
Abstract
Background
Providers caring for adolescents and young adults with HIV (AYA-HIV) mostly base their adherence counseling during clinical encounters on clinical judgment and expectations of patients’ medication adherence. There is currently no data on provider predictions of viral suppression for AYA-HIV. We aimed to assess the accuracy of provider predictions of patients’ viral suppression status compared to viral load results.
Methods
Providers caring for AYA-HIV were asked to predict the likelihood of viral suppression of patients before a clinical encounter and give reasons for their predictions. Provider predictions were compared to actual viral load measurements of patients. Patient data were abstracted from electronic health records. The final analysis included 9 providers, 28 patients, and 34 observations of paired provider predictions and viral load results.
Results
Provider prediction accuracy of viral suppression was low (59%, Cohen's Kappa = 0.16). Provider predictions of lack of viral suppression were based on nonadherence to medications, new patient status, or structural vulnerabilities (e.g., unstable housing). Anticipated viral suppression was based on medication adherence, history of viral suppression, and the presence of family or other social forms of support.
Conclusions
Providers have difficulty accurately predicting viral suppression among AYA-HIV and may base their counseling on incorrect assumptions. Rapid point-of-care viral load testing may provide opportunities to improve counseling provided during the clinical encounter.
Plain Language Summary
Providers caring for adolescents and young adults with HIV (AYA-HIV) mostly base their adherence counseling during clinical encounters on clinical judgment and expectations of patients' medication adherence. Currently, no data exist on provider predictions of viral suppression for AYA-HIV. We aimed to assess the accuracy of provider predictions of patients' viral suppression compared to viral load results. Providers caring for AYA-HIV were asked to predict the likelihood of viral suppression of patients before a clinical encounter with reasons for their predictions. Provider predictions were compared to actual viral load measurements of patients. Patient data were abstracted from electronic health records. The final analysis included nine providers, 28 patients, and 34 observations of paired provider predictions and viral load results. Provider prediction accuracy of viral suppression was low (59%, Cohen's Kappa=0.16). Provider predictions of lack of viral suppression were based on non-adherence to medications, new patient status, or structural vulnerabilities (e.g., unstable housing). Anticipated viral suppression was based on medication adherence, history of viral suppression, and presence of family or other social forms of support. Providers have difficulty predicting viral suppression among AYA-HIV and may base counseling on incorrect assumptions. Rapid point-of-care viral load testing may provide opportunities to improve counseling.
Background
An estimated 1.1 million individuals live with HIV in the United States, and nearly 50,000 new infections occur annually. 1 A significant number of these infections (20%) occur among adolescents and young adults (AYA) aged 15 to 24 years, a priority population for reducing HIV transmission as they have the second-highest HIV incidence. 2 Many of the new infections among AYA go undiagnosed, but the challenges facing AYA with HIV (AYA-HIV) are not limited to diagnosis alone. 3 Despite efforts to optimize HIV care, AYA continue to experience gross disparities along the HIV care cascade.4,5 AYA-HIV are less likely to access care, be retained in care, and achieve virologic suppression than other age groups. 2 The immediate goal of HIV treatment is achieving virologic suppression and improving the overall quality of life. Sustained virologic suppression decreases the risk of HIV transmission, reduces morbidity and mortality, and improves overall treatment outcomes for people living with HIV (PWH).6–8 As a result, “Ending the HIV epidemic: a plan for America” has set a goal of attaining and sustaining virologic suppression for 95% of PWH by 2030. 9 However, current trends in antiretroviral treatment (ART) outcomes for AYA-HIV threaten the timely realization of this goal.
While there is no widely accepted gold standard for assessing adherence to ART, 10 some frequently used measures include pill counts, patient self-reports of missed pills, pharmacy refill data, and other methods. More recent developments include technology-based directly observed therapy (DOT); however, no studies to date have used technology-based DOT to assess ART adherence in HIV treatment. 11
Adherence continues to be challenging for AYA-HIV. In a study of 379 AYA with perinatally acquired HIV, 30% reported nonadherence to ART, and nonadherence was significantly associated with virologic nonsuppression. 12 Similar findings are reported for AYA with nonperinatally acquired HIV.13,14 Some successes in viral suppression outcomes for AYA-HIV have been achieved through interventions to improve adherence (e.g., mobile apps, technology-based interventions, pill counts, HIV care transition). However, they are often short-lived, research-based, and difficult to duplicate, highlighting the need for practical and clinically relevant/instituted intervention.14-17
Point-of-care viral load testing significantly improves viral suppression and retention in HIV care compared to routine testing. 18 However, it is not traditionally utilized in the management of HIV, and traditional out-of-clinic laboratory testing remains the most conventional testing method due to its low cost and wide availability. Moreover, existing point-of-care viral load tests are predominantly based on a threshold of 1000 copies/mL, 19 which limits precision. In the absence of ubiquitous and precise real-time or point-of-care viral load testing, providers depend on self-reported adherence and subjective clinical judgment to make immediate clinical management decisions and target adherence counseling during the patient encounter.
Research on provider predictions of patient medication adherence has mostly focused on adults and demonstrates that provider predictions are frequently inaccurate.20,21 There are currently no data on provider predictions of viral suppression for AYA-HIV and how such predictions correlate with actual patient viral load measurements. Data on how well providers can predict viral load will allow us to determine if point-of-care viral load testing is indeed a strategy that would be beneficial in AYA-HIV care settings. Our study aimed to assess the accuracy of provider predictions of patient viral suppression compared to viral load results.
Method
From July to September 2021, we conducted surveys of HIV care providers of AYA-HIV aged 15 to 24 years followed in 2 outpatient clinics within a tertiary healthcare facility in Baltimore, Maryland. Providers from the 2 clinics were recruited via email outreach. After completing oral consent by phone, email links to a survey were sent to providers. Each week, Qualtrics surveys were programmed with the patient roster, which populated patient names in the surveys. Before the clinical encounter, providers were asked to complete a Qualtrics survey containing a series of questions: Providers were asked whether they were scheduled to see a given patient in the upcoming week (“Are you scheduled to see patient [NAME] in the upcoming week?” Response options: yes/no). If they confirmed the former, they were also asked to predict whether the patient would be virally suppressed (“Do you anticipate patient [NAME] will be virally suppressed when you see them for their next care appointment?” Response options: yes/no), and to provide open text reasons for their predictions (“Why do you think patient [NAME] will be virally suppressed or not suppressed?” Response option: Open-ended text entry). All responses were recorded in the Qualtrics online survey. A standard component of each patient visit is viral load testing. Viral load testing was conducted in the hospital's clinically certified laboratory, using real-time polymerase chain reaction. The results were expressed as HIV RNA copies per milliliter of plasma. Viral suppression status based on this laboratory testing was obtained from electronic health records and defined as VL < 20 copies/ml.
The primary outcome measure was the relationship between provider prediction of suppression status and actual viral suppression status. These data were analyzed using descriptive statistics (cross-tabulation) and interrater agreement measures (Cohen's kappa). Provider responses of reasons for their predictions were analyzed using deductive qualitative coding of open-text responses.
Ethical Approval and Informed Consent
The study was approved by the institutional review board of the Johns Hopkins University School of Medicine (Protocol IRB00211923; PI Dr Agwu). Providers completed oral consent by phone. The only data from participating patients came from retrospective chart reviews and did not require informed consent and assent.
Results
Data were collected over 8 weeks from 9 care providers (3 physicians, 1 nurse practitioner, 2 nurses, 1 clinical social worker, 1 mental health counselor, and 1 case manager). A total of 40 AYA-HIV were evaluated by providers at 53 visits. Of these, 28 patients and 34 clinical observations or visits were included in the final analysis. Twelve patients with 19 visits were excluded from the analysis because no laboratory viral load measurements could be obtained from the electronic health record. Clinical observations represent a pairing of provider prediction and viral load measurements and include 1 to 3 datapoints for each participant and 1 to 13 submissions per provider. Of the 34 paired observations, 22 (65%) had viral load measurements for the same visit of provider prediction, while the remaining 12 (35%) had viral load measurements available at the next visit with a median of 53 days lag in the availability between same visit and next visit viral load measurements.
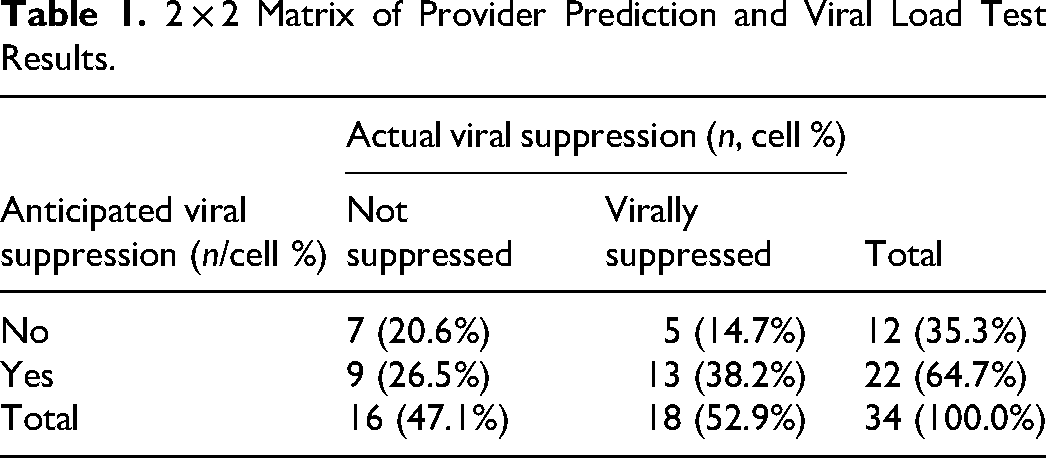
Provider prediction accuracy of viral suppression was low (59% accuracy, Cohen's Kappa = 0.16; see Table 1). Open text responses indicated that providers based an anticipated lack of viral suppression on nonadherence to medications, patients new to the clinic without a history/track record, or structural vulnerabilities (e.g., unstable housing). Anticipated viral suppression was based on medication adherence, history of viral suppression, and social/family support. However, none of these reported reasons differentiated well between patients who were virally suppressed in test results versus those who were not.
2 × 2 Matrix of Provider Prediction and Viral Load Test Results.
Discussion
To our knowledge, this is the first report that assesses the accuracy of provider predictions of AYA-HIV patients’ viral status. Our findings show that AYA-HIV providers have difficulty accurately predicting the viral suppression status of their patients. Prediction tools have historically been used to evaluate determinants of treatment adherence and HIV treatment outcomes, such as retention in care and virologic suppression among PWH.22-24 These prediction tools typically utilize mathematical models and the computation of patient characteristics. They give estimates of probabilities of viral suppression or nonsuppression over a period of time rather than specific time points, which our approach sought to assess.
Accurate assessment of patients’ virologic status at the time of the visit would allow for targeted, informed adherence counseling and timely delivery of needed interventions. This ideal is not feasible for most HIV care centers as viral load assessment in real-time and point-of-care viral load testing are not readily available. In the absence of real-time viral load testing, providers need to rely on their predictions of patients’ viral load status and adjust their counseling accordingly. However, based on our findings, such predictions may be prone to inaccuracies. The lack of precision in provider predictions observed in this study may be the result of incorrect assumptions about medication adherence, underscoring the need for point-of-care viral load testing for AYA-HIV.
Our study also found that predictions of virologic nonsuppression were largely based on factors such as nonadherence to ART, relatively new patient status (e.g., new diagnosis or new to the program without medical records), unstable housing, and a lack of family support. However, they failed to differentiate between patients who achieved viral suppression and those who did not. Similar patient characteristics have been used to predict virologic suppression in patients in clinical settings and research studies.20,23,24 However, as stated earlier, predictions were conducted using validated prediction tools proven to be more accurate due to their objectivity.
Our study has several limitations. First, the sample size was relatively small, making quantitative statistical analysis and comparison of characteristics between groups difficult. Given the small sample size, we also did not account for the clustering of individual participants within providers; larger studies are needed to replicate the results found in the current study. Also, we did not analyze the association between provider roles or age/race differences between providers and patients and their effect on the accuracy of predictions. Direct semiquantitative testing of antiretroviral medication adherence at the point of care has recently been shown to be feasible for some medications. 25 This may be an alternative to point-of-care viral load testing for some patients and was not explored in the current study.
However, the preliminary findings presented provide initial insights into providers’ perception of their AYA-HIV patients’ treatment adherence and their noncorrelation with their actual virologic status. Our findings also expose difficulties in providing tailored counseling to patients due to the lack of point-of-care testing and the insufficiency of subjective clinical assessments. The nascency of our findings calls for further studies to improve our understanding of providers’ predictions or estimation of patients’ adherence and how this impacts treatment outcomes for AYA-HIV. We hope that our findings also contribute to increasing interest in the development of point-of-care viral load testing, particularly for AYA-HIV, for whom virologic suppression and overall HIV outcomes remain relatively poor.
In conclusion, providers have difficulties accurately predicting the viral suppression of AYA-HIV and may base their counseling on incorrect assumptions. Rapid and sensitive point-of-care viral load testing may inform providers of poor treatment adherence and allow for the exploration of treatment barriers with their patients. As such, these tests may provide opportunities to optimize counseling and interventions provided during the clinical encounter.
Footnotes
Acknowledgments
We are grateful to the Johns Hopkins University Center for AIDS Research, an NIH-funded program, which facilitated this research with its infrastructure and resources. We are especially indebted to all the providers and IPC team that care for adolescents and young adults with HIV (AYA-HIV) that we have had the pleasure to work with during this research, and which contributed to our research.
Authors’ Notes
Johannes Thrul and Hasiya Yusuf contributed equally.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was facilitated by the infrastructure and resources provided by the Johns Hopkins University Center for AIDS Research, an NIH-funded program (P30 AI094189), which is supported by the following NIH cofunding and participating institutes and centers: NIAID, NCI, NICHD, NHLBI, NIDA, NIA, NIGMS, NIDDK, and NIMHD. The content is solely the authors’ responsibility and does not necessarily represent the official views of the NIH.