
Abstract
This study evaluated how educational attainment impacts clinical outcomes of HIV-positive patients in Durban, South Africa. The authors conducted a prospective study of 466 adult HIV-positive patients initiating antiretroviral therapy (ART) at an urban TB-HIV clinic from October 2004 to June 2007. The level of educational attainment (highest grade completed) was assessed at ART initiation. The authors measured tuberculosis treatment outcomes as well as death, lost to follow-up, viral suppression (HIV RNA <400 copies/mL), and immunologic response (CD4 ≥200 cells/mm3) at 6, 12, and 24 months after ART initiation. After 24 months of ART initiation, there were 43 deaths; viral suppression and immunologic response were observed in 88% and 83% of the remaining patients, respectively. The authors found no association between level of educational attainment and mortality (P = .12), loss to follow-up (P = .85), virologic response (P = .51), or immunologic response (P = .63). Similar findings were observed at 6 and 12 months post-ART initiation.
Introduction
Clinical outcomes among patients with HIV and tuberculosis (TB) are influenced by demographic, biological, and socioeconomic factors. 1 –5 Understanding how these factors impact clinical outcomes is important to improve treatment efficacy and reduce morbidity and mortality. Universal primary education is a key socioeconomic factor prioritized by the United Nation’s Millennium Development Goals (MDGs 2). 6 It is important to consider how investments in education will synergize with investments in other MDGs aimed at combating HIV and TB.
The mechanism by which education impacts clinical outcomes of HIV and TB is complex and perhaps mediated by differences in disclosure, access to treatment, retention in care, and adherence. 7 –12 Education level affects health literacy and may determine the type of health-seeking behavior necessary to achieve favorable treatment outcomes. 13 A comprehensive search revealed a paucity of literature on education and clinical outcomes for HIV and TB; some studies conclude that an association exists, 5,7 –10,14 and others draw the opposite conclusion. 9,15
Whether educational attainment, defined as the highest level of schooling completed, affects TB and HIV treatment outcomes is unclear in sub-Saharan Africa (SSA), a region facing the world’s highest burden of HIV and TB and the lowest literacy rates; 38% of the adults lack basic literacy, and there are over 21 million out-of-school youths. 16 South African census data indicate that 25% of the adult females are illiterate and that among 17- to 22-year-olds, only 13% and 34% have completed secondary school in rural and urban communities, respectively. 17 When antiretroviral therapy (ART) was introduced in SSA, there was concern that a poor, uneducated patient population would have difficulty with adherence, which would facilitate the spread of drug resistance. 18,19 Several studies have since demonstrated high adherence in this population. 20 –23 This finding challenges the notion that education dictates adherence and calls into question whether socioeconomic disadvantages, such as food insecurity, unemployment, poor social support, and limited access to education really constrain SSA patients’ likelihood of treatment success.
This study aims to describe the level of educational attainment among HIV-infected patients enrolling into an urban integrated TB-ART rollout program and to correlate the level of educational attainment with treatment outcomes.
Methods
This was a prospective chart review of 512 patients, consecutively enrolled into HIV care from October 2004 to June 2007 at the Centre for the AIDS Programme of Research in South Africa (CAPRISA) eThekwini HIV-TB clinic. Patients were eligible for inclusion if they were HIV-positive, ART naive, and at least 18 years old. TB-HIV coinfection was present in 128 (27.5%) patients either at ART initiation or during follow-up.
Prior to initiating ART, health care workers (HCW) administered questionnaires to patients, capturing demographic and socioeconomic information. Patients were grouped into 4 educational levels: primary school or less, some secondary school, completed secondary school, or attended college or university.
South African TB and HIV guidelines were used for all the patients in the study. 24,25 Patients presented for clinical review and adherence assessment weekly for the first 2 weeks of treatment and monthly thereafter. Health education and adherence literacy were standard of care at each study visit. Laboratory assessments were performed at screening and every 6 months, unless clinically indicated. Monitoring for TB sputum conversion was performed at screening, after the intensive phase of TB therapy, 1 month before the end of TB therapy, and whenever clinically indicated.
Definitions of immunologic and virologic response were based on the World Health Organization (WHO) guidelines. 26 Data were routinely collected by program staff, captured using standardized templates, and entered into a study database.
Fisher exact tests and analysis of variance were used to compare differences in categorical and continuous data between the different education groups. An adjusted P value was calculated using generalized estimating equation models. A square root transformation was applied to CD4 count to ensure normality when comparing change from baseline between the education groups. Multivariate proportional hazards models were used to assess mortality and, separately, immunological response between low- and high-education groups. Stratified analyses for each education group and gender were also performed. All analyses were performed using SAS statistical software version 9.3 (SAS Institute Inc, Cary, North Carolina). The study was approved by the University of KwaZulu-Natal Biomedical Research Ethics Committee (E248/05).
Results
Patients
Of the 512 patients initiated on ART from October 2004 to June 2007, 466 reported their education level. Forty-six patients with incomplete records were excluded. Primary school education or less was reported by 72 (15.5%) patients, some secondary school by 206 (44.2%), completed secondary school by 148 (31.8%), and attended college or university by 40 (8.6%; Table 1).
Baseline Characteristics of Patients.

Abbreviations: IQR, interquartile range; SD, standard deviation; WHO, World Health Organization.
a P value adjusted for other variables displayed in the table.
b Plus–minus values are means ± standard deviation.
c Data on race and occupation were not available for 1 patient.
d Data on median number of children were not available for 33 patients.
e Data on history of TB were not available for 7 patients.
f The Karnofsky performance score is a measure of the patient’s general condition and degree of autonomy on a scale ranging from 0 to 100, with lower numbers indicating poorer function. Data were not available for 2 patients.
g CD4 count at baseline were not available for 8 patients.
h Log viral load at baseline were not available for 62 patients.
Compared to patients with primary school education or less, patients who had attended college or university were significantly younger (mean age 31.1 versus 40.1, P < .01), more likely to be employed (57.5% versus 38.9%), and less likely to be unemployed (25.0% versus 61.1%; P < .01). Highly educated individuals had fewer children than patients with less education (2 versus 1, P < .04), but there were no other statistically significant differences between the education groups (Table 1).
Outcomes of HIV and TB Treatment
The proportion lost to follow-up by 24 months was 8.8% and had no association with educational level at 6 (P = .64), 12 (P = .72), and 24 months (P = .85). The number of deaths roughly doubled in each educational group between 6 and 12 months, with 80% of all deaths occurring within the first year of treatment and 43 deaths cumulatively by 24 months. There was no significant association, however, between the education level and the mortality rate by 6 (P = .76), 12 (P = .47), and 24 months (P = .12; Table 2).
Clinical Outcomes of HIV and TB Treatment.

Abbreviations: ART, antiretroviral therapy; IQR, interquartile range; TB, tuberculosis.
a Lost to follow-up is defined as defaulting treatment or not being seen by clinic staff in more than 6 months (excluding deaths, relocations, and transfers).
b Virologic suppression defined as HIV RNA <400 copies/mL.
c CD4 ≥200 cells/mm3 was the definition of immunologic response.
d P Value for median increase in CD4 count was adjusted for baseline CD4 count.
e Number of individual TB cases includes patients with more than 1 episode of TB during follow-up.
f TB cure was defined as a patient who is smear negative at, or 1 month prior to, the completion of treatment and also on at least 1 previous occasion.
g Successful completion of treatment was defined as the use of more than 85% of the prescribed medication.
h Treatment success was defined as TB cure and successful completion of treatment.
i Treatment failure was defined as a positive smear or culture for Mycobacterium tuberculosis that was obtained at least 5 months after the initiation of TB therapy.
In a multivariate model, those with higher levels of education (completed secondary school or more) were no more likely to die than those with lower levels of education (some secondary school or less), after adjusting for age, gender, occupation, history of TB, baseline Karnofsky score, CD4 count, viral load, and the WHO staging (hazard ratio [HR] = 1.76; 95% confidence interval [CI], 0.84-3.70). Among patients with higher levels of education, baseline CD4 count (HR = 1.85; 95% CI, 1.07-3.17) and the WHO stage 4 disease (HR = 3.06; 95% CI, 1.19-7.92) were predictors of mortality (Table 3).
Multivariate Regression Analysis of Risk Factors for Mortality and Immunologic Response, Stratified by Education Level and Gender.
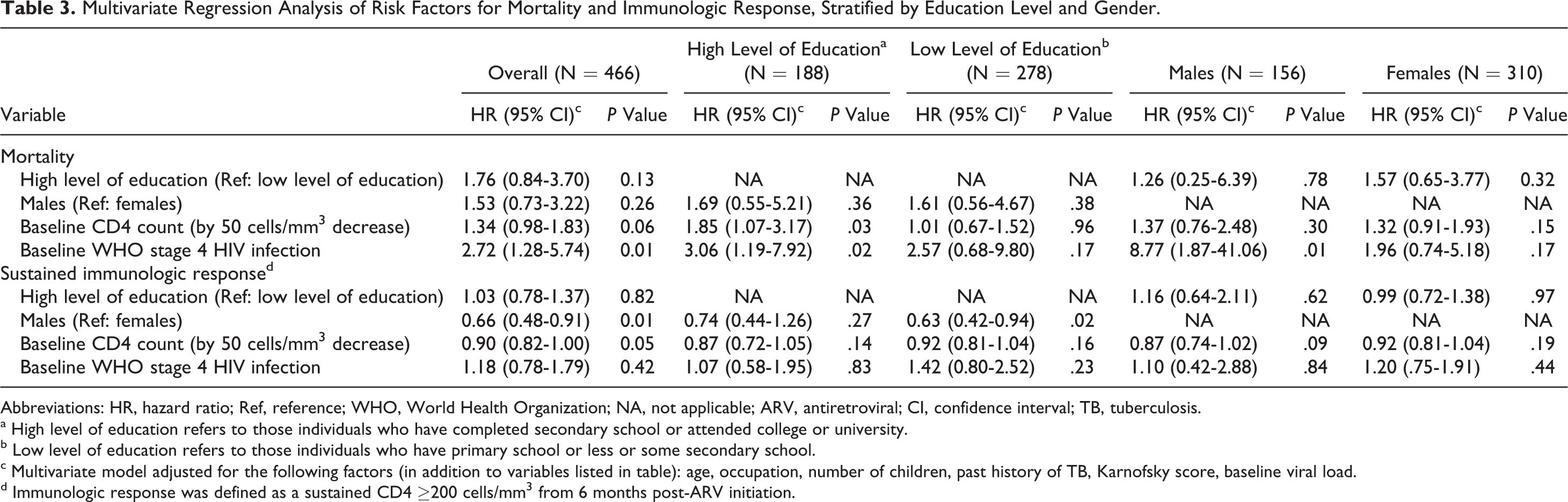
Abbreviations: HR, hazard ratio; Ref, reference; WHO, World Health Organization; NA, not applicable; ARV, antiretroviral; CI, confidence interval; TB, tuberculosis.
a High level of education refers to those individuals who have completed secondary school or attended college or university.
b Low level of education refers to those individuals who have primary school or less or some secondary school.
c Multivariate model adjusted for the following factors (in addition to variables listed in table): age, occupation, number of children, past history of TB, Karnofsky score, baseline viral load.
d Immunologic response was defined as a sustained CD4 ≥200 cells/mm3 from 6 months post-ARV initiation.
There was no significant difference between educational groups in terms of the proportion of patients who were virologically suppressed at 6 (P = .42), 12 (P = .82), and 24 months (P = .51), or the proportion with an immunologic response, which ranged from about 50% at 6 months to 80% at 24 months. After adjusting for baseline CD4 count, however, the median increase in CD4 count at 24 months was 62 cells/mm3 higher in patients who had attended college or university compared to those with primary school education or less (P = .06; Table 2).
In the multivariate model, patients with higher levels of education were no more likely to have a sustained immunologic response than those with lower levels of education (HR = 1.03; 95% CI, 0.78-1.37). Among patients with lower levels of education, males (HR = 0.63; 95% CI, 0.42-0.94) were less likely to achieve a sustained immunologic response than females (Table 3).
There were 144 TB episodes among 128 patients either at baseline or during follow-up. The TB outcomes did not differ significantly between the educational groups (Table 2).
Discussion
We found excellent clinical outcomes for TB and HIV regardless of the education level. The virologic suppression achieved early in a high proportion of patients was consistently maintained throughout the follow-up. Additionally, there was no significant difference in mortality or immunologic response among the different educational groups at any time point (Table 2). Past, baseline, or incident TB were not associated with educational level, suggesting that in a TB endemic setting, HIV infection puts patients at an equal risk of TB, irrespective of the level of education (Table 1).
The available literature provides no consensus about the role of education and TB- and HIV-related health outcomes. Some studies conclude that educational attainment affects CD4 T-cell response, TB treatment success, and HIV- and TB-related mortality, 5,7 –10,14 while others have found no relationship. 9,15 These studies, all conducted in resource-rich countries, are not generalizable to SSA and do not provide data on patients with HIV-TB coinfection. On the other hand, the link between educational attainment and ART adherence has been observed in both developed and developing settings. 27,28 Yet, its effect on clinical outcomes, the true measure of treatment success, remains poorly understood. This issue is particularly important in SSA, where both TB and HIV are endemic and prevalent in lower socioeconomic populations.
We believe our study is the first to demonstrate the absence of a relationship between education and clinical outcomes in SSA. Educational attainment was not associated with loss to follow-up, mortality, virologic response, or immunologic response at all time points (Table 2). Our findings are surprising, given that education is expected to be a key social determinant of health.
Although educational level did not affect clinical outcomes, baseline CD4 count and the WHO stage 4 disease were strong predictors of mortality in patients with higher levels of education (Table 3). Since this effect was not observed among patients with low levels of education, we believe that these more highly educated patients are presenting for care later in their disease. On the other hand, among patients with low levels of education, males were 37% less likely than females to have an immunologic response (Table 3). This gender disparity is a well-documented phenomenon and highlights the fact that HCWs should identify men with low levels of education to ensure they stay sufficiently engaged in programs through specialized adherence and treatment support. 29 –31
Our study has several strengths that support its validity. Baseline questionnaires were administered by HCWs, eliminating potential bias arising from patients with different literacy levels completing self-administered questionnaires. Previous analyses of educational attainment support the claim that disparities in access to care contribute to higher mortality and poorer clinical outcomes among patients with lower levels of education. 7,8 Importantly, all patients were seen at the same clinic, which provided medical care, counseling services, and ART at no cost. Finally, our mortality outcomes are consistent with findings from other ART programs in SSA; high mortality in the first year of ART is believed to be a consequence of very low CD4 counts and advanced HIV disease at baseline. 32
A limitation of this analysis is that educational attainment was only recorded at baseline. Additionally, program data were only available from 2004 to 2007. Given the investments in education in recent years, it is unclear whether the observed effect will change. 16
We have shown that in the CAPRISA research clinic, a setting where patients have equal access to a high standard of care, any underlying effect of inequities in education can be overcome. Nonetheless, educational attainment and its dismal state across SSA should not be accepted. Only 40% of our cohort completed secondary school, reflecting the overall trends in South Africa (Table 1). 17 Our findings are generalizable to neighboring countries, such as Lesotho and Swaziland, where 38% and 44% of the learners complete secondary education, respectively. 33,34 It is apparent that despite investments in social development and 20 years of democracy in South Africa, the levels of educational attainment remain suboptimal.
Conclusion
Our study demonstrates that a higher level of educational attainment is not a key determinant of short- and medium-term ART and TB treatment success in a resource-limited setting. Yet, education plays a role in acquiring HIV/AIDS; a higher level of educational attainment is important in shaping behavioral risk choices and decreasing the risk of HIV infection. 35 –37 Moving forward, it is important to consider whether our findings will persist over longer periods of follow-up and whether they can be replicated not only in large-scale HIV and TB treatment programs but also in prevention programs.
Footnotes
Acknowledgments
Quarraisha Abdool Karim’s oversight of the Fogarty Program was invaluable, without which this project would not have been possible. We gratefully acknowledge the participants in the study and the contributions of the CAPRISA AIDS Treatment Program team and staff of the Prince Cyril Zulu Communicable Disease Centre for providing clinical care of study patients. Finally, we thank Nonhlanhla Yende for her statistical support and Tanuja Gengiah for her overall guidance and advice.
Authors’ Note
GC and KN developed the idea for the article, and GC was the primary author of the article. KN and GC structured the analysis plan, analyzed the data, helped to develop the main argument, and edited the article. SG assisted with data collection and collation. LW conducted the statistical analysis and also edited the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: GC was supported by the National Institutes of Health Office of the Director, Fogarty International Center, Office of AIDS Research, National Cancer Center, National Eye Institute, National Heart, Blood, and Lung Institute, National Institute of Dental and Craniofacial Research, National Institute on Drug Abuse, National Institute of Mental Health, National Institute of Allergy and Infectious Diseases, and National Institutes of Health Office of Women’s Health and Research through the Fogarty International Clinical Research Scholars and Fellows Program at Vanderbilt University (R24 TW007988) and the American Relief and Recovery Act. CAPRISA was established as part of the Comprehensive International Program of Research on AIDS (CIPRA; grant # AI51794) from the US National Institutes of Health. The US President’s Emergency Plan for AIDS Relief (PEPfAR) funded the care of all the participants in the trial. The Global Fund to fight AIDS, Tuberculosis, & Malaria funded the cost of the drugs used in the trial. The research infrastructure to conduct this trial, including the data management, laboratory, and pharmacy cores were established through the CIPRA grant. KN received grant funding from the CAPRISA AIDS TREATMENT Programme (grant # 5U33GPS001350) and The TRuTH Study (TB Recurrence upon Treatment with TB Therapy and HAART) (grant # ZA.09.0263).