
Abstract
Background
Lack of index case testing increased the risk of contracting HIV among the families of index clients, partners, and biological children. The aim of this study was to determine the prevalence of index case HIV testing uptake and its associated factors at Oromia, Ethiopia.
Methods
An institutional-based cross-sectional study was conducted. A face-to-face interviewer administered structured questionnaire and chart review checklist were used to collect data. The data were analyzed using SPSS version 25. Logistic regressions were executed and statistical significance was declared at P < .05.
Results
The prevalence of index case testing was 80.2%. Factors associated with index case HIV testing uptake included HIV status disclosure (AOR = 5.4, 95% CI: 2.1, 14.0), discussed about HIV with family (AOR = 3.1, 95% CI: 1.2, 7.5), counseling of the index case (AOR = 3.3, 95% CI: 1.7, 10.6), perceived benefit of the index case tested (AOR = 3.2, 95% CI: 1.5, 8.7), being on ART 12 months or more (AOR = 2.6, 95% CI: 1.1, 6.1), and maintained privacy (AOR = 3.1, 95% CI: 1.3, 7.1).
Conclusions
The uptake of index case HIV testing was moderately high. Additionally, factors such as HIV status disclosure, discussion of HIV with family, counseling of the index case, perception of the benefits of HIV testing for the index case, duration of clients on ART, and privacy maintenance during service delivery were significantly associated with index case HIV testing. To enhance index case testing, it is crucial to raise awareness and ensure client privacy during the initial HTC visit. Encouraging HIV status disclosure through discussion and promoting adherence to HIV medication is also recommended.
Introduction
Since the Human Immunodeficiency Virus (HIV) is of public health importance, different strategies have been implemented to control the epidemic. In 2014, the United Nations Programme on HIV/AIDS (UNAIDS) set targets aimed at ending the AIDS epidemic by 2030. 1 Different countries, including Ethiopia, have introduced index case testing services, which are a potentially high-yield, population-targeted testing approach for identifying and linking new HIV individuals to treatment services. 2 Index case HIV testing is a case-finding approach that focuses on eliciting the family, sexual partner, and biological children of HIV-positive individuals and offering HIV testing services (HTS). 3 Index testing, also known as assisted partner notification services, involves offering HTS to sexual partners, drug-injecting partners, or biological children of people living with HIV (PLHIV) in a safe and ethical manner.3,4
The index case testing services program demonstrated a positivity yield that was much higher (35%–62%) than prior passive testing modalities. 3 Additionally, it is effective in increasing the detection and testing of sexual partners and biological children of people contracting HIV. 5 The index case HIV testing in turn contributed to high rates of HIV status disclosure, partner tracing, and partner testing.6-8 Various studies have also shown that index case HIV testing is acceptable, feasible, and costless.9-11
Globally, more than 38.4 million people were living with HIV, and more than 1.5 million people had newly acquired HIV in 2021. Nearly 45% of the people newly infected with HIV live in Eastern and Southern Africa. 12 In Ethiopia, the epidemic is primarily concentrated in certain populations and mixed. However, with an estimated 618,000 PLHIV, of whom 40,528 were less than 15 years of age, the national adult HIV prevalence was 0.93%, along with the highest 4.45% in Gambella, the lowest 0.16% in Somali regions, 2.9% in urban areas, 0.4% in rural areas, 1.2% in females, and 0.7% in males. In the Ilu Ababor zone, the prevalence was 0.6%.13,14
According to the WHO report, about 19% of the PLHIV were unaware of their status, and in numerous settings, HTS were not adequately focused. 15 Globally, every day, 4000 people, including 1100 young people, are infected with HIV. If existing trends continue, 1.2 million people will be newly infected with HIV in 2025, three times more than the 2025 target of 370,000 new infections. 16 Consequently, families of index clients, partners, and biological children are at increased risk of contracting HIV.3,4,17
The 20 countries of the Center for Disease Prevention and Control (CDC) report demonstrated that of nearly two million persons tested, 5.8% were reported as HIV-positive. In Ethiopia, specifically, the report showed 117,731 index cases were tested, and 3.5% of people were identified as HIV positive. 18 Yet, the UNAIDS global report showed that more than half of new HIV infections occur among key populations (KP) and their sexual partners.16,19 However, the uptake of index case testing in key populations is very low and has many barriers, as observed from studies done in some African countries.20,21
Studies conducted so far showed that the prevalence of index case testing ranged from 12% to 86%, 5 along with previously identified factors such as gender, level of education, HIV status disclosure, months on ART, referral method, and place of HIV testing.18,22-24 However, there is limited data that addresses factors associated with index case testing, including the key population, counseling on index case HIV status disclosure and its benefits, and protecting privacy at initial HTC visits. In healthcare settings, screening for HIV using partner testing to identify high-risk individuals was mainly based on their contacts. 25 However, adults tend to be tested at voluntary counseling and testing (VCT) centers, and other service delivery points where providers may not be fully aware of the importance of index case testing. 26 A few studies conducted in Ethiopia showed that most of the index clients were first tested by provider-initiated HIV testing and counseling (PICT) rather than index case testing. 25 Thus, the aim of this study was to determine the prevalence of index case HIV testing uptake and its associated factors in Oromia, Ethiopia.
Method
Study Setting and Period
An institutional-based cross-sectional study was conducted from June 21 to July 20, 2023, at the Mattu Karl Comprehensive Specialized Hospital (MKCSH). Mattu, an administration town in the Ilu Ababor zone of Oromia Regional State, is located in the south-west, 600 kilometers away from Addis Ababa, the capital city of Ethiopia. The MKCSH provides different inpatient and outpatient comprehensive services to the population in the surrounding Ilu Ababor zone, Sheka zone (South Western Region of Ethiopia), and Gambella region, with a catchment population of 3.6 million. The hospital has been providing antiretroviral therapy (ART) services for free since 1998. Currently, 1740 clients are taking ART at the hospital.
Population
All PLHIV currently receiving ART regularly at the ART clinic of MKCSH were source population, whereas randomly sampled PLHIV currently receiving ART at the ART clinic of the MKCSH during the study period were study population. PLHIV aged 18 years or older were included in the study, and PLHIV who were seriously ill or unable to respond to the questionnaire during the data collection period were excluded from the study.
Sample Size Determination
The sample size was calculated using Epi Info 3.7.1 software, assuming a prevalence of index case testing of 49.3% taken from the study conducted in Kule, 27 a 95% confidence level, and a 5% margin of error. Thus, the sample size was 315. However, by adding a 10% non-response rate, the final sample size was found to be 347.
A simple random sampling technique was used to select the study participants until the total sample size was reached.
Operational Definition
Family testing uptake: partner or children < 15 years of age tested for HIV. 27 Index client: newly diagnosed HIV positive individual and/or HIV positive individual already enrolled in HIV care. 3
Knowledge of HIV: good knowledge if a participant correctly responds to ≥7 or more questions, moderate knowledge if correctly answered 5–6 questions, and poor knowledge if correctly answered <5. 28
Data Collection Tools
Data collection tools were adapted from different related studies.27,29,30 It contains four components, namely sociodemographic, health and family-related, knowledge-related, and health facility-related components. An interviewer-guided structured questionnaire and chart review checklist tools were used to collect data. The chart review checklist was used for months on ART, preferred referral, time to testing of index contacts, and HIV testing entry point variables. Two bachelor of science nursing professionals and one bachelor of science public health officer professional collected and supervised the data collection. An exit interview was done in a private area after participants took the service at the ART clinic. Training was given to both data collectors and supervisors by the principal investigator for two days. The questionnaire was initially prepared in English and translated by a language professional into the local language, Afan Oromo, and then translated back to English to check for comprehension and consistency. The questionnaire was refined and checked for completeness, accuracy, and consistency by the supervisors and investigators, and corrective action was taken with all the data collectors and supervisors on a daily basis.
Data Analysis
The collected data were coded, cleaned, checked, and entered into the computer using EpiData version 4.6. Then, it was exported to SPSS version 25.0 for analysis. Categorical variables were described using frequency and percentage, whereas continuous variables were described by means with a standard deviation. Both bivariable and multivariable logistic regression analyses were performed. The variables with a P-value <.05 were considered statistically significant and adjusted odds ratios were used to report the strength of the association with a 95% confidence interval. The Hosmer–Lemeshow statistic declared the fit of the model (P = .961).
Ethics Approval and Consent to Participate
The study was approved by the Ethical Review Board of College of Health Science of Mattu University Ref. No/RPG/293/23. A written informed consent was obtained from all study participants.
Results
Sociodemographic Characteristics of the Respondents
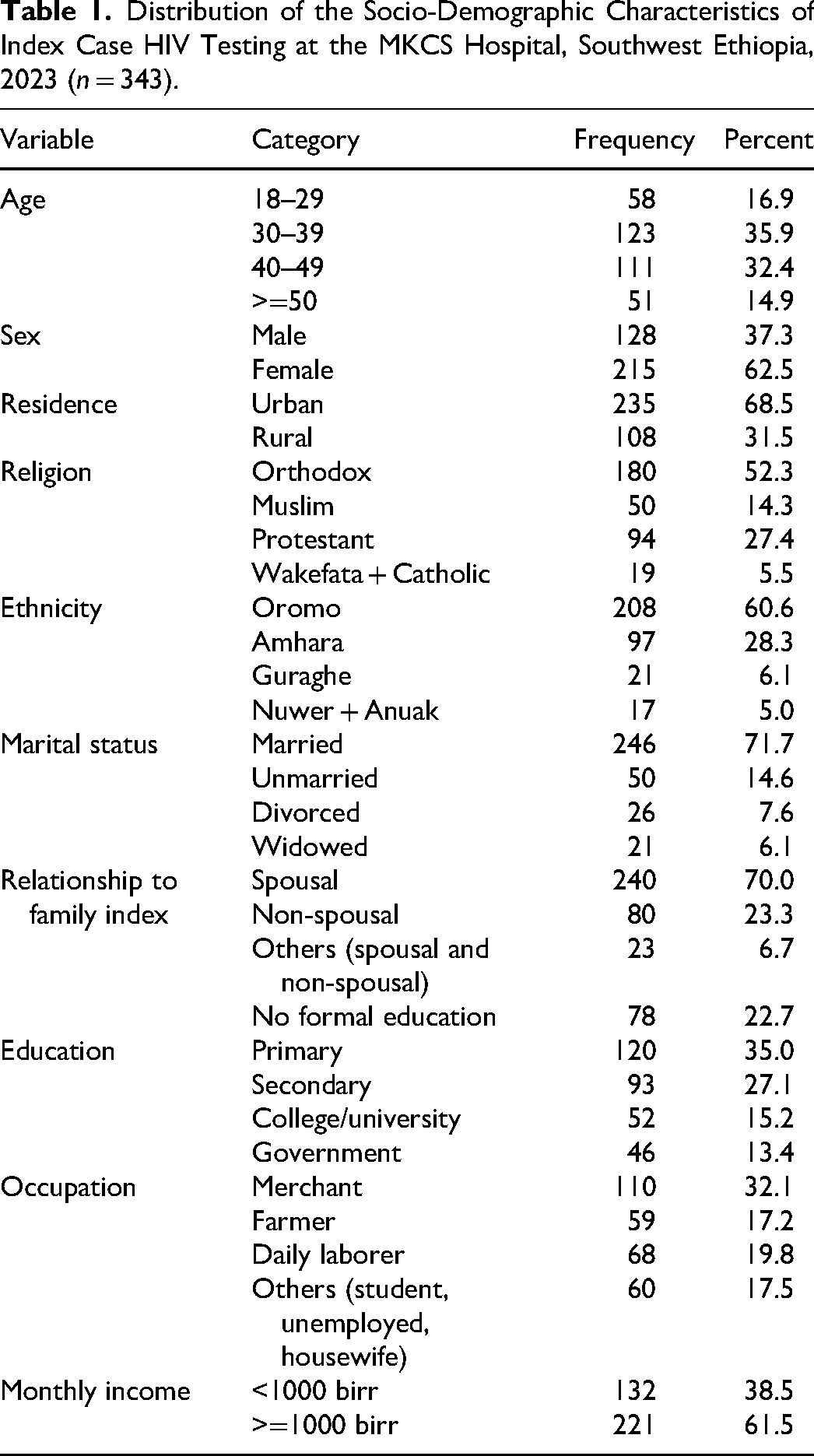
Three hundred forty-three respondents participated in the study, with a response rate of 98.8%. The mean age of respondents was 39.14 ± 10.13 SD years. The majority of respondents were Oromo, followed by Amhara (Table 1).
Distribution of the Socio-Demographic Characteristics of Index Case HIV Testing at the MKCS Hospital, Southwest Ethiopia, 2023 (n = 343).
Health and Family Related Characteristics of the Respondents
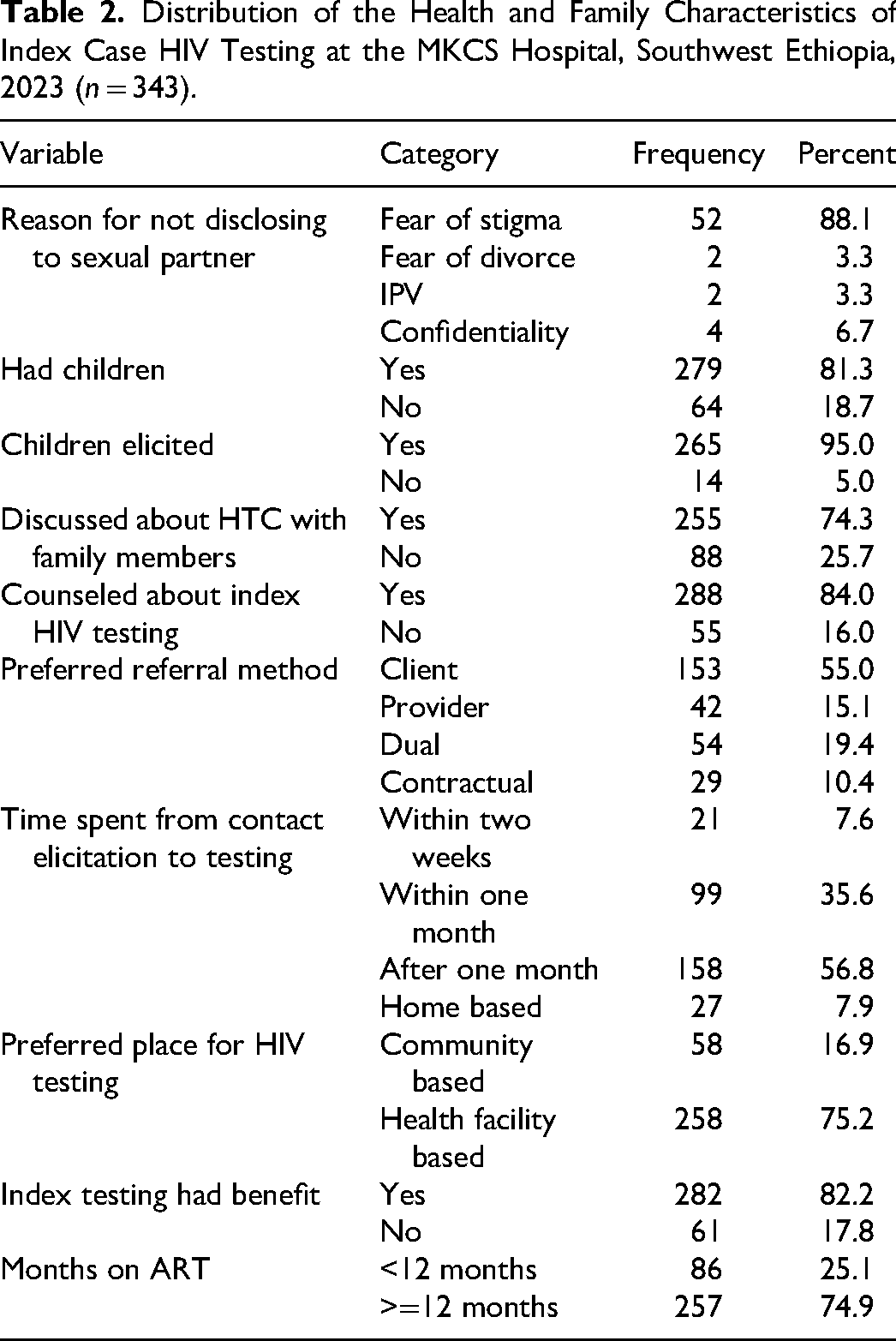
Generally, about 284 (82.8%) respondents disclosed their HIV status to their 234 (82.4%) partners, 9 (3.2%) parents, 19 (6.7%) own children, 7 (2.5%) brothers/sisters, and 15 (5.3%) others (relatives and/or neighbors). More than nine out of ten 317 (92.4%) respondents had sexual partners. Out of them, 295 (86%) were elicited for HIV testing of their sexual partners and about 7% (21) experienced intimate partner violence (IPT). Less than one-tenth 29 (8.5%) participants belonged to the key populations. Of them, only 7 (24.1%) key population contacts were tested for HIV. The reason why key population contacts were not tested for HIV was that 13 (59.1%) partner addresses were not known and 9 (40.9%) did not live together (Table 2).
Distribution of the Health and Family Characteristics of Index Case HIV Testing at the MKCS Hospital, Southwest Ethiopia, 2023 (n = 343).
Health Facility Related Characteristics
About half of the respondents HIV testing entry points (169, 49.3%) were by PICT, followed by 80 (23.3%) self-referral, 61 (17.8%) ICT, and lastly, 33 (9.6%) KP clinics. More than nine-tenths of 320 (93.3%) respondents were initially enrolled in health facility-based testing, whereas 23 (6.7%) were enrolled in community-based testing. About 279 (81.3%) respondents’ privacy was maintained at the initial HCT visit.
Prevalence of Index Case HIV Testing Uptake
The prevalence of index case HIV testing uptake of PLHIV currently receiving anti-retroviral therapy at the Mettu Karl Comprehensive Specialized Hospital was 275 (80.2%) with a 95% CI of [75.9, 84.4].
Factors Associated With Index Case HIV Testing
The bivariable analysis showed that variables such as having HIV status disclosure, having under 15-year-old children, belonging to a key population, index case HIV testing counseling, HIV testing discussion with family members, family index case testing benefit, privacy, knowledge, and months stayed on ART were candidates for multivariable logistic regression at a P-value <.25. Furthermore, the multivariable analysis revealed that HIV status disclosure, index case HIV testing counseling, HIV testing discussion with family members, family index case testing benefit, having privacy, and months stayed on ART were significantly associated with family index case HIV testing uptake at a P-value <.05 (Table 3).
Factors Associated With Index Case HIV Testing at the MKCS Hospital, Southwest Ethiopia, 2023 (n = 343).
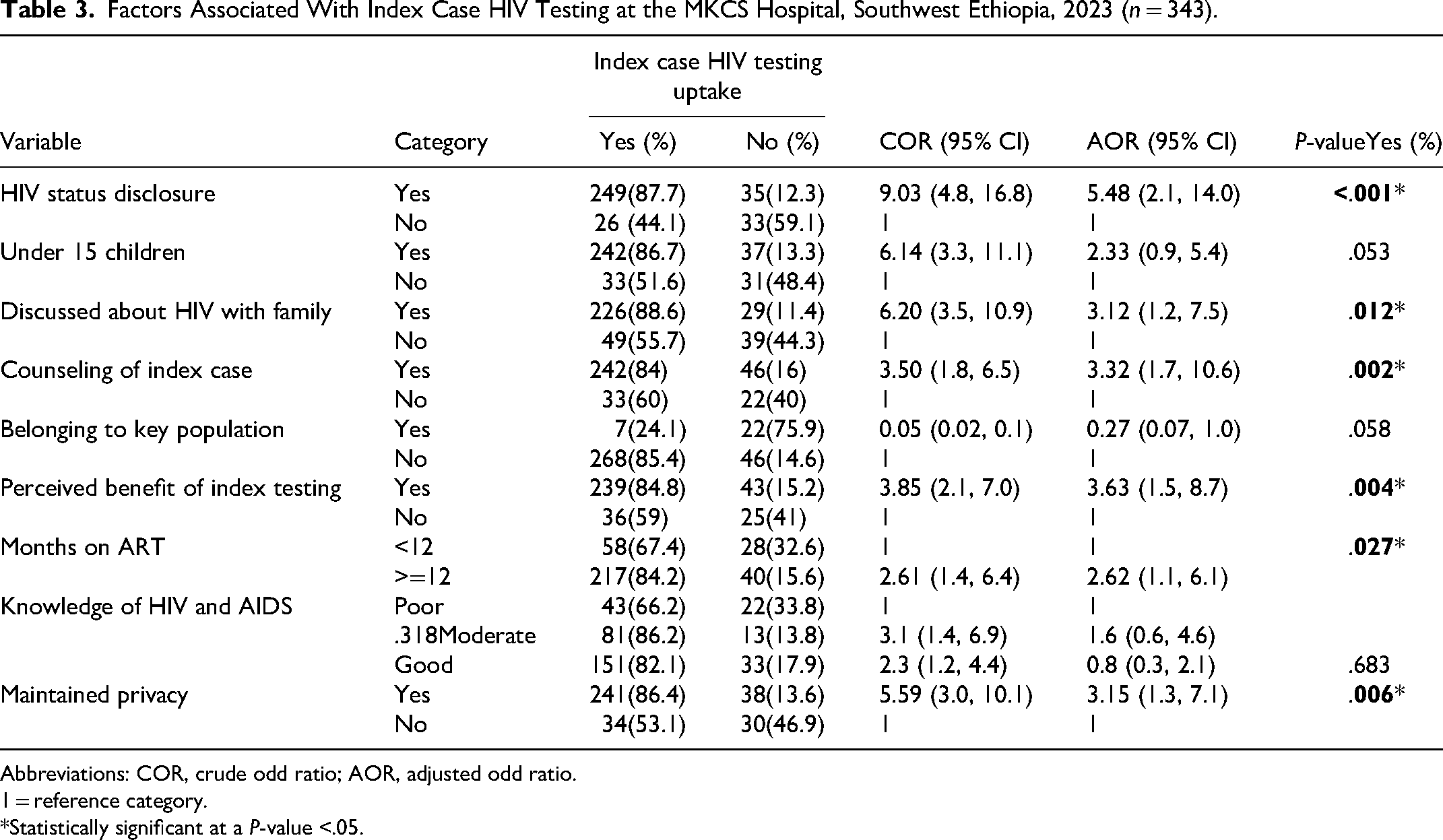
Abbreviations: COR, crude odd ratio; AOR, adjusted odd ratio.
1 = reference category.
*Statistically significant at a P-value <.05.
Discussion
This study revealed that the prevalence of index case HIV testing uptake was 80.2%. This finding is higher than that obtained in studies conducted at Kule, Ethiopia: 49.3%, 27 Kenya: 70%, 31 and Zimbabwe: 60%. 32 The potential reasons for this difference might be socioeconomic variances among the study population, study setting, the period when the initiative started in the corresponding countries, and the time of the study. For example, the result of this study is higher than that of a study conducted in Kenya and Zimbabwe. This could be due to the index cases offered in the facility and community-based testing, where most index clients choose facility testing over community testing. However, biological children were more likely to be tested when community testing was preferred. The result of the study is also higher than that of the study conducted among adults attending ART clinics in the Kule refugee camp, Southwest Ethiopia. This might be due to the dissimilarity between the study population and the study conducted in Southwestern Ethiopia at the Kule Refugee Camp, where HIV testing might be less of a priority issue, where there were inadequate healthcare services, and where fewer skilled health workers were available in such special population settings. Consequently, the findings of this study indicate that there is progress in the implementation index case HIV testing in this area.
However, the prevalence of this study is lower than the finding of Nekemte (85.2%) 29 and Woliso, Ethiopia (96%), 30 and Nigeria (98%) 20 and Tanzania (96%). 33 The possible justification for this difference might be due to sampling differences and study settings. In Nigeria, index cases were admitted patients; hence, index cases might be more cooperative to accept testing due to repeated counseling than in a study where index cases were on outpatient follow-up. In Tanzania, only new index clients diagnosed through VCT and PITC are enrolled as index clients. Since VCT is client-initiated testing, it is easier for them to bring their family for testing.
This study revealed that the odds of index case HIV testing were found to be higher among index cases who have disclosed their HIV status as compared to those who have secreted their HIV status. This finding is similar to a study conducted in Assosa, 34 Kule, 27 Nekemte, 29 and Woliso, Ethiopia. 30 The similarity might be due to the fact that index clients assisted in the elicitation of information about sexual partners and provided education on the benefits of early therapy and a better outcome. Additionally, recurrent discussion about HIV testing uptake and counseling, as revealed in this study, from the health care providers during their follow-up visits, both for status disclosure and for index testing, is expected in HIV prevention and reduction measures. These raise awareness about the risk of transmitting infections to sexual partners and their children and encourage the need for testing.
This finding showed that the odds of index case HIV testing were higher among index cases who discussed HIV testing with family members. This was similar with studies conducted in Kule refuge Ethiopia, 27 and Uganda. 35 The possible reason for this similarity is that discussion about testing creates a favorable environment for the index client to bring their families for testing and is a requirement for tracking family members for testing.
In this finding, respondents who had been on ART for 12 or more months were more likely to test their partner and/or children compared to respondents who had been on ART for less than 12 months. The finding is consistent with a study conducted at 27 Nekemte 29 and Woliso, 30 Ethiopia. Additionally, it agrees with a study conducted in Cameroon, 36 Kenya, and Uganda. 37 The justification for this might be due to the removed barriers to the initiation of HIV treatment and retention of care. As clients have been on ART, it is typically anticipated that their level of awareness of HTC will rise. As a result, the likelihood of telling family members about their status increases, making family testing easier. On the other hand, among recently enrolled clients, high self-perceived stigma and discrimination make them isolated.
In this study, the perceived benefit of index case HIV testing is significantly associated with index case HIV testing. This finding is consistent with the studies conducted in Nekemte, Ethiopia 29 and Uganda. 31 This might be due to the fact that it leads to early initiation into HIV care and treatment, reducing the risk for discordant couples.
This study also shows that those participants who received counseling on index case testing were higher than those who do not counseled. This finding was supported by a study conducted in Assosa, Ethiopia. 34 It could be due to the ongoing counseling that helps the client cope with the emotions that arise from the test result, understand the possible transmission to family, and encourage family testing.
Furthermore, this finding revealed that participants whose privacy was maintained were more likely to test index cases as compared to those whose privacy was not maintained. This finding agrees with the study in Tanzania. 38 This implies that if the privacy of clients is maintained, they will believe in health workers, be confident in the service they are receiving, and have improved self-esteem in living with chronic conditions that contribute to high partner elicitation and testing.
The strength of the current study is that it is the first of its kind in the study area. It tried to show tested index cases in a high catchment area and identified numerous predictor factors. The study also has some limitations. It is the cross-sectional study design, which does not allow establishing cause-and-effect relationships. It was also prone to selection, social desirability, and recall biases.
Conclusions
The uptake of index case HIV testing was moderately high. Additionally, factors such as HIV status disclosure, discussion of HIV with family, counseling of the index case, perception of the benefits of HIV testing for the index case, duration of clients on ART, and privacy maintenance during service delivery were significantly associated with index case HIV testing. To enhance index case testing, it is crucial to raise awareness and ensure client privacy during the initial HTC visit. Encouraging HIV status disclosure through discussion and promoting adherence to HIV medication is also recommended.
Footnotes
Acknowledgments
The authors would like to extend their thanks to the Mattu University College of Health Science and study participants.
Author Contributions
DK conceived the research study; designed the research methods; and led the acquisition, analysis, and interpretation of data. MAH contributed to the analysis and interpretation of data and the writing and revising of this article. BMTK participated in drafting, interpreting the data, and supervising the whole activity. ZA participated in interpreting the data and supervising the whole activity. EC participated in the interpretation of data, drafting, and supervising the whole activity. All authors read and approved the final manuscript.
Availability of Data and Materials
Data are available upon request from the corresponding author.
Consent for Publications
All authors approved for publication and agreed to be accountable for all aspects of the work related to accuracy or integrity.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.