
Abstract
Recent studies have shown social determinants of health (SDOH) to impact HIV care engagement. This cross-sectional study (Oct 20-Apr 21) assessed the impact of a range of SDOH on HIV care engagement using data from HIV Care Connect, a consortium of three HIV care facility-led programs (Alabama, Florida, Mississippi). The exposures were captured using the PRAPARE (Protocol for Responding to and Assessing Patient Assets, Risks, and Experiences) scale. The outcome was captured using the Index of Engagement in HIV Care scale. Participants (n = 132) were predominantly non-White (87%) and male (52%) with a median age of 41 years. Multivariable logistic regression adjusted for various sociodemographics showed lower HIV care engagement to be associated with being uninsured/publicly insured, having 1-3 unmet needs, socially integrating ≤five times/week, and having stable housing. Factors such as unmet needs, un-/underinsurance, and social integration may be addressed by healthcare and community organizations.
Plain Language Summary
Assessing How Social Drivers of Health Affect Engagement in HIV Care in the Southern United States
It has been found that social factors that have a direct impact on health affect engagement in HIV Care among people living with HIV. We included various social drivers of health to see how they affect engagement in HIV Care. We used data between October 2020 and April 2021 from a project titled HIV Care Connect, which is a group of three facilities providing HIV care in Alabama, Florida, and Mississippi. We used social drivers of health as risk factors from a scale called PRAPARE (Protocol for Responding to and Assessing Patient Assets, Risks, and Experiences). Engagement in HIV care was measured by using a scale called Index of Engagement in HIV Care. A total of 132 participants were included. Majority of the participants were of races other than white (87%), male (52%) and were aged 41 years on average. Statistical analysis showed that participants without insurance or with public insurance, participants with 1-3 unsatisfied needs, participants that met with other people less than or equal to five times a week, and participants that had reliable housing had lower engagement in HIV care. These factors have a potential to be addressed by healthcare and community organizations.
Introduction
The White House National Office of National AIDS Policy (ONAP) first published the National HIV/AIDS Strategy (The Strategy) in 2010 in an effort to reduce the number of HIV infections across the United States (U.S.). The Strategy has recently been updated for 2022 through 2025 to guide efforts to achieve the ambitious end the HIV epidemic goals by 2030. 1 Similar to previous iterations, the most recent document outlines four goals needed to reduce new HIV infections by 75% by 2025 and by 90% by 2030: (1) prevent new HIV infections; (2) improve HIV-related health outcomes of people with HIV (PWH); (3) reduce HIV-related disparities and health inequities; and (4) achieve integrated, coordinated efforts that address the HIV epidemic among all partners and stakeholders. 1 The plan outlines 21 objectives that fall under these four goals, which include addressing the structural and social determinants of health (SDOH) that contribute to disparities in HIV treatment and outcomes, as well as increasing access to and retention in HIV care. 1
Complementary to the National HIV/AIDS Strategy, the Department of Health and Human Services’ (HHS) (EHE) calls for a “whole-of-society effort” that requires commitment from not only HHS agencies, but also state and local jurisdictions, tribal governments, health departments, HIV healthcare providers, opioid-use disorder treatment providers, research institutions, and community-based organizations. 2 Much like the goals outlined in The Strategy, the EHE initiative aims to: (1) diagnose all PWH as quickly as possible; (2) treat PWH rapidly and effectively to reach viral suppression; (3) prevent new HIV transmissions by using proven interventions; and (4) respond quickly to potential HIV outbreaks to get prevention and treatment services to people in need.
In addition to outlining goals and objectives, The EHE Plan and The Strategy identify populations that experience higher incidence and prevalence of HIV In 2020, the HIV incidence rate among African Americans/blacks was nearly eight times that of Whites (37.4 vs 4.60 per 100 000) and more than twice that of Hispanics/Latinos (16.7 per 100 000). 3 Additionally, nearly 68% of new infections in 2020 were attributable to male-to-male sexual contact as compared to 7% from heterosexual contact. 3 Moreover, severe geographical disparities among HIV rates and treatment outcomes also exist in the U.S. In 2020, over half of all new HIV diagnoses were in the South. 3 In addition to having a higher HIV incidence rate, the Southern U.S. also had the highest number of PWH as of 2020. 4
A centerpiece of The Strategy is the public health model, HIV Care Continuum. 1 The HIV Care Continuum outlines the goals that are fundamental in achieving viral suppression in a newly diagnosed person, including timely linkage to HIV care, receiving and being retained in HIV care, and ultimately achieving and maintaining viral suppression. 5 Although achieving viral suppression may seem straightforward when looking at the HIV Care Continuum, many individuals are unable to achieve these desired outcomes as they are disproportionally impacted by various SDOH. SDOH are defined by CDC as “The non-medical factors that influence health outcomes. They are the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life.” 6 Previous studies have shown SDOH to impact the desired HIV goals among PWH. A cross-sectional study using the CDC medical monitoring project data (2015-2019) assessed the impact of a variety of SDOH (education, economic stability, health, neighborhood, and built environment) and HIV care outcomes (missed appointments, adherence to ART, and durable viral suppression) and found that as the number of SDOH increased, the likelihood of missing appointment increased and the likelihood of reported ART adherence and viral suppression decreased. 7 When focusing in the South, SDOH such as poverty, education, access to healthcare, racism, homophobia, transphobia, and HIV stigma are more severe than other parts of the U.S., which may have a more profound impact on HIV-related outcomes. 8 A study conducted in Miami assessing the relationship between SDOH (economic stability, education, social and community context, health and healthcare, and neighborhood and built environment) and uncontrolled HIV (not achieving viral suppression) among PWH found economic stability, education, and health and healthcare to be associated with uncontrolled HIV. 9 Although a lot of research has been conducted assessing the impact of SDOH on HIV care outcomes, most studies have been conducted in non-Southern areas of the U.S. Additionally, those that have been conducted in the South are heavily focused on the African American population.10,11 Therefore, we sought to examine the impact of a range of SDOH (personal characteristics, family and home, money and resources, and social and emotional health) on HIV care engagement among PWH in three Southern U.S. states (Alabama, Florida, and Mississippi).
Methods
HIV Care Connect Program
In efforts to reduce the ongoing HIV-related disparities faced by PWH in the Southern U.S., the Merck Foundation funded the HIV Care Connect (HCC) program, which is aimed at reducing disparities in access to care and improving health outcomes for people of color living with HIV in the Southeastern United States. 12 HCC is a 5-year initiative and is being implemented by three healthcare organizations across the South: Care Resource in Miami, Florida; Five Horizons Health Services-Montgomery (FHHS-M), formerly called Medical Advocacy and Outreach, in Montgomery, Alabama; and the University of Mississippi Medical Center (UMMC) in Jackson, Mississippi.
The overall HCC program goals are to (1) improve linkage to and retention in high-quality HIV care for populations most affected by HIV; (2) build sustainable collaborations between the healthcare sector and other sectors to address access barriers related to the SDOH; (3) improve health outcomes for PWH, particularly in underserved communities; and (4) disseminate key findings and program results to advance best practices for improving HIV care. Although each HCC site is implementing a unique program, they share the same goal of overcoming disparities in HIV treatment and adherence by directly addressing patients’ SDOH via intensive case management models. 13 Through intensive case management, social workers, case managers, and linkage coordinators use a variety of patient reported outcomes (PROs) screeners and motivational interviewing techniques to help identify any potential barriers to care, as well as specific social needs that may hinder treatment adherence. Given that not all patients are eligible for such services, or are in need of this additional assistance, these staff members can have relatively small caseloads when compared to the average medical case manager. This enables them to dive deep into the needs of each patient and spend a substantial amount of time addressing each need (eg, accompanying patients to appointments at community partners instead of just scheduling appointments for patients or conducting motivational interviewing sessions with patient to engender behavioral change).
The Merck Foundation selected the University of Alabama at Birmingham (UAB) to serve as the National Program Office for HCC. The role of UAB in HCC includes conducting routine cross-site evaluations of these programs, as well as providing technical assistance and coordinating program activities across sites. Together with the HCC sites, the Research and Informatics Services Center (RISC) at UAB developed a data dictionary to be used across the organizations to capture clinical and PRO data. With a year of planning (2020) and a delayed start due to COVID-19, UAB started receiving data from the HCC sites in March 2022.
Using the HCC data, we included SDOH characteristics captured through the PRAPARE (Protocol for Responding to and Assessing Patient Assets, Risks, and Experiences) scale as our exposure variables. In 2013, the National Association of Community Health Centers, Inc. (NACHC), Association of Asian Pacific Community Health Organizations (AAPCHO), and Oregon Primary Care Association (OPCA) collaborated to develop PRAPARE. 14 The components added in the PRAPARE survey were influenced by the Healthy People 2020, ICD-10, and Meaningful Use Stage 3. 14 The PRAPARE components also align with CDC's definition of SDOH. 6 PRAPAPRE was piloted in 2014 and was first used in 2019 for addressing the needs of complex patients in a health center in Ohio. 14 Additionally, in 2019, PRAPARE became the most commonly used survey to screen for social needs by Medicaid. Moreover, in 2020, PRAPARE was used for the first time in a published peer reviewed article. 14 PRAPARE is a relatively new scale to measure SDOH and not many studies have utilized this tool as a correlate of healthcare outcomes. Of the few studies available, most have utilized a single cumulative PRAPARE score instead of assessing each characteristic separately. 15 Our decision to incorporate PRAPARE as a part of the HCC was based on the comprehensiveness of this scale and also the recent popularity of the PRAPARE scale as being the most commonly used standardized social risk screening tool in 2020 as per UDS data, which further corroborates to its usefulness. 14
The outcome, HIV care engagement, was captured using the Index of Engagement in HIV Care. The Index of Engagement in HIV Care has shown to be associated with HIV retention in care and viral suppression outcome. 16 We could not find a single study which assessed HIV-related outcomes using PRAPARE. Overcoming this gap in literature, our study is the first, to our knowledge, to use the characteristics captured with PRAPARE in assessing HIV care engagement via a validated, self-report instrument.
Study Design
A cross-sectional analysis was conducted using data from the three HCC-participating sites between October 2020 to April 2022. Participants were required to have complete data on all variables to be included in this study. Sites routinely reported data on patient demographics, labs (CD4 and viral load lab dates and results), and visit data (visit dates, visit status, and visit modality). In addition to these, the sites also provided self-reported responses gathered from patients completing information on different PROs.
Description of Variables
The outcome variable, HIV care engagement, was measured by the Index of Engagement in HIV Care (α = 0.88), 17 which contains 10 questions, each having five options to select from based on the severity; 1 being the least and 5 being the most. Some of the questions assessed in the questionnaire include, “How much do you trust your HIV care provider?”, “How open do you feel you can be with your HIV care provider?”, “How comfortable do you feel asking questions during your HIV care appointments?”, and “How well do you follow through on your HIV care when things in your life get tough?”; Supplementary figure 1 contains the 10 questions from the Index of Engagement in HIV Care with the response options for each. Once completed, the responses from the 10 questions are summed up to produce a cumulative score; a higher cumulative score indicates better engagement in HIV care. For this study, the outcome, engagement in HIV care, was divided into three categories, low engagement (score 0-40), moderate engagement (score 41-46), and high engagement (score ≥47); the cut-offs were chosen based on the tertiles. The categories are thought to correspond to the level of resources and efforts needed to improve/maintain HIV care engagement, with low requiring the most and high requiring least efforts/resources. Previous studies utilizing the Index of Engagement in HIV Care have included it as a continuous outcome. While modeling HIV care engagement as a continuous outcome has some appeal, categorizing HIV care engagement into low, middle, and high categories may have more pragmatic value for practitioners who need to prioritize individuals for additional effort and intervention. For example, clinics may choose to systematically focus their time, effort, and resources on individuals with low engagement.
The exposure variable capturing social determinants used the PRAPARE score. The PRAPARE scale (α = 0.86) 18 is divided into four major sub-groups: personal characteristics, family and income, money and resources, and social and emotional health. 19 Each option under every question in PRAPARE is designated a score of either 1 or 0; a score of 1 indicates a patient-related characteristic that has a potential to impact one's health disproportionality. Each question under PRAPARE was included as a unique variable in the study. Supplementary figure 2 outlines the questions assessed within PRAPARE along with the scores associated with each response.
A set of covariates/confounders at study baseline were also included in this study. Age was included as a continuous variable, whereas the rest of the variables were categorized as the following, gender: male, female, transgender (only included male to female), and “refused to answer”; depression measured by the Patient Health Questionnaire-9 (PHQ-9) scale (α = 0.89) 20 : no/mild depression (score 0-9) and moderate/severe depression (score ≥10) 20 ; ART adherence measured by the degree to which an individual was taking their HIV medication routinely in the past 4 weeks (α = 0.83): excellent (score of 6) and < excellent (score <6) 21 ; alcohol use measured by the Alcohol Use Disorders Identification Test (AUDIT-C) scale (α = 0.75) using sex at birth: yes (score ≥4 for male and score ≥3 for female) and no (score <4 for male and <3 for female) 22 ; and substance use measured by the Drug Abuse Screening Test (DAST) scale (α = 0.93) 23 : none (score 0), low/moderate (score 1-5), and substantial/severe (score 6-10). 23
The rest of the categorical variables were from PRAPARE and were self-reported. Among Personal Characteristics, the social construct race was first categorized as White, African American, and “other,” which included Asian, Pacific Islander, Native Hawaiian, American Indian/Alaskan Native, and “other.” However, due to a very small number of individuals in the “other” group (n = 7), the other category was combined with African Americans and was re-named as “non-Whites”; ethnicity was categorized as Hispanic/Latino and Non-Hispanic/Latino; farm worker status was categorized as yes and no; veteran status was categorized as yes and no; and English proficiency (language most comfortable with) was categorized as English and Language other than English. Under Family and Home, federal poverty level was categorized as ≤100%, 101-150%, 151-200%, and ≥200%; housing situation was categorized as housing available and no housing available; and housing stability was categorized as stable and unstable. Under Money and Resources, education was categorized as ≤ High School/GED and > High School/GED; employment was categorized as full-time and part-time/unemployed (seeking and not seeking work); insurance was categorized as public/uninsured (CHIP Medicaid, Medicaid, Medicare and other public insurance) and private; material security included food, clothing, utilities, child care; medicine/healthcare, phone, and other; each was designated a score of 1. Based on the cumulative score, material security around the time of visit was categorized as no unmet needs (score 0), 1-3 unmet needs, and 4-7 unmet needs; and transportation was categorized as no transportation needs, medical transportation needs, non-medical transportation needs, and medical and non-medical transportation needs. Lastly, within Social and Emotional Health, social integration was categorized as >5 times/week and ≤5 times/week and stress was categorized “not at all stressed” and “little to very stressed (little bit, somewhat, quite a bit, very much).”
Statistical Analysis
Descriptive statistics were calculated for the demographics as well as characteristics captured using PRAPARE by low, moderate, and high HIV care engagement. Frequencies and proportions were calculated for categorical variables and median and interquartile ranges were calculated for continuous variables. For bivariate analyses, we conducted Cochran-Mantel-Haenszel tests for categorical and Kruskal-Wallis test for the continuous variables. Due to the small sample size, statistical significance cut-off was set at a two-sided P ≤ .1. For the multivariable analysis, due to the ordinal nature of the care engagement outcome, proportional odds model was fit, which calculated the adjusted odds ratios (AORs) and their accompanying 95% confidence interval (CI) representing lower versus higher care engagement for each characteristic captured using PRAPARE. The adjusted model controlled for all the aforementioned sociodemographics and PROs; farm worker status (from PRAPARE) was excluded from the final model due to incomprehensible AORs (95% CI) associated with it. All analysis was carried out in SAS 9.4. 24
Sensitivity Analysis
Since a modest proportion of individuals were being excluded from the multivariable analyses due to missing data for at least one variable (n = 58, 31%), we endeavored to evaluate the pattern of missingness and found that the variables Ethnicity (n = 74) and Federal Poverty level (n = 43) had the highest number of participants with missing data. We examined whether these variables as well as our outcome variable, Care Engagement Index, followed a particular pattern of missingness across sites, ie, if these variables were uniformly missing from all sites. Ethnicity was missing at FHHS-M (missing = 24) and Care Resources (missing = 50), but not UMMC (missing = 0); Federal poverty level was missing at FHHS-M (missing = 21) and UMMC (N = 22) but not Care Resources (missing = 0); and Care Engagement Index was missing mostly at UMMC (missing = 17) but minimally at FHHS-M (missing = 3) and Care Resources (missing = 2). In addition to this, we also compared all variables descriptively and bivariately (Supplementary table 1) between individuals with complete data (n = 132) versus individuals removed due to missingness (n = 58). Apart from a few variables, we did not observe any significant differences among the two groups and made the decision to only include individuals with complete data for this manuscript. To verify our decision, we also carried out a sensitivity analysis in which a separate missing category was assigned for individuals with missing data for the ethnicity and/or federal poverty variables. This increased the sample size to 158 individuals (83%). The multivariable analysis showed very similar parameter estimates, CIs, and statistical significance to the model with complete cases (Supplementary table 2), suggesting the associations observed and inference drawn from the complete cases (n = 132) were robust to missing ethnicity and federal poverty data.
Ethical Approval and Informed Consent
The Institutional Review Board (IRB) at the University of Alabama at Birmingham acted as the central IRB, whose review was accepted by all participating institutions’ IRBs (IRB-300006212). The central IRB determined that this research involved no greater than minimal risk and approved a waiver for informed consent. Approval was granted on November 13, 2020.
Results
A total of 189 individuals were included. After excluding individuals with missing data, 132 unique individuals remained. Overall, based on the multi-item, self-reported HIV Care Index instrument, 40.2% reported low, 31.1% reported moderate, and 28.8% reported high-care engagement; since individuals with missing data were excluded after categorizing by HIV care engagement, the proportion among the three groups is not evenly distributed. The study population had a median age of 41 years and was comprised of predominantly African American (79.5%), non-Hispanic (53.0%), and male (52.3%) participants. The bivariate analysis (Table 1) showed that individuals reporting higher HIV engagement were more likely to be non-White, be female, report integrating socially >five times/week, and report excellent ART adherence. The multivariable analysis (Table 2) showed that individuals uninsured/publically insured versus privately insured [AOR (95% CI): 3.47 (1.06, 11.35)], individuals reporting 1-3 unmet needs versus those reporting no unmet needs [AOR (95% CI): 3.63 (1.13, 11.65)], individuals reporting social integration ≤five times/week versus >five times/week [AOR (95% CI): 3.49 (1.62, 7.55)] had higher odds of reporting lower HIV care engagement, whereas those reporting unstable versus stable housing [AOR (95% CI): 0.34 (0.15, 0.79)] had lower odds of reporting lower HIV care engagement.
Patient Characteristics for the Study Population by HIV Care Engagement (n = 132).
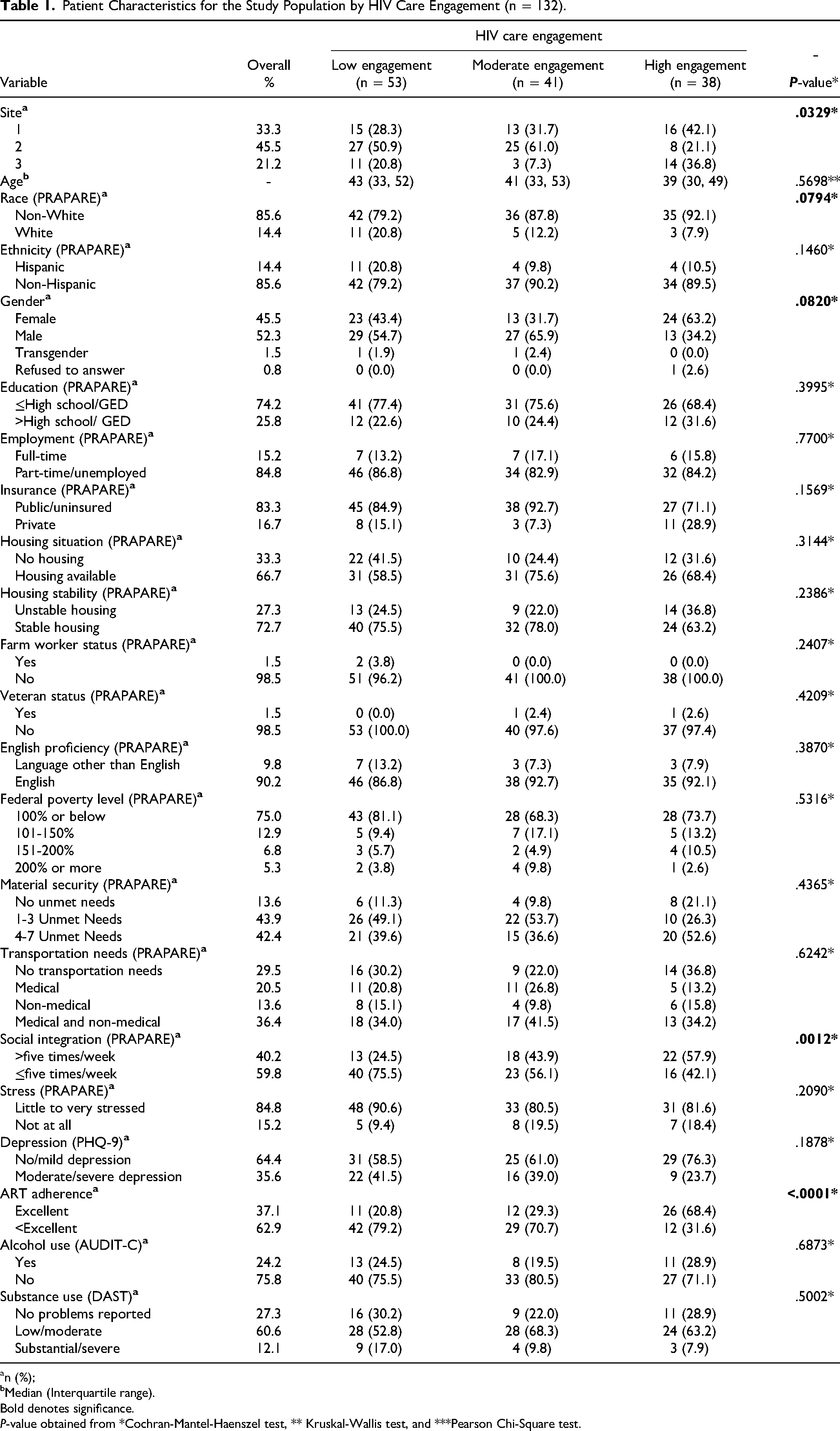
n (%);
Median (Interquartile range).
Bold denotes significance.
P-value obtained from *Cochran-Mantel-Haenszel test, ** Kruskal-Wallis test, and ***Pearson Chi-Square test.
Multivariable Proportional Odds Model Representing Odds of Lower Versus Higher HIV Care Engagement with PRAPARE.
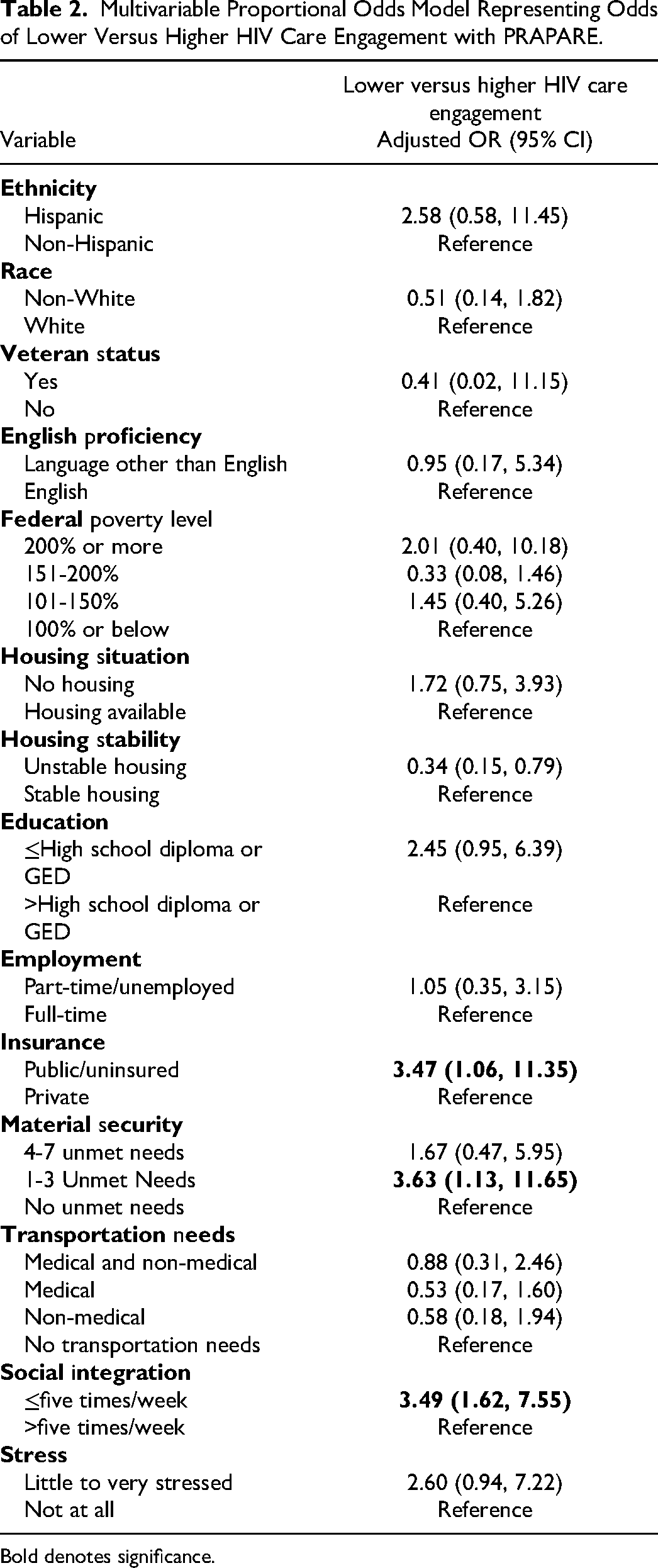
Bold denotes significance.
Discussion
The findings from this study indicate that several SDOH captured with PRAPARE were significantly associated with HIV care engagement as measured by a multi-item, validated index of care engagement. More specifically, those who were publically insured (eg, Medicaid), uninsured, reporting 1-3 unmet needs, and seeing or talking to people they care about ≤five times/week reported lower HIV care engagement than their counterparts. Overall, it appears that these findings align with the literature on SDOH and HIV Care engagement, although we were unable to identify any study that specifically examines HIV care engagement by PRAPARE variables. Most prior studies focused on a subset of SDOH factors lacking the breadth and structure afforded by using a comprehensive, standardized instrument like PRAPARE. Moreover, as PRAPARE was developed for use in clinical settings, use of this measure in three diverse clinic-based populations as part of HCC supports the deployment of this instrument more broadly in other care settings. Indeed, beyond the subset of program participants, one HCC site incorporated the PRAPARE instrument into their social work / case management protocols as standard of care for all patients.
One study, for instance, assessing HIV retention in care among ART-naïve PWH found publically insured PWH to be less likely to be retained in care than privately insured PWH. 25 Another survey-based study in Seattle, WA among PWH who completed at least one visit with the Care and Antiretroviral Promotion Program (CAPP), which is aimed to promote HIV care engagement and ART among PWH, found being uninsured to be a barrier to seeking HIV care. 26 Another qualitative study assessing barriers and facilitators to HIV retention in care among PWH in Philadelphia, PA found lack of insurance to be a commonly listed barrier to retention in care among PWH not retained in care. 27
This Philadelphia study also found social support to facilitate HIV retention in care, which was similar to what we observed in our study, where PWH reporting higher incidence of social integration (interacting with people they care about > five times a week) reported higher HIV care engagement than those reporting lower incidences of social integration. Although social integration and social support are distinct measures, they are likely related as social integration may provide some level of social support to the PWH. Similarly, a qualitative study conducted in Kentucky between December 2019 to June 2021 among young, black, cis-gender men who have sex with men found social support in the form of verbal encouragement from family, friends, partners, and mentors to facilitate HIV retention in care. 28 In addition to social support, the Kentucky study also found housing insecurity to act as a barrier to retention in care. 28 Similar findings were noted in the Seattle study, where homelessness was found as a barrier to HIV care. 26 Contrary to these findings, our study indicated those with unstable housing to have higher self-reported engagement than those with stable housing. This may be due to existing efforts being placed on improving retention in care among those with unstable housing at the HCC-participating sites. For example, one of the HCC sites provides intensive care management focused specifically on PWH who have limited access to care, including and especially people experiencing homelessness or those living in rural areas. Another HCC site has partnered with a local community organization to receive referrals of vulnerable individuals who need HIV prevention and treatment services and refer patients to the partner's transitional housing program.
Additionally, a mixed-methods study in Washington, DC found that PWH retained in care to have lower mean unmet needs than those not retained in care (1.6 vs 2.3). 29 Another qualitative study conducted among PWH not fully engaged in HIV care or at risk for falling out of care found that higher levels of unmet needs (eg, finances, transportation, and substance use) were associated with lower engagement in HIV care. 30 Similarly, another study assessing the relationship between unmet needs and HIV retention in care and viral suppression among out-of-care PWH hospitalized at a safety-net institution in Houston, Texas, found those with ≥3 unmet subsistence needs (housing, transportation, food, or financial needs) to be less likely to be retained in care post-discharge. 31 These findings were in line with our findings where those with no unmet needs reported higher HIV care engagement. Furthermore, a factor consistently found to act as barrier to HIV care engagement in the literature was lack of transportation.26,27,29,31 Although our study did not assess presence versus lack of transportation with HIV care engagement, we did assess transportation needs using PRAPARE and found no association between transportation needs and HIV care engagement.
By providing evidence on the specific SDOHs that act as a barrier to HIV care engagement in this population, this study demonstrates the importance of one of the four overall goals of the HCC program—addressing barriers related to SDOH. Taken together, our findings indicate that a number of SDOH had a significant impact on the HIV care engagement among PWH. Specifically, insurance, housing status, level of unmet needs, and level of social integration were associated with HIV care engagement. HCC sites, and other healthcare organizations, can utilize this information to address HIV care engagement among PWH. While CBOs may be better suited than medical clinics in addressing social integration depending on the level of services clinically available, other identified factors such as insurance and unmet needs may be more directly manageable by HIV clinics. Organizations can systematically assess the unmet needs in PWH seeking care, as well as their insurance status, and intervene early to address any barriers to care engagement. The PRAPARE represents a tool that can be integrated into clinical care and workflow to allow for consistent and standardized assessment of these and other SDOH domains.
Research has documented a growing awareness of SDOH in clinical settings and increasing efforts to screen for SDOH among patients32,33; however, far less research has examined concerted efforts to intervene and address SDOH in these settings, particularly primary care and community-based settings. 34 While our study begins to address this gap, more research is needed to understand what components of these different programs are most effective (when and for whom) for addressing SDOH in these settings and improving retention in care.
Strengths and Limitations
Our data were gathered from three states in the Southern U.S., and while our findings may not be generalizable to all PWH in the U.S., findings may be more generalized to other PWH in the South. Additionally, to our best knowledge, this is one of the first studies in the field of HIV and one of the few overall that has utilized the PRAPARE scale to assess SDOH. With strengths, this study also has a few limitations. The data for this study were collected amidst the global COVID-19 pandemic, which may have impacted participants’ responses, especially those pertaining to the SDOH and HIV care engagement. Additionally, most of the variables were self-reported, which is susceptible to response, recall, and social desirability bias. Although PRAPARE captures a large range of SDOH, it does not capture some of the other SDOH, such as, living environment, food access, and healthcare assess, which may also have an impact on the HIV care engagement. Moreover, due to the utilization of self-reported data, many individuals who did not have complete data on all the variables were excluded, leading to a small sample size with reduced representativeness. The modest sample size may have resulted in a lack of statistical significance despite clinically meaningful differences for some variables. Additionally, our decision to model HIV care engagement as a categorical variable may limit the generalizability of our findings to studies using different cut-points for categorizing the HIV care engagement. Lastly, although some South-based studies support our findings, most of the studies cited are conducted in non-Southern areas, which may lack generalizability.
Conclusion
Our study found insurance type, level of unmet needs, and level of social integration to be associated with lower HIV care engagement among PWH in care at three Southern U.S. clinics. Healthcare organizations may consider addressing unmet needs and un- and underinsurance to increase HIV engagement among their patient population. Additionally, partnerships with community organizations may afford opportunities to address social integration.
Supplemental Material
sj-docx-1-jia-10.1177_23259582241251728 - Supplemental material for Assessing the Impact of Social Determinants of Health on HIV Care Engagement in the Southern United States: A Cross-Sectional Study
Supplemental material, sj-docx-1-jia-10.1177_23259582241251728 for Assessing the Impact of Social Determinants of Health on HIV Care Engagement in the Southern United States: A Cross-Sectional Study by Maira Sohail, John D. Cleveland, C. Greer McCollum, Kaylee W. Burgan, Larry R. Hearld, Alyssa Carodine, Kendra Johnson, Melvin Fort, Jennifer Thompson, and Michael J. Mugavero in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We thank all the participants and the participating sites.
Disclosures
This study was conducted in accordance with the Declaration of Helsinki. Approval was granted on November 13, 2020. The Institutional Review Board (IRB) at the University of Alabama at Birmingham acted as the central IRB, whose review was accepted by all participating institutions’ IRBs (IRB-300006212). The central IRB determined that this research involved no greater than minimal risk and approved a waiver for informed consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Merck Company Foundation, (grant number CCO-19-13414)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.