
Abstract
Introduction
As HIV remains a global public health issue affecting over 38 million people at the end of 2021, with sub-Saharan Africa accounting for up to two-thirds of new cases of the disease, many more strategies for its curtailment need to be considered.1,2 Global AIDS-related deaths in 2020 were estimated at 680,000 with sub-Saharan Africa being the most affected. 2 More so, in 2019 the Nigerian National Agency for the Control of AIDS estimated that 1.9 million people were living with HIV in Nigeria. 3 Since the 1990s, the introduction of Highly Active Antiretroviral Therapy has modified the clinical course of HIV infection, reducing the rate of disease progression, the incidence of opportunistic infection and mortality.4,5
The index case of COVID-19 was confirmed on the February 27, 2020 and was the first case to be reported in Nigeria since the beginning of the outbreak in China in January 2020. 6 As of November 2022, globally, 634,522,052 confirmed cases of COVID-19 with 6599.100 deaths had been reported. 7 As the COVID-19 pandemic gained momentum across the world with many countries, including Nigeria, gradually reopening after going on lockdown at the time of our study, there arose fears that people living with HIV (PLHIV) might not have access to antiretroviral therapy (ART) and the quality of care given might be disrupted. 6
The advancement and availability of ART have significantly decreased the incidence of morbidity and mortality associated with AIDS, resulting in the conversion of HIV into a chronic illness that necessitates consistent, life-long care. As a result, the treatment of uncomplicated HIV infection is generally uncomplicated, provided that it is appropriately managed. However, complex cases may arise, including HIV/TB co-infections, other syndromic conditions, and treatment failure.8,9 Despite all these, the progressive supports exhibited by the healthcare providers in conjunction with PLHIV and their caregivers need to be examined for possible improvement of their quality of life. Healthcare services have primarily focused on treating the diagnosis at hand, and care providers may not recognize the impact the quality of care has on the physical, social, and mental health wellbeing of PLHIV, as well as on treatment compliance. Measuring the quality of care among PLHIV is essential for monitoring the burden of disease, the impact of treatment and evaluating the barriers to accessing good quality care from the perspectives of PLHIV which remains key in ensuring long-term engagement and retention in care and eventual epidemic control.8,9
WHO has defined quality of care as the degree to which health services of individuals and populations increase the likelihood of desired health outcomes. 10 It is focused on evidence-based professional knowledge and is critical for achieving universal health coverage. 9 Research has shown that the quality of services provided ensured that patients are effectively linked to care with mechanisms put in place to retain them. 8 Factors such as limited economic accessibility, poor staff communication, long waiting times, unavailability of services, and stigmatizing practices, play a major role in influencing how PLHIVs perceive the quality of care received. 11 Consequently, poor quality of care can translate into decreased quality of life. 12 As a result of these, care and treatment of PLHIV are gradually shifting from just increasing life expectancy to finding ways to improve nonhealth-related determinants that may act as barriers to accessing quality care. 13 The issue of the client's satisfaction can be used as an indicator of healthcare quality because the more satisfied the patients are, the more likely it is that they will cooperate with the healthcare provider which will in turn result in improvement in clinical outcomes and overall quality of life.14,15 Previous studies have shown that the satisfaction of clients is associated with increased retention in the cascade of HIV care.16,17 Furthermore, perception of the quality of care includes accessibility, affordability, and interactions with service providers and this determines clients’ satisfaction with HIV services.18‐20 It is opined that the understanding of what patients perceive to be good ART-related clinical care and exploration of what is responsible for these perceptions will be a vital tool in improving HIV care. Understanding the quality of care from the perspectives of PLHIV, and how this impacts their ability to engage and be effectively retained in care will be essential in achieving the 95-95-95 targets and ending the HIV epidemic by the year 2030. 13 The goal of this survey was to evaluate patients’ satisfaction with HIV care and treatment and its determinants across the various levels of the service delivery system. The study aimed to identify the main clinical, structural, and social factors influencing the perceptions of quality of care among PLHIV in Lagos Nigeria during the early phase of the COVID-19 pandemic.
Methodology
The Setting, Study Design, and Participants
The study was carried out in Lagos State, one of the Southwestern States in Nigeria among participants drawn from 25 primary, secondary, and tertiary healthcare facilities and 5 One Stop Shops that provide HIV care and treatment services with the involvement of local community-based organizations and networks of PLHIV. The One Stop Shop (OSS) is a concept for providing nondiscriminatory HIV and psychosocial services to the Key Population (LGBTQA+). The facility provides HIV testing services, treatment, and care. It also provides HIV prevention services, that is HIV pre-exposure prophylaxis, postexposure prophylaxis, condom and lubricant programming, distribution of Information Education and Communication materials like other facilities, but also provision of free legal services and skill acquisition centers and recreation points in some locations. Lagos State has a prevalence of 1.4% of HIV among the population. 21 The study was carried out during the early phase of the COVID-19 pandemic in Nigeria during which there was a lockdown at some point throughout the country and PLHIVs received their drugs using courier services and other private medical delivery services. And as the lockdown was eased, a multimonth drug prescription system was initiated where long appointments were given to clients. Also, a client was used to collect medications for others living in the same locality after teleconsultations with other clients that couldn't make their physical appointments.
An observational, cross-sectional study design was applied to investigate the perception of quality of care among PLHIV and identify potential differences in these factors between PLHIV subpopulations.
The data was collected over a 2-month time frame, 9 months into the COVID-19 pandemic in Nigeria among selected participants who had a confirmed HIV-positive status, and were 18 years of age and above, living in and accessing care services in the city of Lagos. They must have accessed care or had been on treatment for at least 12 months and were able to respond to an interviewer-administered questionnaire.
Sample Size Determination
The minimum sample size was determined using the standard formula for descriptive studies 22 using a standard normal deviate of 1.96, a P of .5 for maximum variability, and a margin of error of .05. The minimum sample size calculated was 384. Giving allowances for a 20% nonresponse rate, the sample size was increased to 460. A total of 578 PLHIV from all the Key populations of clients receiving treatment in each of the facilities across the state were interviewed.
Sampling
A stratified simple random sampling technique was used based on the gender, age groups, and the different groups of PLHIV from each of the 25 high-burdened health facilities and 5 OSS facilities in Lagos.
Study Instrument
The instrument was an interviewer-administered, pretested questionnaire which was developed from a review of the literature on the subject. The instrument had 4 sections. The first dealt with the sociodemographic characteristics of the respondents, the second assessed the knowledge and attitude of respondents as regards HIV treatments, while the third and the fourth sections instigated the perception of the quality of care among PLHIV and comorbidities assessment, respectively. Face validation of the instrument was done by all the investigators. And the Cronbach's alpha reliability coefficient was 0.71.
Data Collection Technique
Owing to the already established relationship with the study participants, 5 adolescents and young PLHIV (4 from the general population and 1 from the key population) were trained as study mobilizers to conduct face-to-face interviews at the selected health facilities. Individual survey participants were provided with the anonymity paper version of the questionnaire and interviewed by study mobilizers who helped input the answers onto the tablet or provided a paper version of the questionnaire with no follow-up interviews or other interventions. All survey responses were eventually inputted into the web-based version of the questionnaire deployed via survey monkey developed especially for the study and compatible with all mobile platforms, this was to mitigate the challenges of a paper-based survey for areas with limited connectivity or preference for the paper version.
Variables
For this study, the outcome variable was the perception of quality of care received by the PLHIV with key domains related to the provision of quality healthcare services including HIV counseling, the commencement of ART, whole-person care, and so on. The independent variables were sociodemographic and economic characteristics.
Data Management
Completed questionnaires from the web platform were cleaned and coded on Microsoft Excel 2016 and were exported to STATA SE 12 (STATA CORP LLC, College Station, TX, USA) where it was analyzed. For perception of quality of care, 10 questions were asked and desirable answers were scored = 1, undesirable answers = 0, and the perception was graded, as ≤70% poor, >70 good. 23 Two-sample Wilcoxon Rank Sum (Mann-Whitney) test and Kruskal-Wallis equality-of-populations rank test were used to assess the association between respondents’ perception scores on the quality of care and their sociodemographic characteristics. Ten questions were asked on respondents’ attitudes toward HIV medication, and were scored using a 5-point Likert scale; (5) agree completely, (4) somewhat agree, (3) neither agree nor disagree, (2) somewhat disagree, and (1) disagree completely. The attitude was graded, as ≤70% poor and >70 good. 22 The level of significance was set at P < .05.
Ethical Considerations
Ethical approval was from the Health Research Ethics Committee to carry out this study with approval number LREC/06/10/1390. An electronic and paper-based written consent was obtained from each respondent with the assurance of confidentiality of the information and their right to withdraw from the study at any point in time. Only the patient ID numbers of the sampled ART patient were used. The participants were made to understand that involvement was voluntary and the study pose no risk to them.
Results
About 69.5% were aged 30 years and above with a mean of 38.56 ± 12.0 years. About 60% and 61% were females at birth and after birth, respectively. More than half (53%) were either unemployed or unskilled workers and close to 6% were sex workers. Only about a third (39.6%) was skilled or professional workers while more than 83% had completed secondary education. About 39% had 5 or more people living in their household with a mean of 4.07 ± 1.95 persons. More than one-third (35.3%) earn ₦30,000 or less. A majority (83%) of the respondents stated that they had very good to excellent health status (Table 1).
Sociodemographic Characteristics of Respondents.

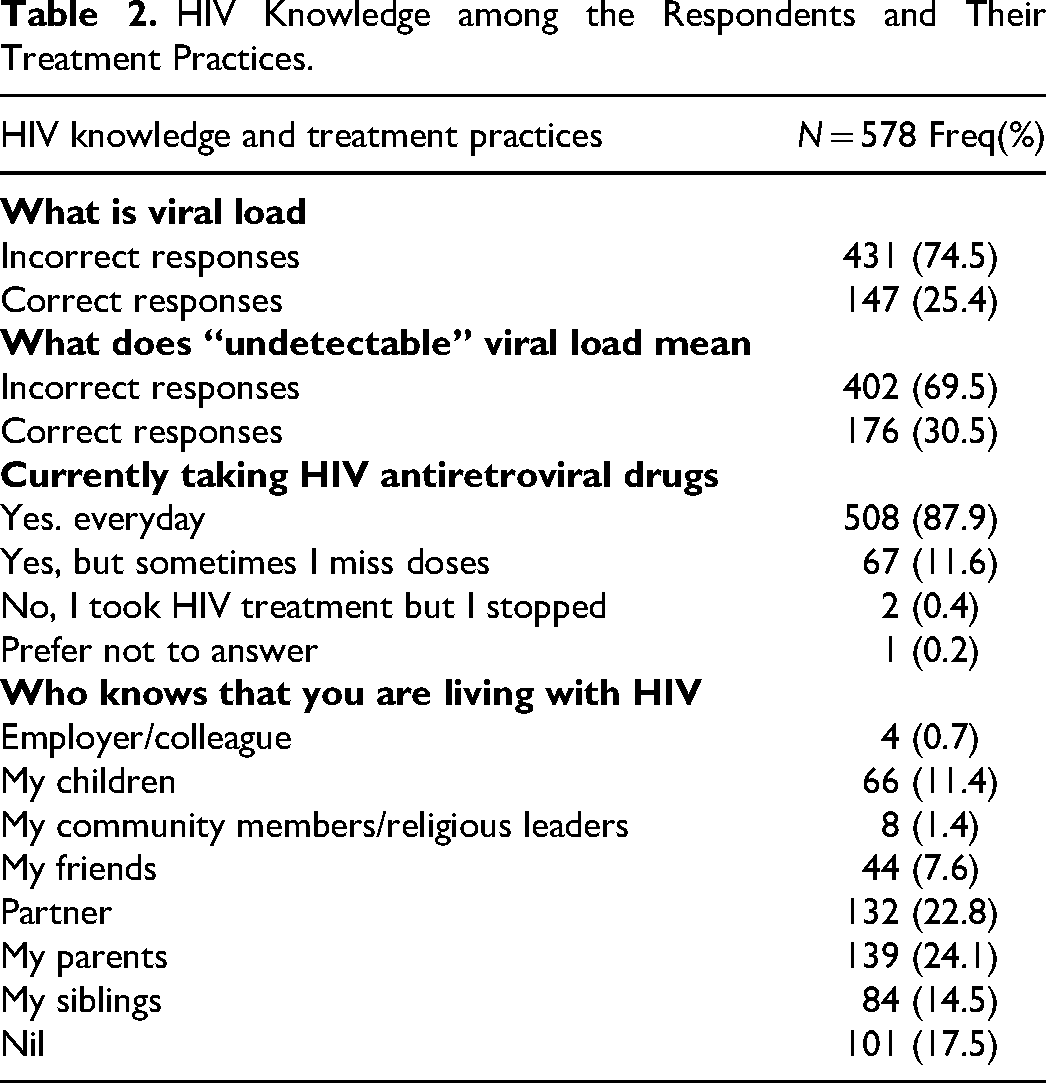
Most (74.5%) of the respondents gave incorrect responses on the definition of viral load and only about 30.5% had correct responses on the meaning of undetectable viral load. The majority (87.9%) currently took their HIV antiretroviral drugs every day and only 22.8% told their partners about their HIV status (Table 2).
HIV Knowledge among the Respondents and Their Treatment Practices.
Approximately 78% were willing to know more about HIV and HIV treatment, and only about 11.2% somewhat agreed or agreed completely that the number of pills that they take for HIV makes their life difficult. The majority (87.9%) of them somewhat agreed or agreed completely to understand the importance of taking their HIV medications every day. Almost all (98.4%) concurred that their healthcare provider had spoken to them about how HIV is transmitted and more than two-fifths (43.1%) of the respondents said that as of the previous year, the doctor checked their viral load twice. The majority (95.0%) had been educated on HIV prevention in the previous year. However, close to two-thirds (60.9%) of respondents stated that their healthcare providers never asked about their current life situation and most (87.2%) felt that the people at their health clinics were unfriendly, rude or unwelcoming. Overall, 95.5% of the respondents had a good perception of the quality of care they received (Tables 3 and 4), and 88% had a good attitude toward their HIV care (Figure 1).

Respondents’ attitude toward their HIV treatment.
Respondent's Attitude Toward HIV Treatment.
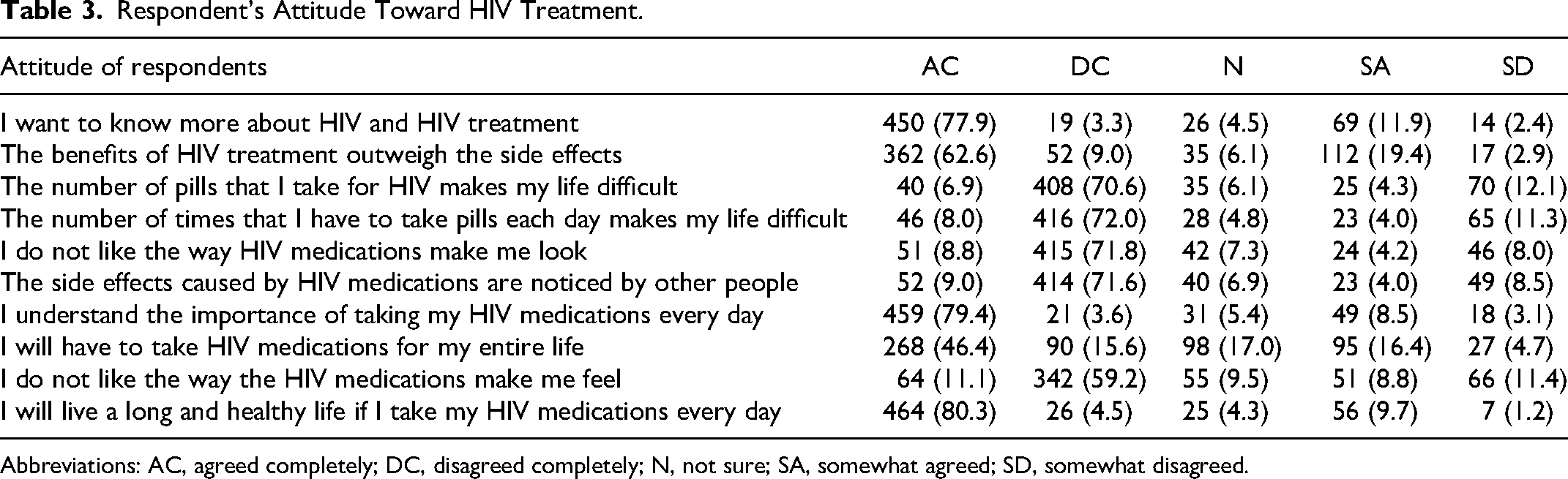
Abbreviations: AC, agreed completely; DC, disagreed completely; N, not sure; SA, somewhat agreed; SD, somewhat disagreed.
Respondent's Perception of HIV Quality of Care.
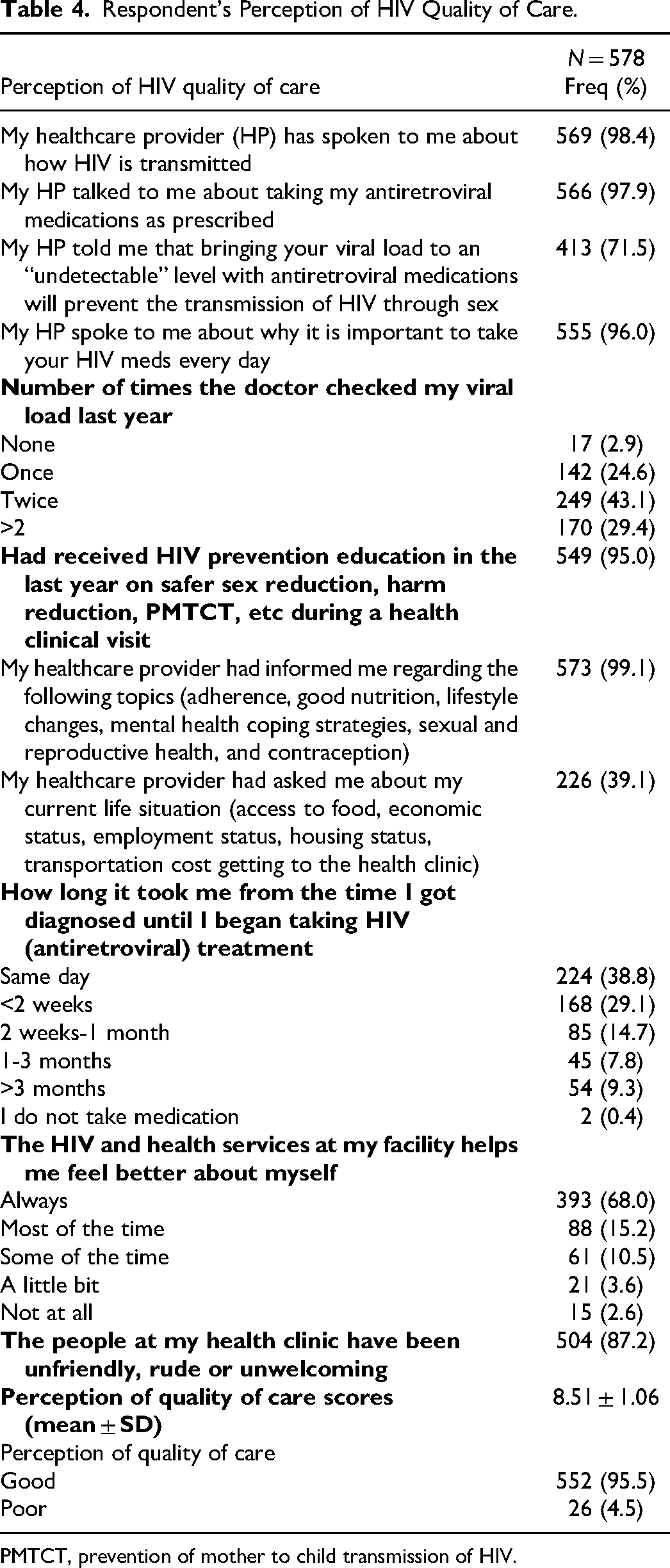
PMTCT, prevention of mother to child transmission of HIV.
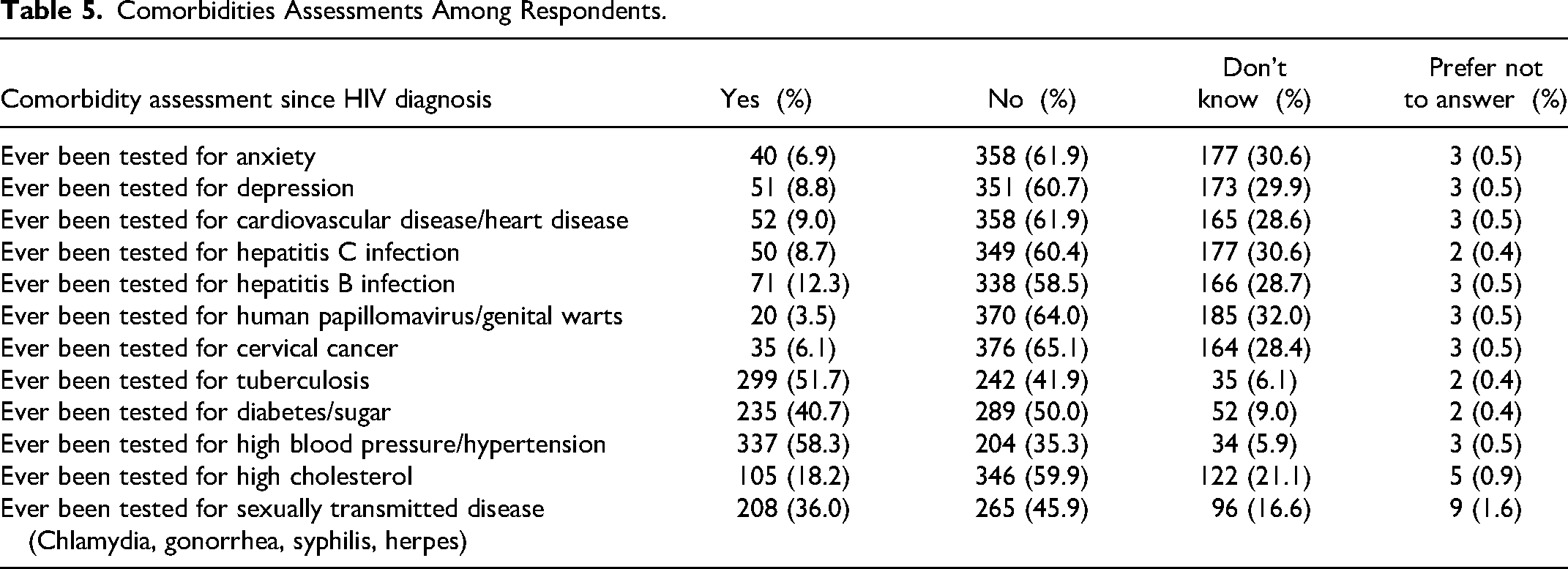
Since HIV diagnosis, approximately 61% had never been assessed for depression, 52% for tuberculosis/TB and almost half (46%) had never been tested for Sexually transmitted diseases (Chlamydia, gonorrhea, syphilis, herpes) (Table 5).
Comorbidities Assessments Among Respondents.
Age group, level of education, occupation, personal monthly income, number of people in a household, and the treatment groups of respondents were statistically significantly associated with the perception of quality of care among PLHIV. Those with a higher level of education, skilled/professionals, and those with higher monthly income had a statistically significantly higher perception of quality of care compared to others (P < .005; Table 6).
Relationship Between Respondent's Sociodemographic Characteristics and Their Perception of HIV Quality of Care.

*5% Significance interval.
Discussion
It's important to acknowledge that the COVID-19 pandemic era may affect the level of care received by patients. This is noteworthy as research has shown that the quality of healthcare services can greatly impact the success of health programs, particularly for individuals living with HIV. 24 In line with this are the findings from a study conducted in Bangladesh which reported that the availability of effective communication and good interpersonal skills are essential in improving the quality of care as compared to just the technical competence of the provider. 25
According to the results of our study, a considerable proportion of individuals living with HIV and AIDS are aged less than 30 years. Specifically, our findings indicate that approximately 30.5% of people living with HIV and AIDS are below the age of 30. This is almost similar to a study done in another southwestern state of Nigeria which reported that close to 30% for that age group as well. 26 This suggests that young people are still a particularly vulnerable group. Given the high prevalence of HIV and AIDS among young individuals, it is crucial to prioritize prevention and education initiatives that target this population.
In this study, almost all (95.5%) had a good perception of HIV quality of care and this is similar to the findings of a study conducted in Southwestern Nigeria (95.2%).26,27
The present investigation, along with other studies, has revealed that factors such as the age of the respondents, their level of education, occupation, the number of individuals inhabiting the same household, and social group are critical determinants of the perception of care quality among PLHIV.26‐28 Consequently, it is imperative to consider the sociodemographic attributes as a whole while formulating policies aimed at enhancing the quality of healthcare services.
One of our findings is that the majority (87.2%) of health workers at their clinic were unwelcoming, rude, and unfriendly. This is contrary to the findings from a study conducted in South Eastern part of Nigeria that reported almost all the patients (98%) thought that the health providers who attended to them were very polite. 29 It is important to note that good communication and politeness positively impact patient satisfaction. Patients are likely to follow medical advice and never miss appointments when they are attended to politely. 29 Findings from another study suggest that patients who had an opportunity to ask their healthcare provider questions and were happy with the explanations provided were more likely to be satisfied with the healthcare services they received. 30 This approach of a good relationship between PLHIV and their healthcare providers has contributed a larger quota to the adherence to medications and the retention of patients in care thereby improving their quality of life.
Furthermore, promptness in the initiation of antiretroviral medications is one of the strategies utilized to improve how these patients do well in care.26,27,31 The findings of our study indicate that about a third of individuals living with HIV and AIDS delay the initiation of treatment after receiving their diagnosis. Specifically, the study revealed that only 39% of patients initiated treatment immediately after being diagnosed as HIV positive, and another 29% within 2 weeks which is the stipulated period according to the National Guideline. The implications of delayed initiation of treatment are well-documented in the literature, with evidence suggesting that early treatment is critical in improving clinical outcomes and reducing the risk of HIV transmission. The delay in treatment initiation observed in some of the respondents in this study may reflect a lack of awareness or stigma surrounding HIV and AIDS, which may prevent patients from seeking timely medical care. It should be noted that this is unrelated to the COVID-19 pandemic as all the respondents included in this study must have initiated treatment at least 12 months before the study. The pandemic started 9 months into the study. However, this supports the results of a different study that provides proof that numerous individuals who have been diagnosed with HIV seek healthcare services several years later, despite the Centers for Disease Control and Prevention's (CDC) suggestion for routine testing for individuals between the ages of 13 and 64 and immediate commencement of treatment for the positive diagnosis.31,32 Initiating ART early is particularly important for patients with AIDS-defining conditions, those with acute or recent HIV infection, and individuals who are pregnant; delaying therapy in these subpopulations has been associated with high risks of morbidity, mortality, and HIV transmission which can compromise their level of quality of care.32,33
In addition, another vital area to consider is the viral load of these patients. Several lines of evidence have established that virally suppressed HIV individuals have a reduced risk of transmitting HIV to their HIV-negative partners (discordant partners) and those with undetectable viral levels pose no risk of HIV transmission.34‐36 But in this study, the evidence of undetectable viral load levels among the participants was 49.8%. Nonetheless, this would require massive interventions including increased enrollment and consistent surveillance of the importance of viral load monitoring.
Despite an overall good attitude and perception of ART, a significant proportion of the participants were not convinced of the effectiveness of ART or understood its importance as a daily medication for life long. Similar findings were obtainable in studies conducted in Madagascar and sub-Saharan Africa.37,38 These patients need to be closely monitored as they may be at high risk of discontinuing ART which leads to an interruption in treatment. Educational interventions, as well as psychological support, should be a continuous process in addressing retention in care issues to improve their quality of life.
Although a greater percentage of 87.9% were currently taking their HIV antiretroviral drugs, nondisclosure was seen in 17.5% of respondents. This nondisclosure can detrimentally affect their level of performance and invariably negatively affect the quality of care.
Systems for quality management and quality improvement are critical to addressing the gaps along the care cascade of HIV/TB comorbidities.39,40 Quality TB and HIV services include screening for HIV and TB with appropriate tests and access to their relevant prevention services. Effective care will include timely identification of both HIV and TB, linkage to appropriate treatment and continued clinical and laboratory monitoring until favorable outcomes are achieved. Among the study participants, only 37.2% were tested for TB with just about two-thirds placed on TB preventive therapy. Contrarily, some studies on the review of TB preventive therapy uptake demonstrated that cohorts from low-and-middle income countries had lower TB preventive therapy completion rates compared to cohorts from high-income countries.39,40
The expectations of patients from the healthcare providers and healthcare system play a significant role in the concept of the quality of care received. Quality of care has been defined as the degree to which health services for individuals and populations increase the likelihood of desired health outcomes.10,11 Our study revealed that most of the respondents had a good perception of the quality of care they received with their current health status. Those with a higher level of education, skilled or professionals, and those with higher monthly income had a statistically significantly good perception of quality of care compared to others. Another study revealed that the sociodemographic factors influence the interaction between a provider and the patient and consequently the quality of services obtained, successful quality management implementation requires a significant change in the mindsets, attitudes, and beliefs of individuals. 41
Limitations
As a cross-sectional study, it is difficult to establish any form of causality, however, this study is the first state-wide study known to us that assessed the perception of the quality of services PLHIV received in Lagos during the COVID-19 pandemic. Another limitation of this study includes recall bias, which is a known limitation of questionnaire-based surveys, and social desirability bias as respondents are known to respond positively when relating with others. A proper explanation of the purpose of the study and assuring anonymity helped to minimize the latter. In addition, the study did not assess the quality of service based on the environment of the service delivery. The perceptions measured were generally limited to clinical care and other support for PLHIV.
Conclusions
In general, we described the perception of the quality of care received among patients with HIV and looked at the factors associated with these perceptions. We found out that the majority of the respondents displayed good perceptions and attitudes as regards the quality of care they received at the ART centers in the state. Targeted initiatives are needed to sustain the quality of HIV clinical care, and treatment services to improve the wellbeing of people living with HIV.
Footnotes
Acknowledgments
This survey was made possible through funding for the Joint UNAIDS-IAPAC Fast-Track Cities project through the support of the U.S. President's Emergency Plan for AIDS Relief and the U.S. Agency for International Development. The paper was authored by Adeyinka Adeniran (DCHPH, LASUCOM, Lagos, Nigeria), Yeside Shogbamimu (LSMOH, Lagos, Nigeria), Omobola Y Ojo (FMC Abeokuta, Nigeria), Florence C Chieme (PGC Lagos, Nigeria), Helen O Olowofeso (IAPAC, FTCI Washington, DC, USA), Oladipupo Fisher (LSACA, Lagos, Nigeria), Monsurat Adeleke (LSACA, Lagos, Nigeria), and Imane Sidibé (IAPAC, Washington, DC, USA). Survey outreach was assisted by study mobilizers from APYIN Lagos, Nigeria: Emerald Cheni-Naya Nnoruka, Kosisochukwu Umeh, Odey Benjamin, Afolabi Toluwani Benjamin, and Bello Omotoyosi Adegoke. The authors wish to thank the leadership of Lagos State through the Fast-Track Cities steering committee and the teams at the Lagos State Ministry of Health, Lagos State AIDS Control Agency, Lagos State Primary Healthcare Board and Lagos State Health Service Commission, whose support concerning disseminating the cross-sectional survey was critical to the successful survey implementation. The authors also express their gratitude to the survey participants whose perspectives from the city of Lagos provided a snapshot of the current QoC landscape and informed this paper's recommendations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the U.S. President’s Emergency Plan for AIDS Relief, United States Agency for International Development.