
Abstract
Uptake of PrEP remains suboptimal, especially in the Southern United States. Same-day or “Rapid PrEP Initiatives” (RPIs) in sexual health centers (SHCs) could facilitate access and overcome barriers to PrEP. We studied the adaptation of an RPI from Denver, Colorado to an SHC in New Orleans, Louisiana. Through focus group discussions (FGDs) with local SHC staff and PrEP providers, we developed a preliminary RPI model. In 5 FGDs with SHC clients referred for or taking PrEP, we gathered adaptation recommendations and feedback on model acceptability, feasibility, and utility. Providers and clients voiced unanimous support for the RPI. Clients favored the ease of same-day PrEP initiation and emphasized a desire for navigational support, financial counseling, and integration of PrEP care with their other clinical needs. Clients recommended that SHC providers discuss PrEP and HIV with all patients, regardless of providers’ perception of risk. Next steps include small-scale implementation and evaluation.
Plain Language Summary
Uptake of PrEP remains low, especially in the Southern United States. Same-day or “Rapid PrEP Initiatives” (RPIs) in sexual health centers (SHCs) could facilitate access and overcome barriers to PrEP. RPIs provide eligible clients with an opportunity to start PrEP on the same day they receive screening for sexually transmitted infections. We studied the adaptation of an RPI from Denver, Colorado, to an SHC in New Orleans, Louisiana. Through focus group discussions (FGDs) with local SHC staff and PrEP providers, we developed a preliminary RPI model. In five FGDs with SHC clients referred for or taking PrEP, we gathered adaptation recommendations and feedback on RPI model acceptability, feasibility, and utility. Providers and clients voiced unanimous support for the RPI. Clients favored the ease of same-day PrEP initiation and emphasized a desire for navigational support, financial counseling, and integration of PrEP care with their other clinical needs. Clients recommended that SHC providers discuss PrEP and HIV with all patients, regardless of providers' perception of risk. Next steps include small-scale implementation and evaluation.
Introduction
HIV pre-exposure prophylaxis (PrEP) is a highly effective yet underutilized method of HIV prevention. 1 Although it has been more than 10 years since its initial approval by the United States Food and Drug Administration (FDA), PrEP is prescribed for only a quarter of Americans eligible. 2 Moreover, PrEP is not reaching Americans with the highest rates of new HIV diagnoses, particularly people of color living in the Southern United States.3-6 Although more than half of all new HIV diagnoses in the United States occur in the South, 7 it has the lowest PrEP-to-need ratio (ie, number of PrEP users divided by new HIV diagnoses) of all regions.8,9 PrEP stigma, limited awareness, cost of use, and low perceived accessibility are barriers that have been noted to contribute to inadequate PrEP uptake.10-15
Same-day PrEP counseling and initiation at sexual health centers (SHCs) is a potential solution to overcome some of these barriers. In a traditional PrEP referral system, patients are referred to a PrEP provider at their initial appointment and then must schedule and attend this subsequent appointment to receive PrEP counseling, complete necessary labs, and wait until lab results are back before receiving a prescription. Same-day PrEP initiation consolidates counseling, labs, and prescription provision to the same day that clients present for care. Amidst elevated rates of sexually transmitted infections (STIs) nationally, 16 SHCs are well situated to facilitate increased PrEP awareness and initiations at the point of care by offering streamlined PrEP access to individuals who may be at higher risk for HIV. 17
Same-day PrEP prescribing has been identified by the Centers for Disease Control and Prevention (CDC) as a strategy to improve PrEP access and reduce patient burden, and the CDC now offers guidance on how to offer same-day PrEP in order to safely shorten time to PrEP initiation. 18 Rapid or same-day PrEP initiation protocols have been successfully established in select clinics across the country, demonstrating that it can be a safe and effective way to prescribe PrEP.17,19-26 However, these programs have not been widely implemented, and limited acceptability or feasibility data have been collected from patients and providers.19,23,24
Prior work on PrEP referrals from our SHC, part of a Federally Qualified Health Center (FQHC), in New Orleans, Louisiana, demonstrated that PrEP referrals from the SHC to a PrEP clinic co-located in the same building resulted in a PrEP initiation visit for fewer than half of the clients referred. 27 Clients referred for PrEP were less likely to attend an initial PrEP appointment if they did not receive in-person service facilitation by a PrEP navigator, were uninsured, or were heterosexual 27 ; these findings demonstrate the need to improve PrEP initiation systems to reduce attrition. Thus, we adapted a model implemented by the Denver Rapid HIV PrEP Program 19 to meet the unique needs of local providers and clients in New Orleans, an Ending the HIV Epidemic initiative priority jurisdiction. 28 Through focus groups discussions (FGDs) with SHC clients, we gathered feedback, concerns, and suggestions for implementing the Rapid PrEP program at our SHC, located in a zip code with an HIV prevalence of more than 4%. 29 The objective of this study was to determine patient-centered priorities for adapting the Rapid PrEP model. Here we describe the results of FGDs with SHC clients.
Methods
Study Design
We applied the ADAPT-ITT process model (Assessment, Decision, Administration, Production, Topical experts—Integration, Training, Testing), a framework for adapting evidence-based HIV interventions, 30 to the Denver PrEP program 19 to inform development of the New Orleans Rapid PrEP Initiative (RPI). Investigators and the Denver team (“topical experts”) first identified core components of the Denver program (Table 1), that is, processes to ensure same-day PrEP services can be feasibly administered.
Denver Rapid PrEP Core Components.
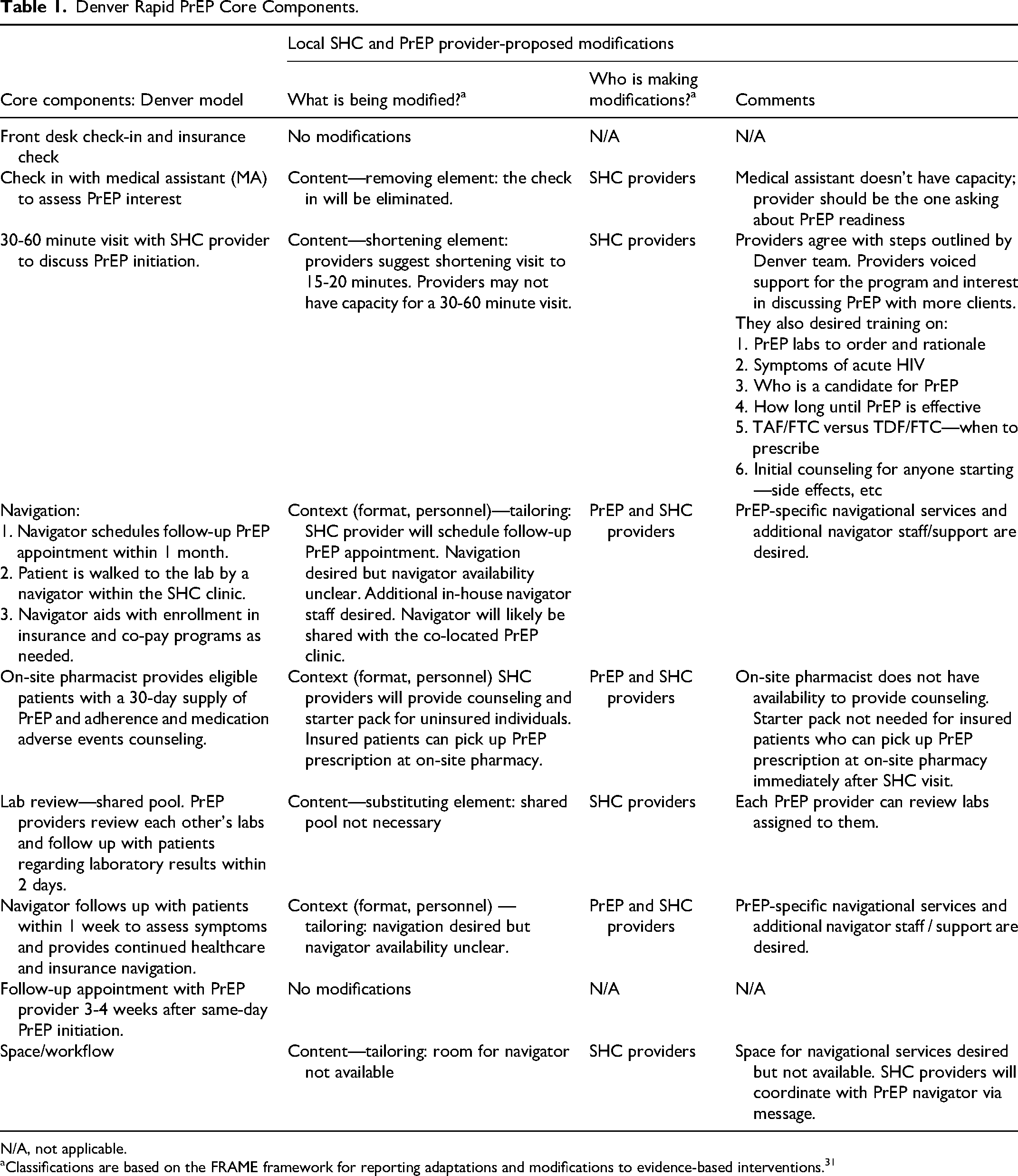
N/A, not applicable.
Classifications are based on the FRAME framework for reporting adaptations and modifications to evidence-based interventions. 31
As part of the initial “Assessment” phase of ADAPT-ITT, investigators conducted FGDs with staff (“local stakeholders”). One FGD was conducted with 4 SHC clinic staff and a second FGD was conducted with 5 PrEP providers. Clinic personnel participating in the FGDs proposed modifications to the Denver Model, mostly related to reassignment of tasks due to limitations in personnel and capacity (Table 1), and, together with investigators, they developed a preliminary model for adapting the RPI to the SHC (Figure 1).
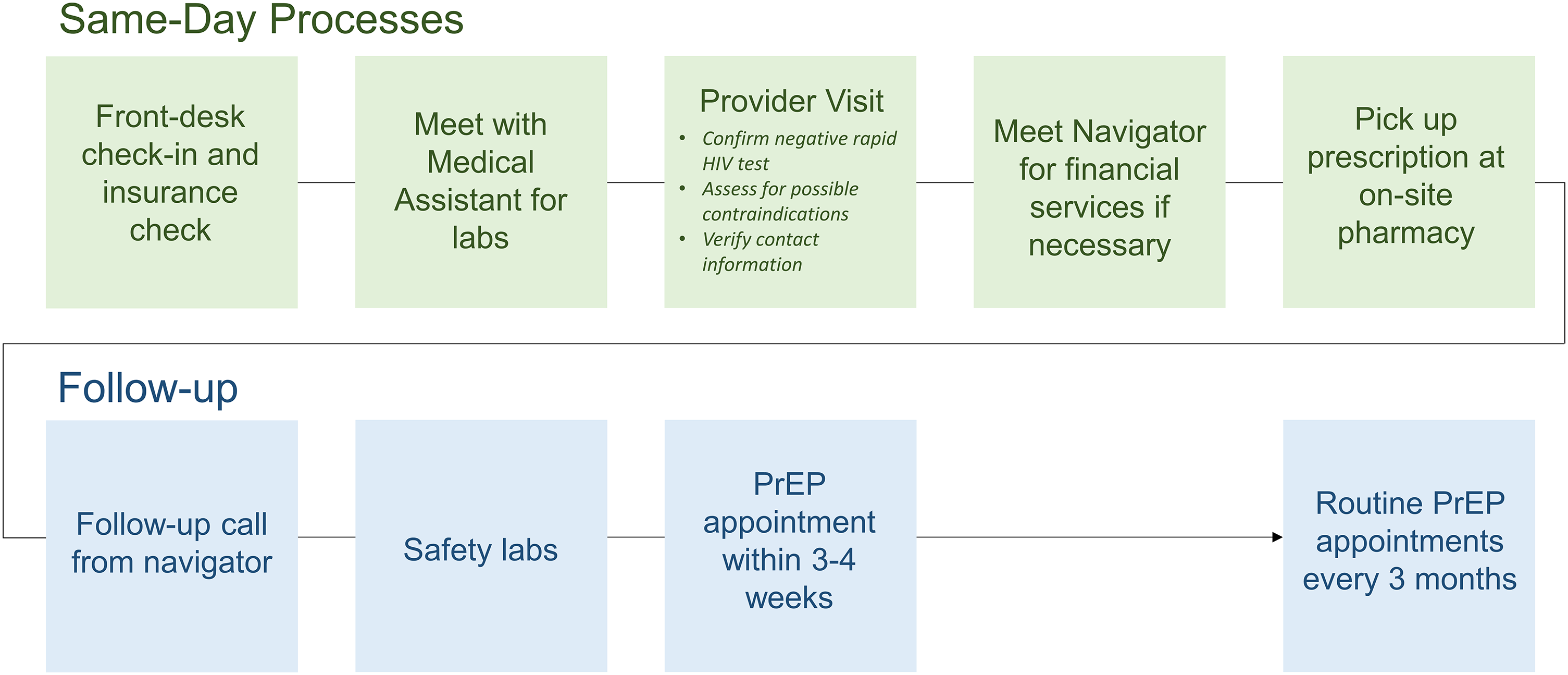
Rapid PrEP initiation model.
Following FGDs with staff, the researchers conducted 5 FGDs with SHC clients, the “target population.” In the client FGDs, researchers presented the preliminary RPI model to participants to gather feedback on the acceptability, feasibility, and utility of the implementation plan and gathered suggestions for further adaptation. The data saturation point was reached after the fifth FGD. This is a qualitative descriptive study. 32 The study was conducted and reported in compliance with the consolidated criteria for reporting qualitative research (COREQ). 33 Additional information based on the COREQ checklist is provided in the Supplemental material (Supplement 1. COREQ checklist).
Participants
Participants were recruited from the SHC and were either receiving PrEP or had been referred for PrEP. Inclusion criteria were the following: age 18 years or older, self-reported HIV-negative status, eligibility for PrEP per CDC criteria, 18 and no medical history of chronic kidney disease or hepatitis B infection. FGDs were purposefully recruited to reflect the demographics of clients served by the SHC 27 and have a variety of demographic characteristics represented (eg one group of cisgender women of color, one group of gender-diverse participants).
Ethical Approval and Informed Consent
Study procedures were approved by the Institutional Review Board (IRB) of Louisiana State University Health Sciences Center—New Orleans (#1558). Permission to obtain verbal consent was requested and approved by the IRB. Verbal informed consent was obtained from each participant via phone call in advance of the online FGDs. Participants were provided with an information sheet which was reviewed by investigators before consenting. Investigators documented when verbal informed consent had been obtained for each study participant.
FGD Process
Each FGD included 4 to 7 participants and was conducted remotely on Zoom 34 by a trained moderator (MEC or AL). Participants had the option to keep video on or off, and all chose to keep video off. The moderator presented slides illustrating the RPI model (Figure 1) and asked questions outlined in the FGD discussion guide (Supplement 2. FGD Discussion Guide). FGDs lasted approximately 1 hour and were audio-recorded and transcribed. Participant names were masked with an anonymous pseudonym in the Zoom session and transcript. Following the FGD, participants completed a paper demographic questionnaire, including questions about PrEP history and interest (Supplement 3. Demographic Questionnaire). The FGD interviewer guide and questionnaire were not pre-tested and are included as supplements.
FGD Content
Each FGD began with a brief presentation of the preliminary model for adapting the RPI to the local SHC. Participants were invited to voice initial impressions and questions. Next, each core component of the RPI was presented, and participants were invited to share feedback on each component's acceptability, feasibility, and utility, suggest changes, and share general thoughts. Core components of the same-day model included the front desk check-in and insurance verification, the provider visit, laboratory assessments, navigational services, and pick-up of the prescription. The moderator described how the preliminary model for same-day PrEP services would fit into the clinic workflow, addressing follow-up processes as well.
Qualitative Analysis
Applied thematic analysis of the FGD transcripts was executed by 2 analysts using NVivo. 35 A structural codebook was developed based on the interview guide and was used independently by each analyst to code the transcripts. The structural codebook was iteratively refined through analysts’ discussion and re-applied independently until an inter-coder agreement of greater than 80% was reached. Following structural coding, analysts developed content sub-codes based on emergent themes emphasized by FGD participants. Analysts independently re-applied the revised codebook to the FGD with the greatest percentage of transcript coverage for each structural code. The codebook was revised and re-applied until inter-coder consensus was achieved.
Results
Demographic Characteristics
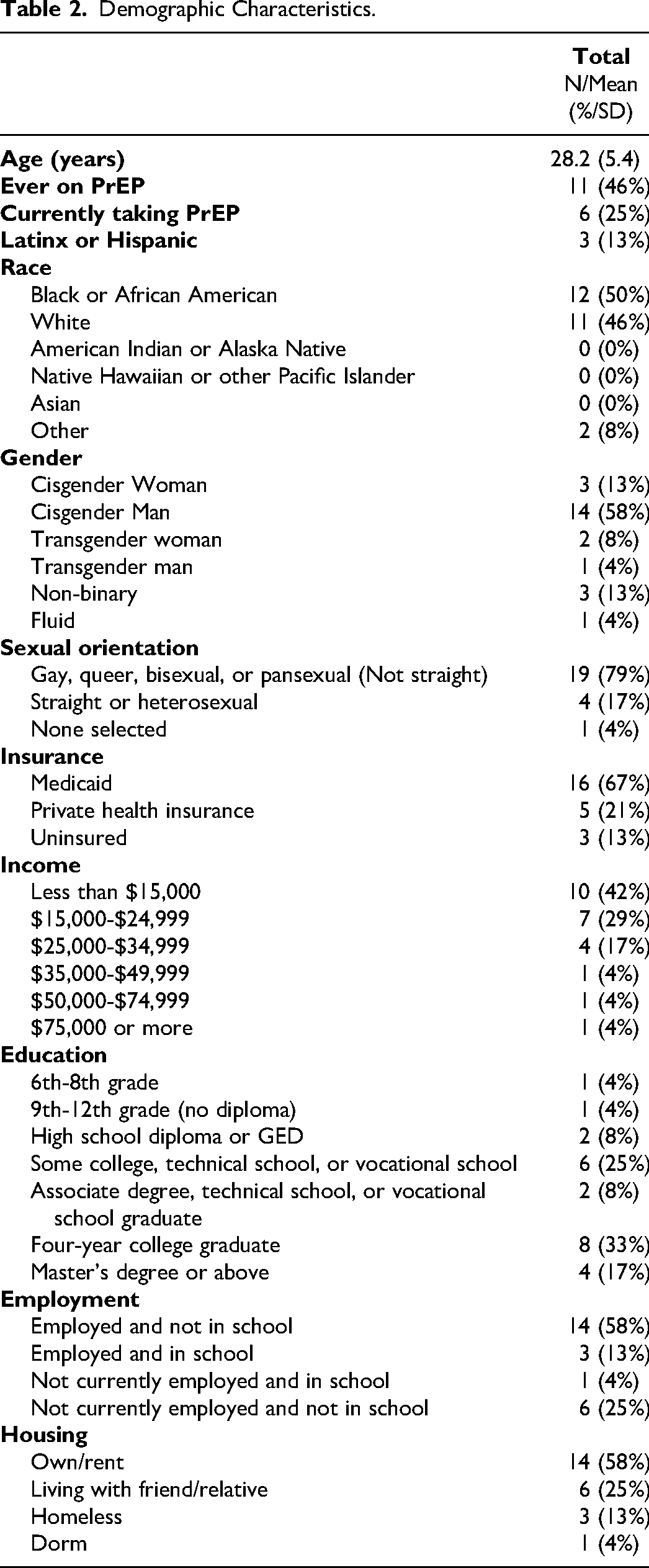
Of the 24 client participants, the mean age was 28 years, and most identified as gay, queer, bisexual, or pansexual (19, 79%). The majority (21, 88%) had an annual income of less than $35,000 and were on Medicaid (16, 67%). Housing status, employment, and education level varied across FGDs. Eleven (46%) had ever taken PrEP, including 6 currently taking PrEP. Demographic characteristics are shown in Table 2. No FGD participants who started an FGD dropped out or refused to participate.
Demographic Characteristics.
General RPI Impressions
Participants in all of the FGDs voiced support for implementing the RPI at the SHC. Participants expressed that the RPI would be time-saving compared to the current model of PrEP referrals from the SHC through eliminating the need for a separate appointment to initiate PrEP (when eligible for same-day initiation). Two participants had experienced same-day PrEP initiation in New York and shared that Rapid PrEP was “very effective” and more efficient than the referral model. When I moved to New Orleans, it took them almost a year to get me on PrEP. The whole thing was very drawn out, and unnecessary. But yeah, I kept thinking, why is it? When I went to New York, I went in to ask about it, and literally I went to the doctor and 45 min later, I was picking up my prescription and starting. And it's very effective, and they not only do that, but then they also vaccinate you for hepatitis, and all of that, the same week. It's very effective. They’re very adamant about just getting everything done that needed to be done. It was just very effective. —Speaker 4, FGD 4
Participants were optimistic about consolidating the steps to obtaining PrEP into fewer appointments and about the SHC provider writing the initial PrEP prescription. Participants noted that the RPI could reduce logistical barriers, such as difficulties with scheduling and attending subsequent appointments. One of the things that I think is really good about the Rapid PrEP for New Orleans, is that a lot of us here tend to be a little bit flaky. Or, when you minimize the number of times that we have to come back in to do things, I think it maximizes the likelihood that the medication will actually get to the people. —Speaker 1, FGD 4
One participant noted that the RPI could also reduce the financial burden of PrEP by reducing the number of appointments and co-pays. Participants also noted that the RPI could address psychological barriers, such as overthinking PrEP during the gap between the SHC visit and PrEP appointment. However, one participant voiced concern that the RPI model might not allow adequate time to comprehensively inform patients of potential side effects. Others emphasized that providers should not rush PrEP counseling. Because I feel like if you are doing it that fast you might run into the risk of drug interactions that you wouldn’t necessarily foresee if somebody forgets to – or doesn’t mention – a medicine that they take because they don’t think it's that serious. —Speaker 1, FGD 1
Core Components and Participant-Proposed Modifications
Participants were asked and provided feedback about each core component, as adapted by the Denver team and staff from the PrEP clinic SHC (Table 3). No substantive feedback was received for the front desk check-in or meeting with the medical assistant components of the proposed workflow.
Client-Proposed Modifications to Rapid PrEP Implementation Model.
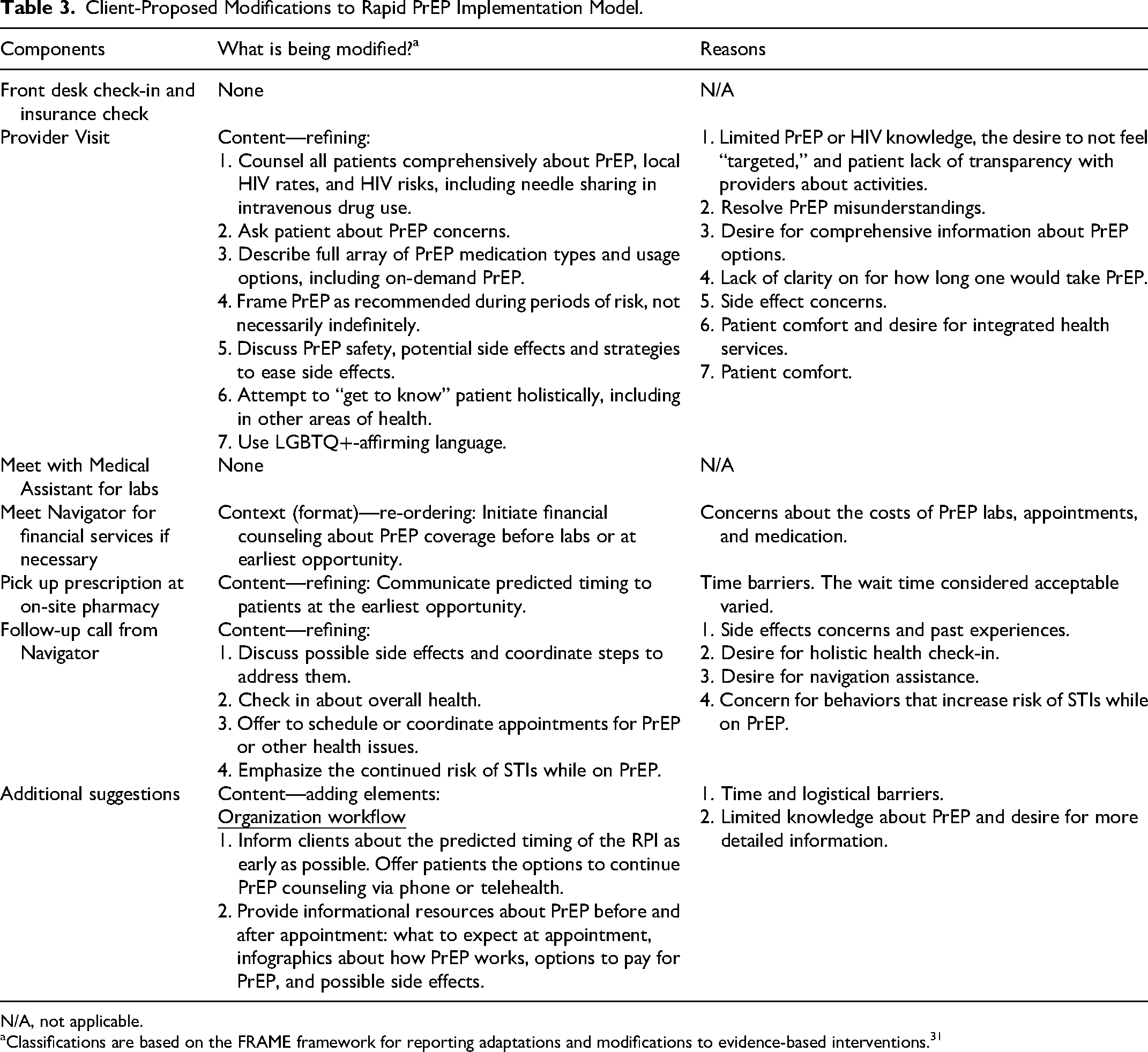
N/A, not applicable.
Classifications are based on the FRAME framework for reporting adaptations and modifications to evidence-based interventions. 31
Provider Visit
The Denver team described the steps of the provider visit as first assessing client interest in PrEP, then for those expressing interest, offering more information about the medication and, if appropriate, prescribing PrEP the same day. For those who report no interest but are eligible, the provider asks why and tries to understand the client's lack of interest. This approach was generally supported by participants, who offered additional feedback about initial PrEP counseling. Participants desired that all clients be counseled comprehensively about PrEP and HIV, regardless of perceived risk factors. Participants emphasized that patients do not always open up to their provider about activities that could put them at risk, underscoring the need for universal PrEP counseling. Additionally, they expressed that talking to everyone about PrEP might minimize the feeling of being targeted by a provider. I feel like it's damaging. I think that not everyone is asked if they want to be on it. It is damaging whenever you go to a doctor's office, and the doctor might look at you and be like, “Oh, maybe this person needs that.” They’re pegging you in some type of category, and it feels a little like if everyone were asked then it wouldn’t feel so heavy. —Speaker 2, FGD 5
In every FGD, participants identified discomfort with medical professionals as a barrier to PrEP care. Participants described distrust relating to systematic racism, gender- and LGBTQ+ -based discrimination in healthcare, unrelatable providers, perceived stigma, and suspicion of provider incentives to prescribe PrEP. This isn’t a jab toward [local clinic] at all, it's a larger medical conversation issue. A lot of people who work in medicine are poorly trained, or not trained, to deal with the complications of systemic issues that also intersect with the medical industry. When prefacing medication in such a general way, to certain groups of people, there are major problems that can arise. And, it continues to uphold a major wall, or a major barrier inside of education, and access to health for certain groups of people. Specifically, like Black and Brown communities, in New Orleans and elsewhere. —Speaker 5, FGD 4
Across FGDs, participants emphasized the need for education about PrEP, local HIV rates, and HIV risk factors, including sharing injection drug equipment. More requests for PrEP education arose in FGDs composed primarily of cis-women, trans women, trans men, non-binary, or gender-fluid individuals. Just keep pushing education, because it seems like we all could use some more in terms of everything that's coming up. I didn’t even know there was an alternative to Truvada, so it's good to know. Everybody should know that. —Speaker 6, FGD 5
Similarly, participants desired for providers to describe the full array of PrEP medication types and usage options, including on-demand PrEP. All FGDs suggested that providers provide more in-depth counseling about potential PrEP side effects. Specifically, they recommended providers address the expected course of side effects, potential long-term effects, strategies to ease side effects, and PrEP interactions with other drugs. However, some voiced that spending too much time on side effects might cause worry and deter them from PrEP. I think like talking about side effects, like psychologically just letting me know, like, what all has been seen, and like the statistics about the numbers about it. But for me, I wouldn't want you to linger on it too long, because then I'm gonna start worrying if you start talking about it for too long. —Speaker 3, FGD 2
Participants also desired LGBTQ+-affirming language. They noted that clients might feel more comfortable in settings with LGBTQ+-affirming signals, such as visibility of LGBTQ+ staff, LGBTQ+ signage in the clinic, and providers’ usage of LGBTQ+-affirming language. I feel like, for me, it's easier to open up about specific details of my sexual experiences so that they can work on like what's appropriate for me and whatnot. Just the way it's presented, and they're very open about LGBTQ terminologies, ideas, concepts, stuff like that. —Speaker 4, FGD 2
Navigator Services
A meeting with the clinic navigator to assist with PrEP access and financial considerations was discussed as a core component of the same-day process, and participants agreed with the importance of this encounter. Participants in 2 FGDs also stressed the need to initiate financial counseling about PrEP-related costs before labs were collected to avoid surprise costs. They also desired explanations of options to offset costs (eg, assistance to enroll in insurance, co-payment programs, or medication assistance programs).
Visit Timing
Because the RPI model might necessitate a longer clinic visit than SHC clients might expect due to PrEP counseling and labs, participants were asked how much additional visit time would be acceptable. Participants deemed a range of additional visit time acceptable, from 15 min to over an hour. Some expressed a preference for a longer visit rather than potentially compromising the depth of care. Similarly, participants voiced that they would be willing to wait to pick up their prescription at the pharmacy on-site. Across FGDs, participants requested that staff inform clients about the predicted visit timing at the earliest opportunity. In one FGD, participants suggested offering clients options to continue PrEP counseling via phone or telehealth.
Follow-up Phone Call From Navigator
All FGDs supported the core component of the RPI model in which a PrEP-specific navigator calls clients to assess for side effects, address concerns, remind clients of the follow-up PrEP appointment, and coordinate appointment scheduling as needed. They also thought the navigators should check in about the clients’ overall health and emphasize the continued risk of STIs while on PrEP. You need to tell these gays [said in jest] that just because you’re on PrEP that does not mean you cannot get gonorrhea and chlamydia and all this other stuff. Because these people are on PrEP and feel like they are invincible. When I tell you, they’re like, “I’m practically wearing a condom.” No, ma’am, you are not. Like, seriously. That needs to be emphasized. —Speaker 1, FGD 1
Discussion
Principal Findings
Clients from the New Orleans SHC found the plan to implement the adapted RPI from Denver to be a highly acceptable, feasible, and useful way to initiate PrEP. Eliminating the need to attend a separate appointment for PrEP counseling and initiation was unanimously appealing across FGDs. Clients noted that same-day PrEP initiation could minimize barriers to attending a separate PrEP appointment such as “flakiness,” logistical barriers, and inadequate knowledge about PrEP, including costs, side effects, and eligibility. Clients emphasized that the same-day model could resolve misunderstandings about PrEP and that both same-day financial counseling and follow-up navigation services would be helpful. They voiced support for a navigator to assess for side effects to PrEP alongside general health concerns, provide linkage to other types of care, and provide appointment reminders. Most FGDs with clients included a discussion of the desire for less siloed health services, in which navigators and providers offer support and coordinate care across multiple domains of health. Participants indicated that wraparound, integrated health services would better serve and retain PrEP-eligible clients across their clinical needs.
Participants also discussed systemic barriers to PrEP, such as community-level gaps in PrEP and HIV awareness, stigma, difficulty navigating insurance and co-pay programs, inequitable access to medical care, distrust of clinicians due to racism or identity factors, and inconsistency in whether providers initiate a PrEP conversation or make clients feel comfortable. The desire for more extensive PrEP and HIV education was voiced across FGDs, particularly in training providers to discuss PrEP, HIV risk factors, and local HIV rates with all patients in a destigmatizing and non-targeted manner. Many FGDs emphasized the need for community-level strategies to increase PrEP awareness.
Comparison to Prior Literature
The acceptability of the RPI in this sample is consistent with that of existing RPI programs.19,24 Participants’ feedback that providers discuss PrEP with all patients aligns with CDC guidelines which recommend that providers inform all sexually active patients about PrEP. 18 Prior research from New Orleans has found that a minority of providers discuss PrEP with eligible clients, 36 highlighting the need to train providers to have these discussions. Participants’ feedback to discuss PrEP with every client further aligns with reportedly low rates of PrEP awareness among PrEP-eligible groups.10-13 In these FGDs, there was limited knowledge of whether PrEP was appropriate for people who inject drugs and cisgender heterosexual women, despite low PrEP-to-need ratios for these groups.6,9,37 Client feedback varied between FGDs with distinct demographic characteristics, suggesting that purposeful collection of adaptation feedback from different populations may be useful in adapting RPI in other settings and in addressing demographic disparities in PrEP usage. 2
Participants’ support for receiving a call from a PrEP navigator after their SHC appointment is consistent with prior work indicating that active navigation and case management can improve retention in PrEP care and can help clients overcome common barriers. 38 Others have shown that active navigation of patients referred for PrEP is associated with an increased proportion of individuals that receive a prescription.27,39 Significant rates of patients lost to follow-up in other settings with RPI protocols similarly highlight the importance of providing navigation services.19-21,24,25 Similarly, participants’ emphasis on the importance of financial counseling is consistent with CDC guidance that clinics that implement same-day PrEP initiation protocols must be able to assist patient in enrolling in insurance or medication assistance programs. 18 Other sites that have implemented RPI programs similarly reiterate the importance of financial navigation.15,17,19,21,23,25
Limitations
A limitation of this study is that focus groups were only conducted on Zoom which meant participants were required to have internet access, time, and a quiet place to attend a FGD, and the ability to navigate Zoom. These structural and logistical requirements may have limited the range of participant perspectives represented, as clients facing these constraints may have had key feedback given that structural and logistical barriers to PrEP initiation were emphasized in these focus groups. As all participants chose to keep video off, the lack of visual cues may have also limited discussion engagement. Given the purposeful variation in demographic characteristics between FGDs, outcomes are not representative of issues unique to these demographic groups but provide insights that can be explored in future work.
Conclusion
FGDs with SHC clients eligible for PrEP show that the RPI model is highly acceptable and outlined key avenues to adapt the model to local client needs. Next steps include integration of client feedback into the RPI implementation plan, pilot testing and further adaptation as needed, and evaluating small-scale implementation for feasibility, impact, and sustainability. Numerous barriers to PrEP care, including gaps in knowledge about PrEP and logistical barriers, could be resolved or reduced via RPI implementation. In New Orleans, where high HIV incidence rates are sustained but a minority of PrEP-eligible clients receive PrEP,27,29,36 same-day PrEP initiation could be pivotal in changing local trajectory rates. Moreover, widespread implementation of RPI models and incorporating default PrEP counseling into SHC workflows can better meet the needs of clients lost to follow-up in traditional PrEP referral systems. Amidst nationally sustained HIV incidence rates, 40 population- and person-centered adaptations of PrEP services are imperatives for ending the HIV epidemic. 28
Supplemental Material
sj-docx-2-jia-10.1177_23259582241258559 - Supplemental material for Client Perspectives on the Development of a Rapid PrEP Initiative at a Sexual Health Center in New Orleans, Louisiana
Supplemental material, sj-docx-2-jia-10.1177_23259582241258559 for Client Perspectives on the Development of a Rapid PrEP Initiative at a Sexual Health Center in New Orleans, Louisiana by Aish Lovett, Rose Luder, Rebecca A. Lillis, Isolde Butler, Julia Siren, Samuel Gomez, Kevin Kamis, Oluyomi Obafemi, Sarah E. Rowan, Stefan Baral and Meredith E. Clement in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-3-jia-10.1177_23259582241258559 - Supplemental material for Client Perspectives on the Development of a Rapid PrEP Initiative at a Sexual Health Center in New Orleans, Louisiana
Supplemental material, sj-docx-3-jia-10.1177_23259582241258559 for Client Perspectives on the Development of a Rapid PrEP Initiative at a Sexual Health Center in New Orleans, Louisiana by Aish Lovett, Rose Luder, Rebecca A. Lillis, Isolde Butler, Julia Siren, Samuel Gomez, Kevin Kamis, Oluyomi Obafemi, Sarah E. Rowan, Stefan Baral and Meredith E. Clement in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-4-jia-10.1177_23259582241258559 - Supplemental material for Client Perspectives on the Development of a Rapid PrEP Initiative at a Sexual Health Center in New Orleans, Louisiana
Supplemental material, sj-docx-4-jia-10.1177_23259582241258559 for Client Perspectives on the Development of a Rapid PrEP Initiative at a Sexual Health Center in New Orleans, Louisiana by Aish Lovett, Rose Luder, Rebecca A. Lillis, Isolde Butler, Julia Siren, Samuel Gomez, Kevin Kamis, Oluyomi Obafemi, Sarah E. Rowan, Stefan Baral and Meredith E. Clement in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We thank LSU-CrescentCare and CrescentCare providers and staff for their collaboration, including Katey Varnado, Laura Hernandez, Eric Babineaux, and Christopher Garnett. We thank Brian Perry for guidance on qualitative analysis methodology.
Author Contributions
AL: investigation, analysis, and writing—original draft, review, and editing. RL: analysis and writing—original draft, review, and editing. RAL: conceptualization and review. IB: conceptualization and review. JS: conceptualization and review. SG: conceptualization and review. KK: conceptualization and review. OO: conceptualization and review. SR: conceptualization and review. SB: conceptualization, methodology, supervision, and writing—editing and review. MEC: conceptualization, funding acquisition, methodology, investigation, supervision, and writing—original draft, review, and editing.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MEC has received research support (grants to institution) from Gilead Sciences and ViiV Healthcare; has received consultancy/advisory board fees from ViiV Healthcare and FHI360; and has received personal fees for educational events from Vindico Medical, Education, Practice Point Communications, and Prime Education. RAL has conducted clinical trials at her institution for Abbott, Becton Dickenson, BioFire, Cepheid, Chembio, Cue, Gilead, Hologic, LabCorp, Merck, QuidelOrtho, Roche, and Visby; has served on a scientific advisory board for Abbott and Roche; and has received personal fees for educational events from Cepheid and Oakstone Publishing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the International Association of the Providers of AIDS Care and the Duke University Center for AIDS Research (CFAR), an NIH-funded program (5P30 AI064518).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.