
Abstract
Background
This study determined the trends of transfusion-transmissible infections (TTIs) among blood donors in a regional hospital in Ghana from 2017 to 2022.
Methods
A retrospective analysis was conducted on 6339 blood donor records. Data were analyzed using STATA version 17.0 at the 0.05 significance level.
Results
The prevalence of TTIs was 31.4% in 2017, 13.8% in 2018, 20.4% in 2019, 9.5% in 2020, 9.6% in 2021, and 11.7% in 2022. There were significant associations between hepatitis C virus (HCV), Syphilis, and sex (OR = 2.06; 95% CI [1.29-3.30]; P = .003) and (OR = 2.28; 95% CI [1.48-3.54]; P < .001), respectively. Blood donors aged 20-29 were more likely to be infected with hepatitis B virus (OR = 1.96; 95% CI [1.28-2.99]; P = .002). Blood donors aged 40-49 had higher odds of infection with HCV (OR = 3.36; 95% CI [2.02-5.57]; P < .001) and Syphilis (OR = 3.79; 95% CI [2.45-5.87]; P < .001).
Conclusion
The study highlights the need to implement targeted prevention strategies for donors with a higher TTI prevalence.
Plain Language Summary
Background
Despite efforts to enhance the safety of the blood supply, transfusion-transmissible infections (TTIs) continue to pose a significant problem. This study determined the trends of TTIs among blood donors in a Regional Hospital in Ghana from 2017 to 2022.
Methods
A retrospective analysis was conducted on the records of 6,339 blood donors to determine the presence of anti- human immunodeficiency virus 1/2 IgG/IgM, hepatitis B virus (HBV), anti-hepatitis C virus (HCV) IgG/IgM, and anti-Treponema pallidum IgG/IgM/IgA. Data were analyzed using STATA version 17.0. Both descriptive and inferential statistics were employed at a significance level of 0.05.
Results
Of the 6339 blood donors, 16.1% showed serological evidence of at least one TTI. The trend analysis showed that the prevalence rates of TTIs were 31.4% in 2017, 13.8% in 2018, 20.4% in 2019, decreased to 9.5% in 2020, 9.6% in 2021 and increased to 11.7% in 2022. TTIs were dominant among male blood donors compared to female blood donors. There was a significant association between HCV, Syphilis, and sex (aOR = 2.06; 95% CI [0.59-1.73]; P = .003) and (aOR = 2.28; 95% CI [0.15-0.69]; P < .001) respectively. Donors aged 20 to 29 were more likely to be infected with HBV (aOR = 1.96; 95%CI [1.28-2.99]; P = .002). Also, donors aged 40 to 49 years were more likely to be infected with HCV and Syphilis (aOR = 3.36; 95% CI [2.02-5.57]; P < .001) and (aOR = 3.79; 95% CI [2.45-5.87]; P < .001) respectively.
Conclusion
The study identified a high overall prevalence of TTIs, highlighting the need to encourage female donor participation, raise awareness among young adults about safe practices, and implement targeted prevention strategies for males with a higher TTI prevalence.
Introduction
Blood transfusion, a vital therapeutic intervention for patient survival, also poses the risk of transmitting infections such as the human immunodeficiency virus (HIV), hepatitis B virus (HBV), Syphilis, and hepatitis C virus (HCV).1,2 This risk stems from potential contamination of donated blood with infectious agents, leading to transfusion transmissible infections (TTIs). TTIs may occur due to various factors, including inadequate screening of donors, failure to detect early-stage infections, or human errors in the testing process.3,4 In some cases, blood donors may unknowingly carry these infections, making it challenging to eliminate the risk. However, the proper screening of blood may minimize this risk.
Globally, prevalence rates for these infections in collected blood donations vary, with HIV ranging from 0.003% to 1.08%, HBV from 0.03% to 3.70%, HCV from 0.02% to 1.03%, and Syphilis from 0.05% to 0.90%. 5 In Iraq, there was a decline in hepatitis B by 26%, hepatitis C by 21.4%, and Syphilis by 5.3% from 2019 to 2021. 6 Also, Ayilo et al 7 reported an overall prevalence of TTIs of 4.6% in Ethiopia.
The World Health Organization (WHO) strongly advocates the mandatory testing of all blood donated for infectious diseases, which is now a compulsory and regularly conducted practice in blood banks. 5 This stringent screening aims to prevent the transmission of TTIs to blood recipients during transfusions. Despite these measures, the challenges lie in the persistent threat of TTIs, particularly in low- and middle-income countries where resources and accessibility remain limited. 8
In sub-Saharan Africa (SSA), a systematic review conducted by Puerto-Meredith et al 9 reported an overall prevalence of TTIs to be 2.0%, with HBV being the most prevalent at 3.0%, followed by HIV, HCV, and Syphilis at 2.0%, 1.0%, and 2.0%, respectively. In Ghana, the overall TTI prevalence is 21.0%, with specific rates for HBV (6.6%), HCV (4.9%), HIV (2.9%), and Syphilis (6.8%). 10 A study conducted in Akatsi South Municipality in the Volta region of Ghana also reported an 8.0% TTI prevalence, including HIV (3.8%), HBV (3.2%), and HCV (1.0%). 11 Similarly, in the Hohoe Municipality seroprevalences for HIV, HBV, HCV, and Syphilis were 3.9%, 5.0%, 4.2%, and 5.2%, respectively. 12 Beyond the immediate health effects on recipients, TTIs raise greater public health concerns that call for continuous efforts to improve blood transfusion safety procedures and protocols.
Recognizing the significant threat of TTIs to blood recipients, regulatory bodies and public health authorities prioritize mandatory testing for these diseases. Presently, stringent screening protocols in blood banks aim to ensure recipient safety and address public health imperatives. 13 Despite efforts by Ghanaian health facilities, TTIs persist as a concern, as evidenced by prevalence rates outlined in various studies, including those in the Volta region. This study seeks to contribute valuable insights by examining trends in TTIs among blood donors in a Regional Hospital in Ghana, spanning 2017 to 2022.
Methods
Study Site Description
The Hohoe Municipality is in the Volta Region of Ghana and is among 1 of the 18 Municipalities in the region. The population of the Hohoe Municipality according to the 2021 population and housing census stands at 114 472 with 54 893 males and 59 579 females. 14 The Municipality is located in the central part of the region. It consists of 102 communities with a growth rate of 2.4%. 14 The Volta Regional Hospital (VRH) Hohoe is a government-owned healthcare facility in the Municipality. The Hospital serves is a referral center for various healthcare facilities in the Volta Region and beyond. As the setting for the current study, VRH provides a suitable environment with a significant number of blood donors and a well-equipped laboratory for testing donated blood.
Study Setting, Population, and Eligibility Criteria
This study was conducted at the blood bank unit of the VRH. Researchers manually reviewed all available archived results on blood donation from the hospital's laboratory between January 2017 and December 2022. The data reviewed included sociodemographic variables and results of HBV, anti-HCV, HIV, and Syphilis. Eligibility criteria for the study included donors whose blood donation records were available in the Hospital's laboratory archives, records that included complete information on sociodemographic variables, and records that included complete results for HBV, anti-HCV, HIV, and Syphilis tests. Records with incomplete sociodemographic information or lacking results for any of the tests (HBV, anti-HCV, HIV, or Syphilis) were excluded from the study.
Study Design
A retrospective design was adopted using secondary data at the blood bank unit of VRH, Hohoe. This design was most suitable because it allowed for detailed and longitudinal analyses of TTIs in the VRH Hohoe. We have followed the Strobe Guidelines when preparing this manuscript.
Sample Size Determination
The sample size for this study was all data captured in the blood donors’ register within 6 years (January 2017 to December 2022).
Sampling Method
The VRH being the only health facility with a functional blood bank in the entire Hohoe Municipality was purposively selected for the study because it is the only hospital with the required data needed for the study.
Data Collection Procedure
The data collection procedure entailed manual review of blood donors’ records from January 2017 to December 2022. Data from the blood donors’ register, including age, sex, and results of HBV, anti-HCV, anti-HIV, and Syphilis tests were retrieved and reviewed manually. The screening for HIV, Hepatitis B surface antigen (HBsAg), and Anti-HCV was done using ELISA kits from Abbot® (USA). The test for Syphilis was done using the Rapid Plasma Reagin test from Omega Diagnostics® (UK). Five millilitres of blood were collected from each donor, and sera from all the blood samples were checked for the presence of HBsAg and antibodies to HIV-1/2, HCV, and Syphilis using the automated i1000SR immunoassay system from Abbot® (USA), following the manufacturer's instructions.
Data Analysis
Data were captured using Microsoft Office Excel 2019, validated using EpiData version 3.1, and analyzed using STATA version 17.0. Descriptive and inferential statistics were performed at the 0.05 level of significance and 95% confidence interval. The results were displayed in frequency tables and charts.
Results
Demographic Characteristics
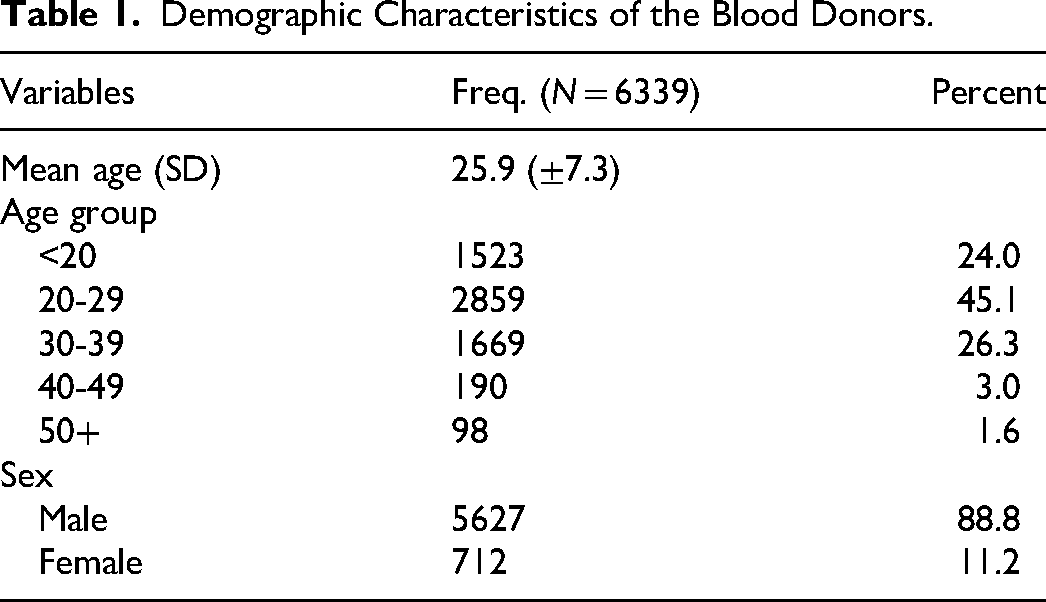
A retrospective analysis was conducted on the records of 6339 blood donors during the period from 2017 to 2022. The mean age of the donors was 25.9 ± 7.3. Among the donors, the majority, 5627 (88.8%) were males and 2859 (45.1%) were aged 20 to 29 years (Table 1).
Demographic Characteristics of the Blood Donors.
Trends in the prevalence of transfusion-transmissible infections (2017-2022)
Figure 1 shows the trends in the prevalence of TTIs over the years 2017 to 2022. Of the 6339 blood donors, 1019 (16.1%) had serological evidence for at least one infection. The prevalence of TTIs varied across the years. In 2017, 19.0% of 1207 donors screened had TTIs, with HIV being found in 68 donors (5.6%), HBV in 70 donors (5.8%), HCV in 155 donors (12.8%), and Syphilis in 86 donors (7.1%). In 2018, 12.0% of 762 donors screened had TTIs, with HIV detected in 9 donors (1.2%), HBV in 13 donors (1.7%), HCV in 41 donors (5.4%), and Syphilis in 42 donors (5.5%). In 2019, 12.9% of 815 donors screened had TTIs, with HIV detected in 7 donors (0.9%), HBV in 38 donors (4.7%), HCV in 37 donors (4.5%), and Syphilis in 84 donors (10.3%). In 2020, 17.7% of 1124 donors screened had TTIs, with HIV found in 3 donors (0.3%), HBV in 22 donors (2.0%), HCV in 19 donors (1.7%), and Syphilis in 63 donors (5.6%). In 2021, 16.6% of 1050 donors screened had TTIs, with HIV detected in 1 donor (0.1%), HBV in 20 donors (1.9%), HCV in 22 donors (2.1%), and Syphilis in 58 donors (5.5%). Finally, in 2022, 21.8% of 1381 donors screened had TTIs, with HIV being detected in 11 donors (0.8%), HBV in 33 donors (2.4%), HCV in 46 donors (3.3%), and Syphilis in 71 donors (5.1%). Overall, across the entire 6-year period, encompassing 6339 donors, the prevalence of different TTIs was as follows: HIV was present in 99 donors (1.6%), HBV in 196 donors (3.1%), HCV in 320 donors (5.0%), and Syphilis in 404 donors (6.4%).
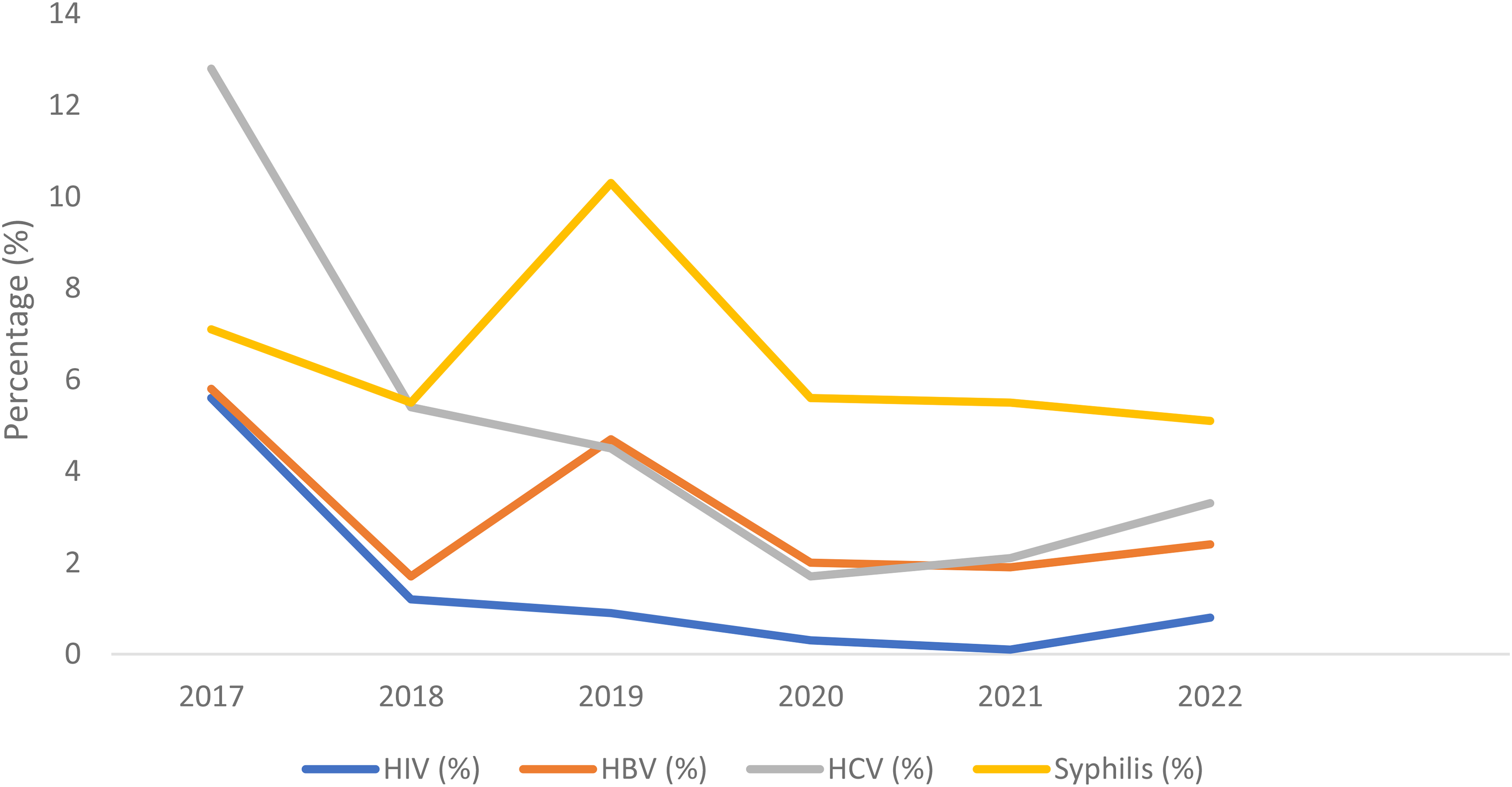
Trends of transfusion-transmissible infections.
Odds for HIV, HBV, HCV and Syphilis Status and Sex and Age
The study found that males were more likely to be infected with HCV and Syphilis than females (OR = 2.06; 95% CI [1.29-3.30]; P = .003) and (OR = 2.28; 95% CI [1.48-3.54]; P < .001) respectively. Donors aged 20-29 were more likely to be infected with HBV and HCV (OR = 1.96; 95% CI: 1.28-2.99; P = .002) and (OR = 1.70; 95% CI: 1.26-2.29; P < .001) respectively. Donors aged 40-49 were more likely to be infected with Syphilis and HBV (OR = 3.39; 95% CI [1.54-7.48]; P = .002) and (OR = 5.93; 95% CI [3.24-10.84]; P < .001) respectively. Donors of the same age group were more likely to be infected with HCV and Syphilis (OR = 3.36; 95% CI [2.02-5.57]; P < .001) and (OR = 3.79; 95% CI [2.45-5.87]; P < .001) respectively (Table 2).
Odds for HIV, HBV, HCV and Syphilis Status by Age and Sex.
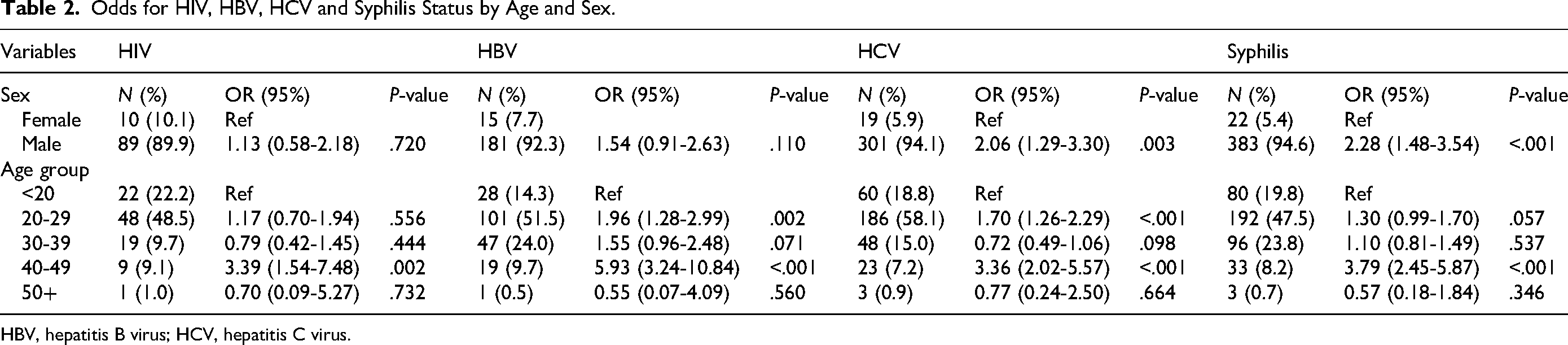
HBV, hepatitis B virus; HCV, hepatitis C virus.
Discussion
This current study determined the seroprevalence of TTIs among blood donors in VRH of Ghana from 2017 to 2022. The results revealed a notable proportion of blood donors, specifically 16.1%, showing serological evidence of at least one TTI. This observed seroprevalence of 16.1% falls within the range of previous reports in Ghana, indicating a consistent trend. For instance, this prevalence aligns closely with studies conducted within the Hohoe Municipality and the Offinso-North District, which reported a prevalence of 18.3% and 19.1% respectively.12,15 The prevalence observed in this study was higher when compared to that of a study conducted in the Akatsi South Municipality in the Volta region of Ghana (8.0%), 11 2% in SSA, 9 10.1% in Northern Tanzania, 3 9.4% in Kenya 16 and 3.6% in Eritrea. 17 However, this finding was lower than what was reported in three multicentered health facilities in Ghana (21.0%). 10 The observed variations in these findings could be attributed to differences in sample size, health systems, exposure factors of TTIs in these countries, donor recruitment methods, demographic characteristics, and the sensitivity of diagnostic tests used for screening.10,12,15 This current study may have had more sensitive and accurate screening and testing protocols, leading to the detection of more cases of TTIs. Also, high-risk populations in Ghana may engage in riskier behavior compared to those in Northern Tanzania, Kenya, and Eritrea, leading to a higher prevalence of TTIs. The finding underscores the importance of developing targeted interventions to reduce the burden of TTIs in vulnerable populations.
The study found the overall seroprevalence of HIV among blood donors to be 1.6%. This finding is similar to the rates of 1.24% and 2.1% found in other studies conducted in Ethiopia 18 and Angola. 19 However, a study conducted in India reported a lower HIV seroprevalence of 0.25%. 20 Moreover, the seroprevalence of HIV in this current study is lower than prevalence rates reported in Hohoe Municipality (3.9%), 12 Ho Municipality (4.8%), 21 Offinso-North District (10.9%), 15 Equatorial Guinea (7.8%), 22 and Nigeria (4.2%). 23 The possible explanation for the differences in the prevalence of HIV among blood donors in this study and other studies could be attributed to differences in study settings, the screening and testing protocols, changes in the behavior of high-risk populations, and the effectiveness of public health interventions aimed at reducing the burden of HIV.15,24 The public health implications of this finding are significant, as they highlight the need for continued health education on HIV preventive measures, monitoring and screening for HIV, particularly among high-risk populations, to prevent the transmission of the disease and its complications.
The seroprevalence of HBV in this current study was 3.1%. This finding is similar to what was found in SSA (3.0%). 9 This finding is lower when compared to other studies; Osei et al 21 reported a prevalence of 7.5% in Ho Municipality, and Adu-poku et al 12 reported a prevalence of 5.0% in the Hohoe Municipality. The lower seroprevalence of HBV in the current study compared to other similar studies within Ghana could be due to differences in the study population, study design, and the period the studies were conducted. Conversely, the prevalence from the current study was higher than the reported prevalence in Brazil (1.63%), 25 Eritrea (2.0%), 17 India (0.49%), 26 and Qatar (0.30%). 27 These differences in prevalence can be attributed to diverse factors, including sociodemographic, socioeconomic status, cultural behaviors, risk factors, awareness, and the efficacy of preliminary screening and laboratory diagnostic methods. It is crucial to note that screening blood donors solely for HBsAg is insufficient to exclude HBV, particularly during the core window period, which could result in posttransfusion hepatitis B in recipients. Therefore, incorporating anti-HBc testing is crucial, as it significantly reduces the risk of posttransfusion hepatitis B infection. Additionally, implementing HBV DNA screening among blood donors is essential to eliminate the risk of HBV transmission through blood transfusion.
Furthermore, the seroprevalence of HCV in the current study was 5.0%. This finding is similar to what was reported in the Hohoe Municipality (4.2%). 12 This prevalence is higher when compared to what was found in Greater Accra and Central regions of Ghana (0.57%), 28 in Calabar, Nigeria (3.1%) 23 in Qatar (1.87%) 27 and in Asmara, Eritrea (0.7%). 17 However, this finding is relatively lower as compared to what was reported in Kenya (8.0%). 4 The differences between these findings could be due to differences in the methods used and the accuracy of the testing kits. The technology used for screening might have improved, making the current tests more accurate and dependable. This difference could also hint at the possibility of variations in prevalence based on geographic regions.
The seroprevalence of Syphilis among the donors was 6.4%. This Syphilis rate corresponds closely with the findings from Hohoe Municipality (5.2%). 12 However, this outcome is comparatively lower than the prevalence documented in Libreville, Gabon, (8.4%), 22 and Equatorial Guinea (21.5%). 29 However, when compared with other studies, this finding showcases a relatively higher prevalence. For example, a study carried out in Ibadan, Southwest Nigeria, reported a much lower prevalence of 1.3%. 30 Similarly, in Aïoun, Mauritania, another study demonstrated a prevalence of 3%. 31 The disparities in the prevalence of Syphilis across different studies could be attributed to variations in geographic locations, population demographics, healthcare infrastructure, awareness campaigns, and preventive measures in place. 15 The differences might also arise from the accuracy and reliability of the testing methods used in different studies. Implementing educational programs that raise awareness about Syphilis, its transmission, and prevention, and ensuring that testing for Syphilis is easily accessible and affordable are some measures that can help reduce the high prevalence of Syphilis reported in this current study.
Gender distribution among the donors revealed a notable prevalence of males, constituting 88.8% (5627), whereas females made up 11.2% (712). All four TTIs exhibited a considerable difference in prevalence when analyzed between males and females. Similar patterns were observed in studies conducted in the Offinso-North District, 15 Ho Municipality 21 and Hohoe Municipality of Ghana. 12 The reasons for donating blood tend to diverge between the 2 genders. Females often donate blood out of altruistic motivations, driven by a desire to help others. Conversely, males engage in blood donation for both altruistic reasons and the potential for monetary compensation. 32 These dual incentives, incorporating both altruism and financial benefits, appear to attract more male donors who are open to compensation. 12 Moreover, males also encounter various risk factors for TTIs due to their wider exposure to certain environments. In contrast, women are often confined to domestic settings. This disparity in exposure likely contributes to the notably higher prevalence of Syphilis among males. 12
The distribution of TTIs across different age groups revealed that young individuals constitute the largest portion of blood donors. Among these age groups, those aged 20 to 49 years had the highest prevalence of TTIs. This aligns with the findings of studies conducted at Hohoe Municipality and Offinso-North District in Ghana, which also showed that a significant number of blood donors fall within the 20- to 49-year age range.12,15 In the present study, donors aged 50 years and above had comparatively lower infection rates for various TTIs. This trend reflects their reduced exposure to the most common modes of TTIs often associated with a decrease in sexual activities within this age group. However, considering the limited number of donors within the older age group, these results prompt the need for further investigations to thoroughly understand this relationship.
Trend analysis showed that the positivity rates of the screened tests were 31.4% in 2017, 13.8% in 2018, 20.4% in 2019, decreased to 9.5% in 2020, 9.6% in 2021 and increased to 11.7%. However, there are some differences between these current findings and the findings of other studies. Aliyo et al 7 reported a prevalence of TTIs of 4.26% in 2020, which is lower than the prevalence of 9.5% reported in the current study for the same year. Also, the study by Leitch et al 33 showed an overall decrease in the prevalence of TTIs from 5.1% in 2015 to 5.8% in 2018. In contrast, the current study showed an increase in the prevalence of TTIs from 9.5% in 2020 to 11.7% in 2022. A possible reason for the differences in the trends could be that the studies were conducted in different populations. Blood donors in different countries and regions may have different risk factors for TTIs, due to differences in factors such as sexual behavior, drug use, and access to healthcare. Another possible reason for the differences is that the studies may have used different methods to collect and analyze data. For example, some studies may have used different screening tests for TTIs, or different criteria for defining a case of TTI. HIV, HBV, and HCV can have serious health consequences, including liver disease, kidney disease, and cancer. TTIs can also be transmitted from pregnant women to their babies, leading to birth defects and other health problems.34,35 The fluctuating trend in the prevalence of TTIs among blood donors is a concern, as it suggests that there is a need for continued vigilance and monitoring. Possible solutions to curb the problem of TTIs among blood donors include, increasing awareness of TTIs and their risks among blood donors and the general public. Another solution could be to strengthen screening and testing for TTIs among blood donors. Finally, it is important to promote safe sexual practices and other preventive measures to reduce the risk of TTIs.
The study employed logistic regression to analyze the factors influencing TTIs. However, due to the limited number of sociodemographic variables considered (only age and sex) and the specific focus of the study, a comprehensive analysis in this regard was not extensively discussed. Nevertheless, the study yielded meaningful insights. Notably, individuals aged 20 to 29 exhibited a higher likelihood of HBV infection compared to their other counterparts. This aligns with findings from Nlankpe et al, 36 where they discovered a similar association in the northern region of Ghana. Similarly, donors aged 20 to 29 were also found to be more prone to HCV infection. Furthermore, individuals aged 40 to 49 showed an increased likelihood of being infected with Syphilis. Likewise, this age group demonstrated a higher probability of HBV and HCV infections. The higher prevalence of HBV, HCV, and Syphilis among relatively older donors in this study implies that many of these donors might have been infected earlier in their lives, highlighting the importance of early interventions and continued awareness campaigns.
In terms of gender, male donors were observed to have twice the likelihood of HCV infection compared to their female counterparts. This observation is consistent with a study conducted in Ethiopia, 37 which found a slightly higher HCV rate among males compared to females. Additionally, male donors displayed a greater likelihood of Syphilis infection compared to female donors. This finding resonates with the results obtained by Adu-Poku et al 12 and Banong-le et al 38 in Ghana. The lower likelihood of female donors being infected with Syphilis could be attributed to the availability of accessible and cost-effective treatment for this infection. Females who contract the disease are more likely to be identified and treated during routine antenatal care visits, contributing to the reduced prevalence compared to male donors.
Limitations
The limited sociodemographic variables concept in this study, namely gender and age, restricted our ability to explore additional determinants of these TTIs and identify potential confounding variables. A more comprehensive analysis involving various factors could offer a clearer understanding and aid in the development of effective strategies for preventing these TTIs among blood donors in VRH. Additionally, the inability of this study to differentiate between various types of donors—such as paid donors, voluntary donors, family donors, and first-time or repeat donors—limits our ability to draw nuanced conclusions. Each of these donor categories presents different risk profiles for TTIs, and not being able to account for these distinctions could potentially impact the accuracy and applicability of our findings. This underscores the need for future research to consider these factors for a more comprehensive understanding of the prevalence and risk factors associated with TTIs among different donor groups in VRH.
Conclusion
The overall prevalence of TTIs in this current study is high. Nevertheless, a noteworthy observation is that males display a higher prevalence of HBV, HCV and Syphilis, while all types of TTIs are most prevalent among adults. It is imperative to take measures that encourage and boost female donor participation, as our study highlights a scarcity of female donors. Equally essential is the need to raise awareness among the general population, particularly young adults, about safe practices to effectively prevent TTIs. Targeted prevention strategies and interventions should also focus on male donors, given their higher prevalence of TTIs.
Footnotes
Acknowledgments
The administration of the Volta Regional Hospital
Authors’ Contributions
PYH and EET conceptualized and designed the study; GAV and EB analyzed the data; PYH collected the data; EB and EET supervised the data collection; PYH, GAV, MH, NK, and EET led the writing of the manuscript; EET, MN, and NK critically reviewed the manuscript; all the authors read and approved the final version of the manuscript.
Data Availability
The datasets used for the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval was obtained for the current study from the University of Health and Allied Sciences Research Ethics Committee (UHAS-REC) with approval number UHAS-REC A.10 [124]22-23. Permission to conduct the study was also obtained from the institution where data were collected. The blood donor register provided the data, which were kept completely confidential and disclosed to no other person. The study had no written consenting process since there was no human interaction but rather blood donors’ records in the blood donors’ register.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.