
Abstract
Although the identification of individuals infected with HIV is an important element of treatment and prevention programs, many people living with HIV are unaware of their status. Thus, individuals are unable to benefit from treatment, and preventable HIV transmission continues to occur. Rapid point-of-care testing for HIV has been found to be preferred by patients in some contexts. However, few studies have examined preferences in primary care populations. This study investigates HIV testing preferences within an urban primary care clinic. Employing a cross-sectional design, data were collected on demographic characteristics, HIV risk factors, and testing history and preferences of participants. A total of 81% of participants stated that they would prefer rapid testing to standard testing, a finding that is consistent across demographic variables and risk factors examined. Increased availability of this modality may decrease barriers to HIV testing, with positive implications both for clinical management of HIV infection and prevention of HIV transmission.
Introduction
Identification of individuals infected with HIV is crucial to effective prevention and treatment strategies. However, an estimated 25% of those who are HIV positive in the United States and 27% in both the United Kingdom and Canada are unaware of their infection status.1–3 Transmission from those who are not aware of their HIV-positive status contributes significantly to the burden of new HIV infections, 4 and late diagnosis has been shown to result in worse clinical outcomes.5–8 Increasing uptake of HIV testing has been identified as a priority by the World Health Organization. 9
One means to improve HIV testing uptake may lie in the increasing availability of rapid testing protocols, allowing for specimens to be collected and results delivered to patients and health professionals at the point of care, within the same visit. Many populations encounter barriers to HIV testing, including stigma and lack of access to health care services, and are consequently less likely to access testing. 1 Concerns regarding nominal reporting, anxiety related to waiting periods preceding receipt of results, and avoidance of multiple counseling sessions have been described as factors decreasing acceptance of standard testing protocols for HIV.10,11 These concerns may be reduced through increased availability of rapid testing.
Rapid testing has also been shown to increase the proportion of patients receiving results.10,12–14 This is a significant benefit, given the concern of undelivered results. 1 Failure to return for test results of HIV testing has been found to be related to factors including fear, apathy, time constraints, and motivation for testing. 15 By delivering results within 1 clinical encounter, rapid testing mitigates these barriers to complete counseling and testing.
Research on patient preferences suggests that rapid HIV testing may be acceptable and preferred over standard testing to many patients12–14 and that rapid testing can allow for high-quality counseling. 14 However, existing high-quality studies have largely focused on specific high-risk patient groups 12,14 —often those already accessing HIV testing at sites specialized for this purpose—rather than the general population, for whom voluntary testing is also recommended, but in many contexts not adequately delivered. 9 In many settings, rapid testing for HIV is available in specialized settings such as sexually transmitted infection (STI) clinics, but not in general primary care settings. The improvement of testing uptake, vital for both treatment and prevention programs (including strategies employing antiretroviral therapy [ART] for the prevention of transmission), 16 will require an improved understanding of testing preferences in a variety of populations, including those where prevalence of HIV infection is low to moderate.
Primary care represents an important venue for HIV testing: primary care clinics serve large communities with widely varying levels of risk of HIV acquisition, and existing research has found that some patients prefer HIV testing to be provided by their primary care physician. 11 However, little research has examined acceptability of rapid testing for HIV among primary care populations.
The objective of this pilot study is to examine attitudes toward HIV testing among female patients in an urban primary care setting and to compare preferences for rapid and standard testing. The results of this study may be used to guide health care providers in optimizing the provision of HIV testing, and more broadly, to improve HIV testing uptake and knowledge of HIV status in populations.
Methods
A self-administered written questionnaire was offered to patients attending an urban primary care (family practice) centre providing health services to a multicultural population. Inclusion criteria were female sex and aged 16 to 39 years. Consecutive women meeting inclusion criteria were invited to participate. Sample size calculation was based on the primary study objective of estimating the proportion of the sample population preferring rapid HIV testing (with a marginal error of ±7.5%), using a projection of 90% based on previous research in a similar jurisdiction. 14 Thus, 64 participants were required to complete the questionnaire. A target number of questionnaires distributed was set to 96, allowing for the possibility of as many as one third of participants accepting the survey but not providing a response on HIV testing preferences. All participants provided written consent for the study.
The questionnaire collected information on participants’ demographic information, risk factors for STIs and HIV, as well as HIV testing history, knowledge, and preferences. The questionnaire was field tested for clarity and acceptability and took approximately 10 minutes to complete.
Analyses of the data were carried out using Stata IC Release 11 (StataCorp LP, College Station, Texas). Fisher exact test (2-tailed) was used to examine associations between demographic and behavioral characteristics and HIV testing preferences, with P < .05 considered significant. Ethical approval for the study was granted by the (“Institution name withheld per submission guidelines”) Research Ethics Board.
Results
Participation and Inclusion
A total of 104 patients completed and returned the study questionnaire, with no patients declining participation. Of all, 100 participants reported a lifetime history of sexual intercourse and were included in further analyses.
Sexual History and Practices
The median reported number of lifetime sexual partners was 6 (interquartile range, 3-11 and range, 1-80), and the median reported number of sexual partners in the past year was 1 (interquartile range, 1-2 and range, 0-5). Among the participants, 73.0% reported intercourse within the past month and 91.0% reported intercourse within the past year; 84.0% reported lifetime experience of sexual intercourse with men only, 13.0% reported sexual intercourse with men and women, and 3.0% reported sexual intercourse with women only; and 26.0% reported a history of a STI.
Testing for HIV
Among the participants, 56.0% reported experience of HIV testing during their lifetime, 84.0% of participants stated that they were willing to be tested for HIV in the future, and 89.0% stated that, if HIV positive, they would take measures to decrease risk of transmission to partners.
Of those previously tested for HIV, 7.6% reported not being aware of the results, and 15.1% of those tested reported engaging in unprotected sexual intercourse between specimen collection and receiving results.
Awareness and Preferences Regarding HIV Testing
Of the participants, 15.0% were aware of rapid HIV testing and 2.0% had experience of a rapid test. Given a brief, neutral written description of rapid and standard testing protocols in the questionnaire, 81.1% of respondents stated that they would prefer rapid testing over standard testing. Of the respondents, 53.5% stated that they would be more likely to be tested for HIV, if rapid testing was readily available to them.
Table 1 describes participant HIV testing preferences by demographic characteristics and risk factors for STIs. Preferences for rapid testing were consistent across demographic characteristics (age, education, income, ethnicity, and foreign country of birth) and risk factors examined (history of STI, lifetime sexual partners >5, and partners in past year >1). A trend was noted toward a greater preference for rapid testing among participants who were married or in common-law relationships (90.2% preferring rapid testing) compared with those who were single (73.6%), although the significance of this trend (P = .06) did not reach the criterion set a priori.
HIV Testing Preferences by Participant Characteristics
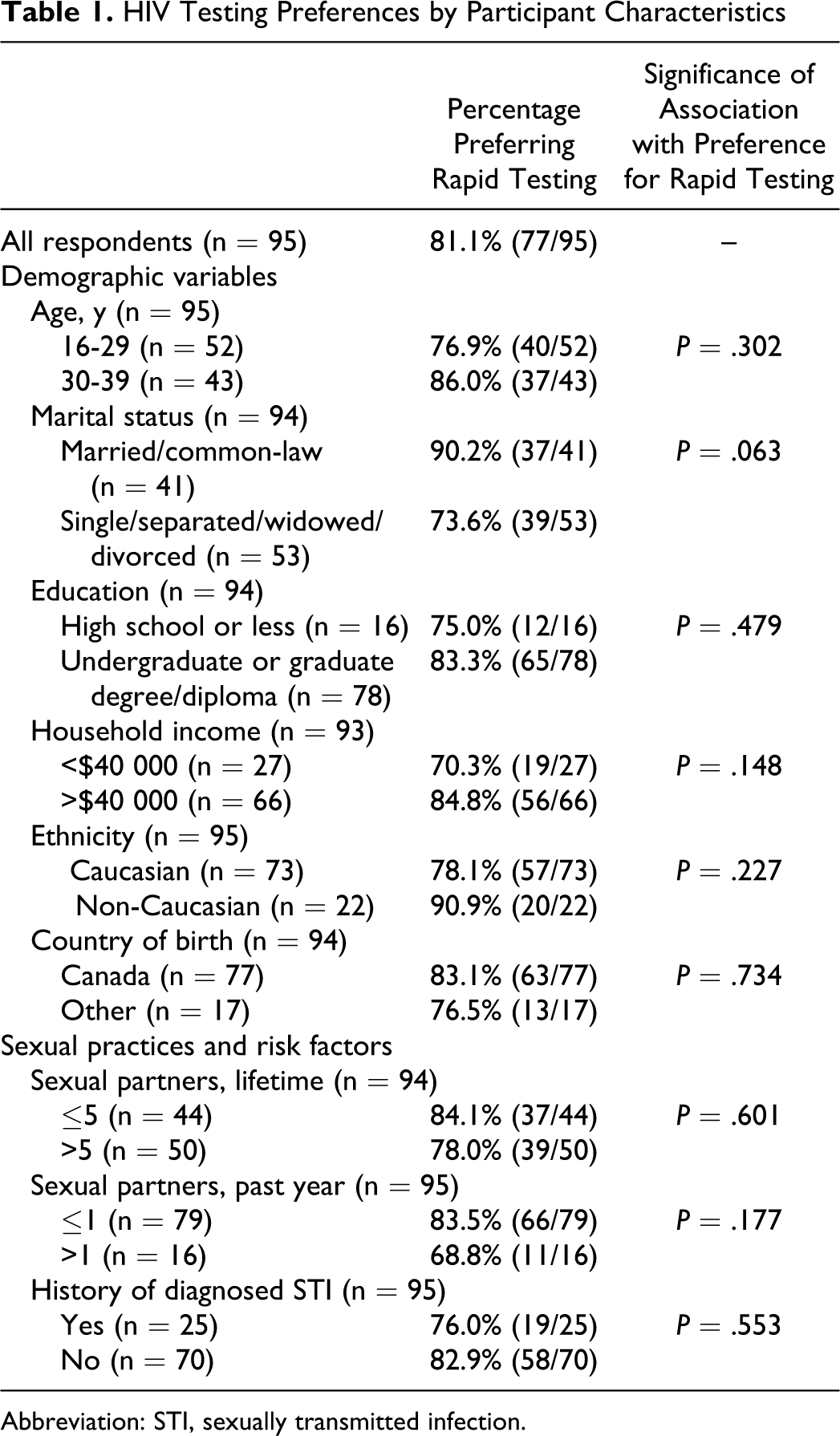
Abbreviation: STI, sexually transmitted infection.
Discussion
This study identified a strong preference for rapid testing for HIV among a female primary care population. This finding is consistent with prior research on rapid HIV testing in high-risk and low-risk populations. 11,12,14 Existing qualitative research has suggested that shorter waiting times may be a factor in such preferences, and that for some patients, testing in a primary care setting may avoid stigma perceived in specialized centers. 11
Identification of individuals living with HIV infection is required for the realization of numerous clinical and public health benefits. Antiretroviral therapy has been widely demonstrated to reduce HIV-related morbidity and mortality. 17 Also, a potential role of ART in prevention of HIV transmission has been supported by observational studies of serodiscordant couples, 18 –20 as well as population data indicating that increased ART use in communities may lead to decreased HIV prevalence. 21,22 Furthermore, research has shown that diagnosis of HIV infection in an individual may lead to a reduction in unprotected intercourse. 18,23,24
This pilot study was limited by a sample size that was insufficient for the stratification of demographic characteristics and risk factors to a degree finer than that described here. Statistical power was sufficient to address the primary objective of this study, to examine the overall HIV testing preferences of the population sampled, but not sufficient to rule out subgroup differences. Prior research has found that HIV testing preferences may vary by age, gender, ethnicity, sexual orientation, education, income, employment, and other variables. 13,25 –27 Notably, a recent large study found that patients at higher risk of HIV were more likely to choose rapid over standard HIV testing protocols. 27 In order to optimize the provision of HIV testing methodologies, continued research designed to examine preferences among the large variety of communities affected by HIV is imperative.
Conclusions
Rapid point-of-care testing for HIV was preferred to standard testing in this female primary care population. Implementation of rapid HIV testing in primary care settings has the potential to increase uptake of HIV testing and delivery of results in primary care populations. This may lead to improved treatment and preventive activities, among individuals and in populations. HIV treatment and prevention strategies will benefit from the application of this developing knowledge base.
Footnotes
Appendix A
Appendix B
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.