeficiency virus (HIV) remains a significant problem in the Southern United States, especially in Mississippi. In 2019, Mississippi had the fifth highest rate of new HIV infections of any state with 19 of every 100,000 people being diagnosed. 1 Pre-exposure prophylaxis (PrEP) is efficacious in preventing HIV transmission.2,3 Yet, in 2021, Mississippi had the fewest individuals on PrEP compared to the number of new infections of any state. 1 In Mississippi, PrEP treatment is mostly performed by specialized physicians located in urban areas with academic centers, serving a small percentage of the state's population but leaving large geographic regions underserved.2,4 Nonmetropolitan Mississippi is at particular risk due to lack of local services, poverty, and stigma,5-7 pointing to the critical need to expand PrEP delivery.
Multiple studies indicate that many at-risk individuals will initiate PrEP if it is readily available.3,8 PrEP delivery has been successfully expanded elsewhere by decentralizing services to settings beyond academic medical centers. These settings include community-based organizations (CBOs), 9 pharmacies,7,10-12 primary care clinics,9,13 mobile clinics, 12 and telemedicine (remote appointments via phone and/or video).7,12,14 Across Mississippi, CBOs provide HIV testing and refer individuals with infection to treatment. However, clients with negative results often leave CBOs without learning about, or being linked to, PrEP care because of inadequate resources and training.5,6,15 Evidence indicates that remote healthcare services such as telemedicine, HIV self-testing (HIVST), and prescription mail delivery are feasible for rural and resource-poor areas, and among diverse populations.7,9,12,14,16-18
Another potential avenue for PrEP expansion, which could also help surmount current geographic limitations, is to offer PrEP information and services in novel settings. One such setting is gyms, where some men who have sex with men (MSM) congregate, including to meet casual sex partners.7,9,12,16-18 Moreover, a study of 311 MSM attending New York City gyms found that 46.3% had engaged in sexual behaviors at the gym in the past 6 months, 19 indicating these venues have potential for contextually driven HIV prevention. A gym-based intervention in London trained some MSM gym attendees to talk to other members about sexual risk and steroid-injecting behavior.20,21
This study investigated the acceptability and feasibility of using remotely delivered services, including telemedicine appointments, HIV/STI self-testing, and medication home delivery, as well as alternative options (including gyms) to expand access to PrEP across Mississippi. The mixed methods design employed cross-sectional survey data and in-depth interviews to assess barriers and facilitators to using these remotely delivered services for PrEP among PrEP-eligible individuals in Mississippi.
Methods
Study Design
This research was conducted in phases: (1) a cross-sectional survey (n = 63), and subsequently, (2) in-depth, single-session interviews (n = 26). For both phases, participant eligibility criteria were as follows: (1) 18 years of age or older; (2) presented at a CBO for HIV testing; (3) PrEP-eligible; and (4) able to read and speak English. All research procedures were approved by the affiliated Institutional Review Boards and are registered on ClinicalTrials.gov. Table 1 presents frequencies and descriptive statistics for demographic variables for both study phases.
Characteristics of Samples.

Notes:
One interview participant did not complete the demographics questionnaire.
One additional interview participant is missing medical literacy data.
Phase One
Procedures
Survey participants were recruited between December 2019 and July 2021, through word-of-mouth and flyers, from five CBOs in North Jackson, Hattiesburg, Gulfport, and the Delta region of Mississippi (where PrEP care is less readily accessible). CBO staff had interested individuals fill out a consent-to-contact form, which was securely sent to research staff. Staff screened interested persons for eligibility, and the electronic consent was completed using HIPAA-compliant DocuSign. One hundred fifty-seven individuals indicated interest, and 83 were not enrolled, among which 55 were not able to be reached and 15 did not complete the consent form. Seventy-four individuals were enrolled, and 11 were withdrawn after not completing the survey within 30 days of enrollment. Phase one included 63 participants who completed the 30 minute survey using HIPAA-compliant REDCap. 22 Each participant was compensated with a $25 electronic gift card. The survey collected demographic data and assessed comfort levels receiving PrEP at eight locations: mail delivered, telemedicine, STI/HIV clinic, mobile clinic, CBO, pharmacy, general health clinic, and gym. For each setting, participants responded to an item asking about their comfort in receiving PrEP and other health-related services there, selecting from six options ranging from “1, very uncomfortable” to “6, very comfortable.”
Data Analyses
Survey data were analyzed using SPSS software, Version 28.0 23 and SAS software, Version 9.4. 24 Differences in participants’ ratings of comfort across settings were assessed using a one-way analysis of variance, and a Scheffé post hoc test was used to evaluate pairwise differences. The mean of the comfort ratings across all eight settings was calculated to assess each participant's overall comfort receiving PrEP services. An independent samples t-test assessed potential differences by gender in participants’ overall comfort.
Phase Two
Procedures
Qualitative interviews included participants from phase one (n = 15) and newly enrolled individuals (n = 11), who were recruited using the same strategies described above. PrEP prescriptions and PrEP telemedicine appointment attendance were abstracted from medical records to ensure the majority of participants had utilized these services. Interview participants were enrolled between March 2021 and May 2022 from the previously identified referral sites (excluding the Delta location). All participants completed electronic consent via DocuSign. Of the 31 individuals enrolled, 26 participants were included in the present analyses. The remaining five did not attend their scheduled appointment. Participants completed a single-session interview via the HIPAA-compliant video conferencing platform Zoom. Each interview was audio recorded, lasted 45–60 minutes, and was accompanied by a brief demographics survey using REDCap. Since phase one found that mail delivery and telemedicine were regarded as the most comfortable way to receive PrEP, the semistructured interview covered experiences, attitudes, benefits, drawbacks, and alternatives to using remote PrEP services. Interview participants received a $40 electronic gift card as compensation.
Data Analyses
Interviews were conducted until data saturation was achieved. All audio recordings were transcribed by a HIPAA-certified, outside transcription company and reviewed for accuracy. A coding scheme was created a priori based on the semistructured interview guide and the quantitative findings. Additional codes were iteratively incorporated into the scheme to address new ideas that arose during analysis. To ensure consistency in coding, over half of the transcripts were independently coded by two team members. Weekly meetings were held to discuss discrepancies, reach consensus on resolutions, and hone code definitions. Upon coding completion, all data were organized using NVivo (QSR International Pty Ltd, 2018); and reflexive thematic analysis was performed. 25
Results
Characteristics of samples (Table 1). For study phase one (n = 63), the mean age was 30.3 years old, the sample was half-male (50.8%), and most identified as a racial minority (85.7%). For study phase two (n = 26), the mean age was 33.8 years old, and the sample was also majority male (65.4%) and racial minority (61.5%). The majority (80.8%) had recently received a PrEP prescription using telemedicine.
Phase One
Participants rated mail delivery (m = 5.14, SD = 1.45) and telemedicine (m = 4.89, SD = 1.43) as the settings in which they would be most comfortable receiving PrEP and gyms as the least comfortable (m = 3.92, SD = 1.99). Results of the one-way analysis of variance test indicated that mean comfort levels differed overall by setting (F = 2.90; d.f. = 7; P < .01). A significant pairwise difference was found only between gyms and mail delivery (Table 2). Overall, women were less comfortable than men receiving PrEP at the locations (m: 4.08 vs 5.07; t = 2.83; P < .01).
Ratings of Level of Comfort Receiving PrEP at Eight Locations (N = 63).
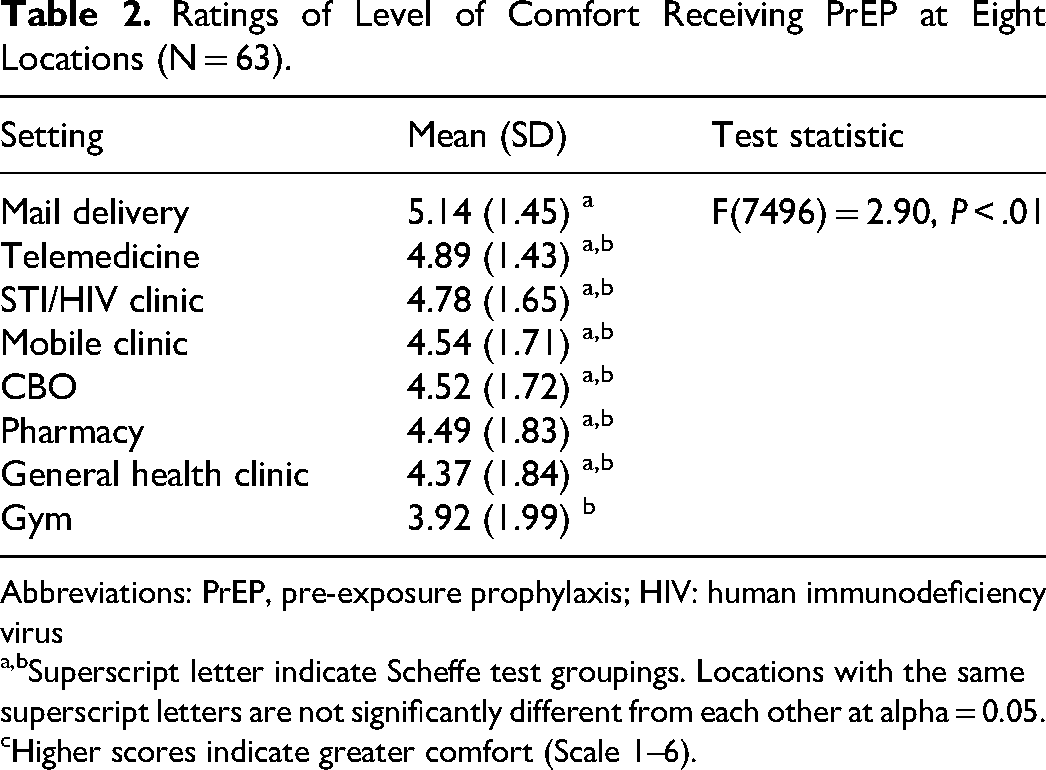
Abbreviations: PrEP, pre-exposure prophylaxis; HIV: human immunodeficiency virus
a,bSuperscript letter indicate Scheffe test groupings. Locations with the same superscript letters are not significantly different from each other at alpha = 0.05.
Higher scores indicate greater comfort (Scale 1–6).
Phase Two
Pros and Cons to Receiving PrEP Services Remotely.
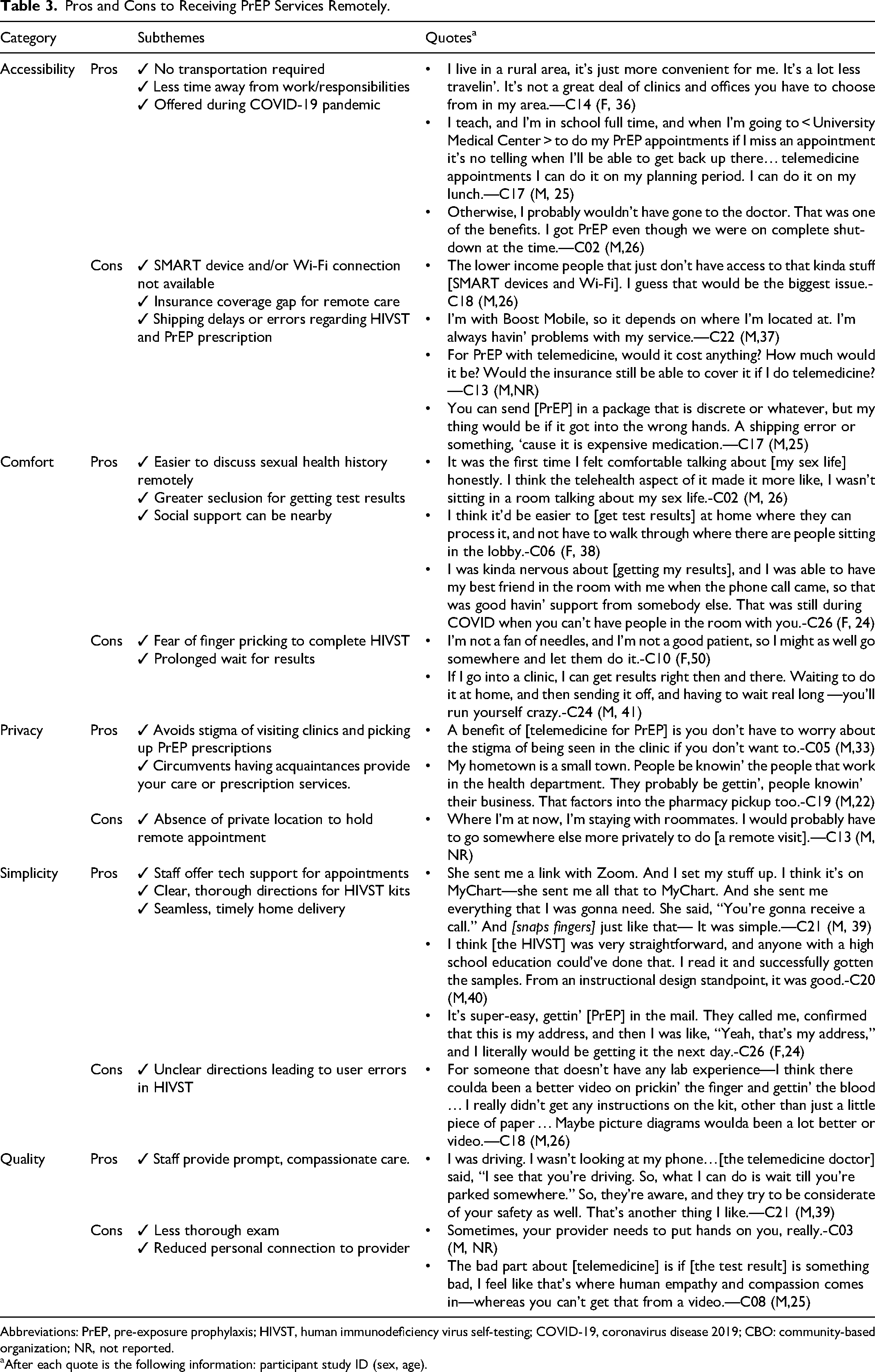
Abbreviations: PrEP, pre-exposure prophylaxis; HIVST, human immunodeficiency virus self-testing; COVID-19, coronavirus disease 2019; CBO: community-based organization; NR, not reported.
After each quote is the following information: participant study ID (sex, age).
Accessibility of Remote PrEP Services
The most frequently voiced accessibility benefit was not needing transportation. This was especially salient for those living in rural areas and those lacking or sharing an automobile. Two participants valued telemedicine for being able to continue PrEP with the same clinician after moving. Additionally, the time savings and convenience of not traveling allowed several participants to engage in PrEP care without interfering with other commitments (eg, work, home care). They attended remote visits during breaks at work, between errands, or at home. Participants also acknowledged that telemedicine ensured they could continue to access PrEP safely through the coronavirus disease 2019 (COVID-19) pandemic.
Of note, participants reported remote PrEP services would not be accessible to everyone. Some voiced concern that lower-income homes may lack a smart device, wireless connection, or cellphone coverage necessary for telemedicine visits. Further, large swaths of rural Mississippi are limited to using internet and cell service providers that are sometimes unreliable. A few individuals expressed concern about whether their health insurance would cover remote appointments. Lastly, some participants worried that PrEP mail delivery could cause shipping delays or errors, forcing them to miss doses, or putting their HIVST kit or prescription in the wrong hands.
Comfort of Remote PrEP Services
Overall, participants reported comfort with remote PrEP care. Some individuals noted that telemedicine made it easier to discuss their sexual history with their provider, bolstering patient–provider alliances. Others voiced appreciation for getting test results at home where they could receive social support and avoid unwanted attention from walking through the waiting room after an appointment.
While nearly all participants reported comfort regarding remote appointments, reports regarding routine HIVST were mixed. Over half reported being afraid of pricking their finger to complete the HIVST. In addition, multiple individuals noted that waiting for the test to reach the laboratory by mail could delay receiving results, which would lead to rumination and emotional distress.
Privacy of Remote PrEP Services
An important factor accounting for participant comfort was enhanced privacy. Most participants live in small communities where everyone is acquainted. Numerous individuals reported knowing the health department workers, clinic staff, and pharmacy technicians involved in PrEP care. While participants acknowledged the existence of HIPAA regulations, they expressed concern about gossip and disclosure of their PrEP use to others. Further, participants reported that clinics currently providing in-person PrEP care were associated with the LGBTQ + community, and they believed visiting these clinics could “out” someone who is not open about their sexuality.
Some participants identified not having access to a private area at home or work to conduct remote appointments as a potential barrier. For example, two individuals who lived in shared accommodations reported that it could hinder their ability to find a comfortable and secluded space.
Simplicity of Remote PrEP Services
Participants who engaged with remote PrEP services found the process easy to navigate. Several stated that staff gave adequate directions on how to join appointments. In a few instances, care teams reportedly spent extra time with them to make remote care easy. One participant was provided a smart tablet to access appointments, while another had technological support to troubleshoot videoconferencing issues. Regarding HIVST, many participants had no problems with the tests and said the directions were clear. Similarly, home delivery was reported to be simple to set up with the pharmacy and prescription deliveries were reliable.
Notably, only one individual stated that directions for HIVST kits were not clear enough and could be improved by including a how-to video or clear step-by-step diagrams.
Quality of Remote PrEP Services
Participants who utilized telemedicine for PrEP services provided glowing reviews of the providers and staff. They described the healthcare teams as prompt, flexible, and compassionate. Specifically, staff was said to work around their clients’ schedules, link individuals to necessary resources (eg, payment assistance, smart devices), and answer any concerns during remote care.
A few participants living in close proximity to a clinic indicated they prefer receiving services in-person. These individuals noted that while remote services may work for PrEP maintenance, they believed it imperative to first develop rapport with the provider face-to-face. In addition, they thought a more thorough physical exam was beneficial.
Regarding Gyms
Multiple participants already engaged in PrEP care reported that all the proposed settings were suitable. They noted that offering PrEP in different settings increases the likelihood that someone will find a location that fits their lifestyle. However, others were opposed to gyms offering PrEP, stating that it would seem “strange” and too public. This dichotomy is exemplified by the following quotes: They’d probably be confused. I’m tryin’ to think, how would I feel if I went to the gym, somebody was talkin’ to me about PrEP. I would get the knowledge, but I don’t know. Some people, they just wouldn’t. I would definitely love it, but I don’t know how other people are. It probably wouldn’t be up there with [other ways to get PrEP]. C19 (M,22)
I think some people might be very interested, and some people might think it's weird… You’ve got some people out here that is completely weird about certain areas in the gym … Some people probably are gonna dislike it. Some people think, why is this actually inside the gym? C16 (M,29)
Discussion
Research comparing methods to expand PrEP services beyond Mississippi's urban, academic centers is imperative to address the state's low PrEP-to-need ratio. 1 Therefore, the present research employed mixed methods to assess the acceptability and feasibility of using remotely delivered PrEP services, compared to other care options. In summary, of the 63 Mississippi adults surveyed, mail delivery was regarded as a more comfortable way to receive PrEP than receiving it at gyms. When 26 individuals were interviewed regarding this topic, they cited elevated accessibility, comfort, privacy, simplicity, and quality as positive attributes of remote PrEP services (ie, telemedicine, HIVST, mail delivery), which make this an attractive option.
The finding that remote services are an acceptable and preferred method for decentralizing and expanding PrEP access in Mississippi reflects previous findings.7,12,14 Like prior studies, telemedicine was seen as a promising way to reach tech-savvy young adults (most at risk for HIV acquisition) and rural communities, while overcoming the stigma associated with entering HIV/STI clinics.7,12,14 However, participants identified potential hurdles (eg, lack of a smart device, Wi-Fi, or private location) that will need addressed. One solution could be the hub-and-spoke approach in which local health organizations connect patients to a remote PrEP specialist using a private exam room. 7 Also, one participant mentioned a Mississippi assistance program that provides a smart phone to those who qualify. Our sample exhibited greater skepticism towards HIVST.7,12,18 In a past review of three randomized trials, one found that HIVST in lieu of lab visits improved PrEP adherence, while two found noninferior effects. Participants in all three studies deemed HIVST acceptable and preferred to in-person testing. 18 The PrEP@Home study similarly found that over 80% of participants opted for HIVST over lab visits. 7 In comparison, our sample was split, with roughly half wishing to avoid HIVST due to concerns of physical pain, user errors, and delays in getting results. Like Rousseau et al, 12 we found that PrEP home delivery was seen as a valuable tool to avoid travel, save time, and enhance privacy. However, certain barriers to home delivery have been noted. D'Angelo et al, 9 found that locating a mail-order pharmacy covered by insurance and timing refills can be challenging, and some were concerned about privacy. Three of our participants worried that mail delivery could cause errors/delays and reduce privacy.
The present study benefited from obtaining both quantitative and qualitative feedback from individuals who were eligible for PrEP or had used it. This allowed for a more holistic view of PrEP needs and preferences. Another strength was that by querying participants on their comfort and preferences across numerous, diverse settings, we were able to see how hypothetical care options compare to existing opportunities.
However, there are a few notable limitations. The sample size was relatively small and from one state. Therefore, findings may not be generalizable to populations outside of Mississippi. Nonresponse bias may also impact findings. Only 40.1% of those who completed consent-to-contact forms for phase one were successfully reached, enrolled, and completed baseline. Similarly, 16.1% of those who consented for an interview never completed one. Lastly, most of our qualitative sample received PrEP using telemedicine and home delivery. Therefore, they were able to draw from experience when asked about the benefits and limitations of these options compared to hypothetical ones (ie, gyms).
Future research could implement PrEP services at gyms (and other innovative, more commercial settings) and investigate participants’ lived experiences. To our knowledge, only one study has ever attempted to provide HIV prevention education at gyms. While found feasible, the initiative was not able to reduce risk behavior, likely due to attrition among peer educators.20,21 Studies could also explore preferences among populations in other states and countries and tailor PrEP services to fit local needs and context.
In summary, research shows that when PrEP is made readily available, many individuals at risk for HIV will seek and obtain a prescription.3,8 At present, barriers, such as transportation and stigma, persist, undermining accessibility. Expanding remote options for PrEP care could alleviate these concerns and encourage prescription initiation, while reducing healthcare costs.16,17 Regardless, participants made it clear that whatever is done to enhance PrEP convenience must not be at the cost of their privacy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Our study was approved by the Institutional Review Board of both the University of Mississippi Medical Center (#2018-0080) and Rhode Island Hospital (#1223057). All participants provided written informed consent prior to enrollment in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible with help from the Providence-Boston Center for AIDS Research (P30 AI 042853) and support from grant number R34MH115744 (Brown) from the National Institute of Mental Health (NIMH).