
Abstract
Objectives:
We determined the proportion and correlates of self-reported pregnancy planning discussions (that is preconception counseling) that HIV-positive women reported to their family physicians (FPs), HIV specialists, and obstetrician/gynecologists (OB/Gyns).
Methods:
In a cross-sectional substudy, HIV-positive women of reproductive potential were asked whether their care providers discussed pregnancy planning. Logistic regression was used to calculate odds ratios for the correlates of preconception counseling.
Results:
A total of 431 eligible participants (median age 38, interquartile range = 32-43) reported having discussion with a physician (92% FP, 96% HIV specialists, and 45% OB/Gyns). In all, 34%, 41%, and 38% had their pregnancy planning discussion with FP, HIV specialist, and Ob/Gyns, respectively; 51% overall. In the multivariable model, significant correlates of preconception counseling were age (P = .02), marital status (P < .01), number of years living in Canada (P < .001), and age of youngest child (P < .01).
Conclusions:
Preconception care in our cohort was suboptimal. We recommend that counseling on healthy preconception should be part of routine HIV care.
Introduction
The reduced mortality and morbidity due to HIV through the use of antiretroviral therapy (ART), including lowering vertical transmission rates to <1% if HIV-positive pregnant women receive care and lowering rates of transmission between partners, combined with the innate desire of most to want children, have led many HIV-positive women around the globe to consider pregnancy. 1 –11 Although not an option previously supported by the medical community with many health care providers (HCPs) counseling HIV-positive patients against pregnancy and thereby contributing to the barriers to fertility care access, pregnancy planning is now widely accepted. The acceptance of HIV and pregnancy planning is evident by the many commentaries and publications written supporting the reproductive rights of women living with HIV. 12 –23 Health care workers are now encouraged to advocate for informed choice counseling for their patients living with HIV, and pregnancy planning guidelines are emerging globally. 12 –23 Despite this movement to support safer planned reproduction for HIV-positive women, it is unclear whether discussions regarding preconception, pregnancy planning, and pregnancy are occurring between HCPs and their HIV-positive female patients. We do know that the rates of pregnancies in HIV-positive women are increasing over time in many countries around the world and that many of these pregnancies are unintended. 14,19 –21,23 –32
The discussions about preconception and pregnancy planning that occur between HCPs and their HIV-positive female patients are crucial to counsel not only on the prevention of vertical transmission but also on the prevention of horizontal transmission between partners, optimizing ART for the woman including avoiding potentially teratogenic drugs 12,33 and promoting healthy preconception to reduce maternal and fetal complications. 12 Although promoting healthy preconception is important to all pregnancies, these additional considerations make counseling in the context of HIV even more essential. The recently updated Department of Human Health Service (DHSS)’s Perinatal HIV Guidelines 12 have new recommendations to discuss reproductive intentions with all women of reproductive age on an ongoing basis throughout the course of their care.
In a small study designed to address unmet needs in reproductive counseling in the Baltimore area, Finocchario-Kessler and colleagues asked HIV-positive women whether HCPs were discussing their reproductive plans. 34 Of the 181 predominately African American HIV-positive women surveyed, 67% reported a general discussion about pregnancy and HIV, but only 31% reported a personalized discussion about future reproductive plans. 34 Although a significant proportion of HIV-positive women wanted to discuss reproductive plans with their HCPs, many did not have the opportunity. 34,35 The authors emphasize that these are missed opportunities for HCPs to help women safely plan pregnancies. 34,35 This same group partnered with researchers in Brazil to assess similar communications regarding reproductive intentions between HIV-positive women in Rio de Janeiro and their HCPs. 36 As in Baltimore, the majority of women in clinical care had not discussed future reproductive wishes with their HCPs, suggesting the lack of discussion about pregnancy is widespread. 34,36
We conducted an analysis in a large diverse sample of HIV-positive women of reproductive potential living in Ontario, Canada, to determine the proportion and correlates of self-reported discussions regarding pregnancy planning with their family physicians (FPs), HIV specialists, and obstetrician/gynecologists (OB/Gyns). We believe that pregnancy planning counseling between HCPs and their HIV-positive female patients is a good indicator of the quality of efforts to implement preconception care.
Methods
Study Design and Population
This was a secondary analysis of a larger study, for which the details are reported elsewhere. 5 The main data set was a cross-sectional study using a survey instrument conducted with participants who met the following inclusion criteria: (1) HIV-positive, (2) biologically female, (3) of reproductive age (between the ages of 18 and 52), (4) living in Ontario, Canada, and (5) able to read English or French. 37 The upper age limit was chosen to reflect the cutoff for fertility clinic consultation in Canada. 38 Since the primary outcome of interest for this analysis was preconception care, 2 supplementary exclusion criteria were added (1) women who had a history of tubal ligation or a hysterectomy and (2) women who did not answer the question on pregnancy planning discussions with their HCPs. For interest, women who underwent tubal ligation were assessed separately.
Recruitment, Ethics and Survey Instrument, and Validation
A convenience sample was used with recruitment running from October 5, 2007, to March 31, 2009, through 38 sites across the province of Ontario (reviewed in detail elsewhere). 5 Each research site received ethics approval from their local institutional research ethics board (REB). Written informed consent was obtained from every participant.
A 189-item survey instrument, “The HIV Pregnancy Planning Questionnaire,” was created using the methods of Fowler 39 for instrument development, and content and face validity were assessed as described previously. 5,40,41 The survey was first developed in English and translated into French using the back-translation method. 42 The survey was self-administered with assistance if needed from the research coordinator and took approximately 1.5 hours to complete.
Statistical Analysis and Description of Outcomes and Correlates
The characteristics of the study population were summarized using medians and interquartile ranges (IQRs) for continuous variables, because they were not normally distributed and frequencies and proportions for categorical variables.
The analysis began with questions relating to whether the participants were cared for by an FP, an HIV specialist, and/or an OB/Gyn by asking (1) “Do you have a family doctor?” (2) “Do you see an HIV specialist?” and (3) “Do you see an obstetrician/gynecologist (OB/Gyn)?” The response options for these questions were ‘‘yes’’ or ‘‘no.’’ If participants answered affirmatively to the above-mentioned questions about having the specific HCPs listed, they were asked the following questions to represent preconception counseling: (1) “Has your family doctor talked to you about pregnancy planning?” (2) “Has your HIV specialist talked to you about pregnancy planning?” and (3) “Has your OB/Gyn talked to you about pregnancy planning?” The response options for these questions were ‘‘yes’’ or ‘‘no.’’ This preconception care variable was dichotomized into “preconception counseling” if answered “yes” and “no preconception counseling” if answered “no” and represented the primary outcome of interest.
Additional analyses were carried out, limiting the sample to those women who desired to become pregnant and give birth in the future. Other questions were asked regarding the degree of satisfaction with the amount of pregnancy planning information received from their FP, HIV specialist, or Ob/Gyn using a 5-point Likert-type scale with options of “definitely true,” “somewhat true,” “neither,” “somewhat false,” and “definitely false.”
Univariate logistic regression models were fit to determine the unadjusted odds ratios (ORs) with 95% confidence intervals (CIs) for correlates of preconception counseling. The correlates of interest included age, ethnicity, number of years since immigration for those born outside of Canada, religion, sexual orientation, marital status, living in Toronto, employment status, education, income, duration of HIV diagnosis, HIV risk factor, hepatitis B and hepatitis C coinfection, most recent CD4 count and viral load, antiretroviral status, relationship status, desire and intention to give birth in the future, pregnancy and birth history, and age of youngest child. Variables that were a priori believed to be associated with preconception counseling were examined in univariate analyses and were candidates for inclusion in multivariable logistic regression models for preconception counseling. When multiple covariates measured similar phenomena, the variable representing each construct with the higher effect size and most statistical significance was chosen. We assessed collinearity among pairs of continuous variables with scatterplots, among pairs of categorical variables with frequency tables, and between categorical and continuous variables with boxplots.
We carried out an additional analysis limited to women reporting the use of efavirenz (EFV) to determine whether their HCPs had discussed the potential teratogenic effects of EFV if taken during pregnancy. This analysis was considered to be worthwhile, as the DHSS still recommends that EFV not be used in preconception or in the first 5 to 6 weeks of pregnancy. 12 This outcome was created by first asking participants “Are you currently taking efavirenz (Sustiva)? (This HIV-medication should not be taken during pregnancy)” with an added color picture of all the different pills and capsule forms of EFV. The additional sentence regarding that EFV should not be taken during pregnancy was requested by the REB. If answered affirmatively, participants were asked “Have any of your doctors told you that EFV (Sustiva) is harmful to your baby when you are pregnant?” The response options for these questions were “yes,” “no,” or “I don’t know.”
Statistical analyses were performed using SAS Version 9.3 (SAS Institute, Cary, North Carolina).
Results
Study Population and Survey Validation
A total of 506 HIV-positive women of reproductive age living in Ontario, Canada, were recruited for the overall study. Of the 506 participants, 5 did not meet the inclusion criteria (3 were over the age of 52 and 2 were not living in Ontario). An additional 58 women had a history of tubal ligation or hysterectomy, and 12 women did not answer the question about preconception counseling. This left a sample of 431 HIV-positive women of reproductive potential to be included in the final analysis. As the survey was self-administered, valid answers were not available for all the questions as reflected in the percentage calculations.
The cohort demographics are presented in Table 1. The final study sample had a median age of 38 (IQR 32-43; range 18-52) at the time of the survey. Of the 431 participants, 62% were born outside of Canada, 54% were living in Toronto, 47% defined themselves as being of African ethnicity, 72% were currently on ART. In all, 30% indicated that they had never been married, and 49% stated that they were in a monogamous relationship. Of the study population, 84% had previously been pregnant and 69% had previously given birth with a median number of children in their care of 2 (IQR 1-3). The median age of their youngest child was 8 (IQR 3-14). Similar to the entire cohort, 73% (305 of 416) desired and 63% (257 of 408) intended to give birth to a child in the future. 5
Demographic Characteristics of Eligible Study Participants at the Time of the Survey (N = 431).a

Abbreviations: IDU, injection drug use; VL, viral load; IQR, interquartile range.
a Continuous variables are summarized with medians and IQR; categorical variables are summarized with N (%).
b Denominator varied slightly for each characteristic, missing data was generally <5%, lower response rates were for education, income, years since HIV diagnosis, CD4 count and viral load.
c Recent CD4 count and VL refers to self-reported values closest to the time of the survey.
Quality Indicator of Preconception Care
Of the total of 431 women, 92% had an FP, 96% had an HIV specialist, and 45% had seen an OB/Gyn. Figure 1 outlines the proportion of women reporting that their HCP had a discussion about pregnancy planning with them. Of those with an FP, HIV specialists, and Ob/Gyn, 34%, 41%, and 37% reported that their HCPs counseled them on pregnancy planning, respectively. When combined, a total of 221 (51%) women had any medical HCP discuss pregnancy planning with them. In all, 50 (23%) women reported discussions with their FP, HIV specialists, and Ob/Gyn; 99 (45%) discussed with 2 physicians; and 72 (33%) discussed with only 1 physician. The results are similar for the 305 women who desired pregnancy in the future; the corresponding proportions were 39%, 47%, 44%, and 59% for their FP, HIV specialist, Ob/Gyn, or any medical HCP having discussed pregnancy planning with them, respectively. These low rates of communication regarding pregnancy planning did not appear to impact reported satisfaction with overall care. Although 94% (83%, 89%, 77%) of the participants agree or strongly agree that they are satisfied with the treatment received by any medical HCP (their FP, HIV specialist, Ob/Gyn), only 63% (46%, 56%, 50%) agree or strongly agree that they are satisfied with the amount of pregnancy planning information received.
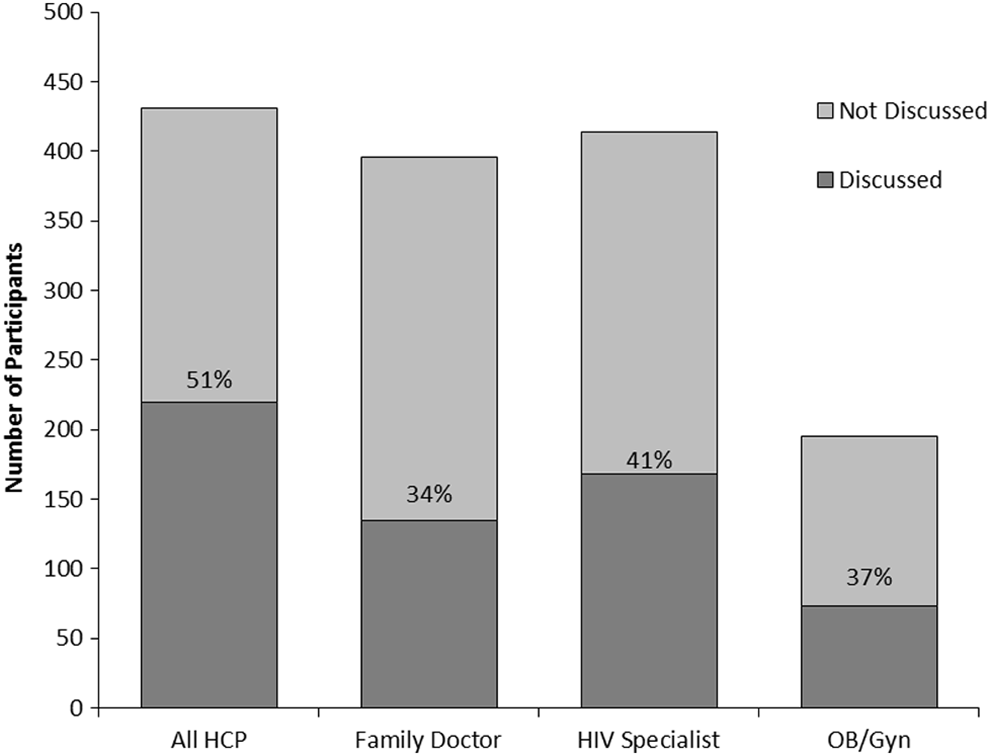
Frequency and proportion of participants reporting preconception counseling with their medical care providers (all health care providers [HCP], family doctors, HIV specialists, and obstetricians/gynecologists [OB/Gyn]).
Tubal Ligation and Pregnancy Intentions and Counseling
As other groups have reported, a significant number of women (10%) in our cohort had a history of tubal ligation. Of the women with tubal ligations, the median age was 39 (IQR, 35-44), 37% were born outside of Canada, and 23% were of African ethnicity. Interestingly, despite prior tubal ligation (n = 52), 42% still desired and 25% intended to become pregnant and give birth to a child in the future. Again for this subset of women who had had tubal ligation, only 36%, 26%, 29%, and 39% of their FP, HIV specialist, Ob/Gyn, or any medical HCP had raised the issue of pregnancy planning, respectively.
Correlates of Preconception Counseling
The results from the univariate logistic regression modeling revealed that significant correlates of reporting preconception counseling were younger age, African ethnicity, being born outside of Canada and number of years living in Canada, living in the Toronto area, married or in a common law relationship or living with a partner, income, shorter duration of HIV infection, having acquired HIV through injection drug use or an unknown source, being coinfected with hepatitis C, number of lifetime births, and age of youngest child in her care (Table 2). A univariate association between pregnancy intentions and preconception counseling (OR = 2.4, 95% CI = 1.6-3.7; P < .01) was found. In the multivariable model, the significant correlates of increased preconception counseling were younger age, being born outside of Canada and fewer years living in Canada, being married or in a common law relationship or living with a partner, and having and/or caring for younger children. This model provided an adequate fit to the data (Hosmer-Lemeshow Goodness of Fit P value = .84).
Distribution of Study Participants and Logistic Regression Analysis for Preconception Counseling among HIV-Positive Women of Reproductive Age (N = 431).a

Abbreviations: CI, confidence interval; IDU, injection drug use; ORs, odds ratios.
a Continuous variables are summarized with medians and interquartile range; categorical variables are summarized with N (%).
b Age, years living in Canada, marital status, and age of youngest child were the variables retained in the multivariate analysis.
Counseling on Teratogenicity of EFV
Of the total 431 women, 60 reported that they were currently taking EFV. Of these women, only 42% reported that any of their medical HCPs had discussed the potential teratogenic effects of EFV if taken during pregnancy. This is outlined in Figure 2.
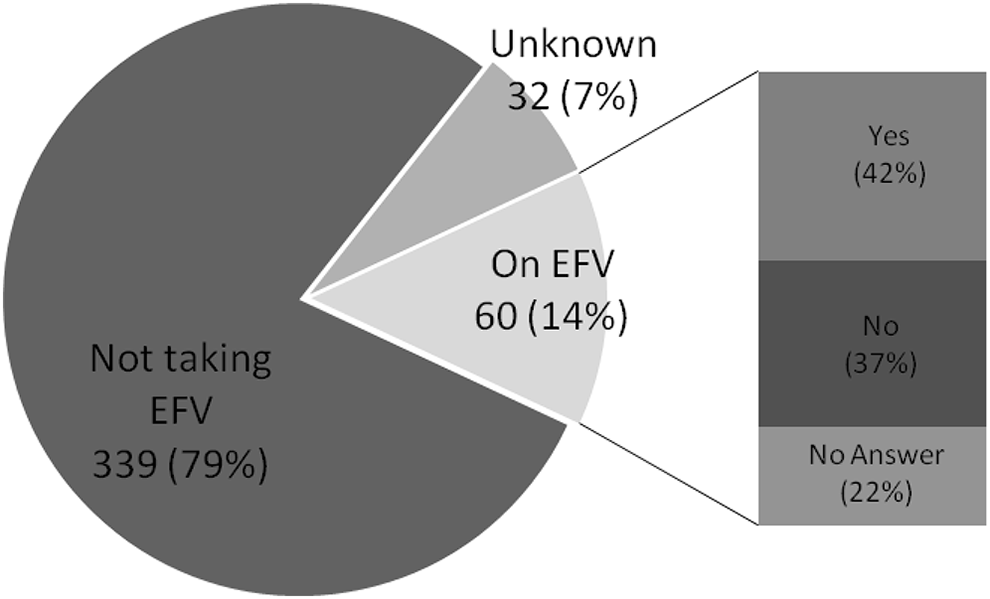
Participant taking efavirenz (EFV) reporting discussions of potential teratogenicity of EFV.
Discussion
Although 73% of the 431 HIV-positive women of reproductive potential in our study indicated that they desired pregnancy, only 51% reported that one of their physicians had discussed pregnancy planning with them. When we assessed the different types of physicians individually, the rates were even lower, 34%, 41%, and 38% for their FP, HIV specialists, and Ob/Gyn, respectively. It was encouraging to note that for women desired or intending to become pregnant in the future, the proportions of those counseled was higher. This may signify that physicians may have some alternate method of knowing when to counsel women of reproductive potential on pregnancy planning; this could be via conversations that the patient does not remember or by type casting younger women in relationship to younger children. Although of less importance, we found that among the 60 taking EFV, 37% reported that none of their medical HCPs had discussed the potential teratogenic effects of the drug if taken during pregnancy. Although this finding is currently less clinically significant, the DHSS still recommends that EFV not be used in preconception or in the first 5 to 6 weeks of pregnancy, and it is therefore important to counsel on this point in the preconception phase. 12
The significant correlates of increased preconception counseling in our multivariable model included younger age, being born outside of Canada and number of years in Canada, being married or in a common law relationship or living with a partner, and having younger children. Other studies 27,31,43 –48 have found the significant correlation between younger age and increased counseling on pregnancy and have argued that it is logical that this association exists. However, although women in their 20s and early 30s are being counseled, women in their midlife (late 30s and early 40s) may still desire to become pregnant and may proceed with pregnancy without counseling and proper preconception care or may not become pregnant at all due to lack of appropriate education. Our study is the first to expand beyond age as the main correlate of HCP communication on pregnancy and HIV. Similar to age, being married or in a common law relationship or living with a partner is an obvious correlate of pregnancy counseling. However, our previous work showed that marital status was not correlated with pregnancy intention and that not counseling single women will miss an important number of women. 5,26,49 Again, limiting counseling to women with younger children is also a missed opportunity for women with older children.
Interestingly, although the proportion of women in our study who reported that they were satisfied with the overall care of their physician was high (94% for any physician), the proportion reporting satisfaction with the amount of pregnancy planning information received was low (63% for any physician), correlating with the relatively low degree of preconception discussion reported. This finding likely reflects the multiple factors that lead to satisfaction with patient–physician relationships.
Freedman recently published an important commentary about the integration of HIV and maternal services. 50 She outlines how the maternal health organizational culture stands in stark contrast to the rapid, well-resourced deployment of HIV services around the world, while significant numbers of maternal and infant deaths continue from intrapartum hemorrhage, hypertension, and treatable conditions. She advocates that integration holds the answer for the much needed transformation of implementation support practices in both the fields. Although integration would solve several problems for women living with HIV of reproductive age, the feasibility of merging these 2 megaoperations seems daunting. Rather, from our work and this analysis, we propose that preconception care become integrated with HIV care, as these skills are easily taught to HIV HCPs. 5,13,18,19,49 –53 The training of HCPs is essential to integrating HIV and preconception care. Studies have shown that HCPs in the field of HIV may not feel comfortable engaging in open dialog with patients regarding protective sexual health behaviors along with the intrapersonal and social factors that affect reproductive decision making. 54,55 As these HCPs need to provide the knowledge of preconception care via training tools, programs, and workshop, they need to be provided with the counseling tools and training required to provide quality preconception counseling and communication of sexual health issues. In Canada, we have begun operationalizing such a program called the Canadian HIV Fertility Program with the first deliverable being the publication of Canadian HIV Pregnancy Planning Guidelines. 17 These evidence- and community-based guidelines are aimed to assist HCPs in addressing the pregnancy and fertility needs of HIV-positive individuals and couples by providing clinical information and flexible recommendations that take into account the social factors and intersecting population needs of individuals living with HIV in Canada. The aim of the Program and Guidelines is to reduce the stigma associated with HIV and pregnancy, increase access to pregnancy planning and fertility services, reduce vertical and horizontal transmission of HIV, and improve fetal and maternal outcomes in the context of HIV. 18
The present study has a number of limitations. (1) Its retrospective nature could have contributed to recall bias when the women were asked to remember whether their physicians had discussed pregnancy planning with them. As providers were not included in this study, it is possible that such discussions about reproductive health did occur and that the women did not recall. There is a significant body of literature on the correlation between the discussions had by physicians and what is recalled and reported by the patients. 56 –61 Furthermore, some would argue that it is what the patient remembers having been discussed which is crucial and that further work is required to determine the optimal methods of communication for patients to take in, consider, and address counseling provided by physicians and other HCPs. (2) Questions regarding OB/Gyns could be biased; women are likely seeing such a specialist either because they are pregnant or because of cervical dysplasia, and the topic of pregnancy planning may not be essential to the primary reason for the visit and appropriately not addressed. (3) The questions were focused only on counseling provided by physicians and not by other HCPs. In many settings, nurses and social workers would provide such counseling. (4) The data were collected 4 years ago and could be argued to not be current. However, it is felt that although there has been much progress in the field of HIV and reproductive health internationally, little has trickled to North America and less at the physician level. (5) Many clinical and demographic questions were reported at the time of the survey and not at the time when the physician had the discussion about pregnancy planning, limiting the analysis of their impact. (6) Exact timing of potentially related variables such as that of preconception counseling, pregnancy, and tubal ligation was not captured. (7) Our questions on preconception counseling were not adapted from validated scales; however, our study is in line with the recent publications on the topic. 27,31,43 –48 (8) Finally, the sample population was limited to adult women ≥18 years of age due to requirement from our REB, which led to exclusion of adolescent girls, an important group to investigate as it relates to reproductive health.
Despite these issues, there are also a number of strengths of our study including its large sample size, which allowed us to include a larger number of correlates of interest in our regression analyses compared to other investigations in this field. 36,62 –69 An attempt was made to match the study recruitment to the geographic distribution of HIV-positive women living in Ontario, allowing for generalizations to the Ontario HIV-positive female population and for more meaningful contributions to provincial policy. 22 A significant proportion of the enrollment was carried out using a community-based research model involving nongovernmental organizations and women living with HIV in the study recruitment and coordination. 5 This had multiple benefits including engaging participants who do not usually partake in research and increasing the capacity of the Ontario HIV-positive community to conduct research. Such recruitment techniques likely contributed to our findings not being inflated compared to if we had sampled only from clinics.
As much of our previous work 5,26,49 in this area has stressed, the findings in this study highlight the importance of developing programs that support fertility and pregnancy planning for HIV-positive individuals. It is evident from our current analysis that our program should include training of physicians and HCPs on items required for the pregnancy planning counseling. Although FPs who specialize in HIV care and HIV specialists may want to counsel on pregnancy planning, many may not have the knowledge regarding preconception care. We hope that our research and ongoing projects assist HIV-positive individuals, policy makers, and HCPs globally to develop their programs for safer, supportive pregnancy and family planning for HIV-positive individuals in their communities.
Footnotes
Authors’ Note
Additional research team members are listed in Acknowledgment section.
Acknowledgments
We thank the study participants, the frontline AIDS Service Organization staff and research coordinators, and the members of the Project Advisory Committee.
The Ontario HIV Fertility Research Team members are Victoria Govan, Women’s College Research Institute, Toronto, Ontario, Canada; Saira Moammed, Women’s College Research Institute, Toronto, Ontario, Canada; Elena Ivanova, Women’s College Research Institute, Toronto, Ontario, Canada; Sylvie Daviau, ACCESS AIDS Network of Sudbury, Sudbury, Ontario, Canada; Lisungu Chieza, Women’s Health in Women’s Hands, Toronto, Ontario, Canada; Anna Laziri, Africans in Partnership Against AIDS, Toronto, Ontario, Canada; Precious Hove, Voices of Positive Women, Toronto, Ontario, Canada; LaVerne Monette (deceased), Ontario Aboriginal HIV/AIDS Strategy, Toronto, Ontario, Canada; James F. Downey, Toronto East General Hospital, Toronto, Ontario, Canada; Anne C. Wagner, Ryerson University, Toronto, Ontario, Canada; Trent Newmeyer, Brock University, Brock University, St Catharines, Ontario, Canada; Lena C. Soje, Black Coalition for AIDS Prevention, Toronto, Ontario, Canada; Marvelous Muchenje, Women’s Health in Women’s Hands, Toronto, Ontario, Canada; Pancha Panzo, AIDS Committee of Toronto, Toronto, Ontario, Canada; Semenawork Tafes Teklemariam, Africans in Partnership Against AIDS, Toronto, Ontario, Canada; Janvere Bessette, Black Coalition for AIDS Prevention, Toronto, Ontario, Canada; John MacTavish, HIV/AIDS Regional Services, Kingston, Ontario, Canada; Jenna Christensen, 2-Spirited People of the 1st Nations, Toronto, Ontario, Canada; Corena Ryan, 2-Spirited People of the 1st Nations, Toronto, Ontario, Canada; Maureen Ringlein, The Teresa Group, Toronto, Ontario, Canada; Edith Reyes, AIDS Committee of Simcoe County, Barrie, Ontario, Canada; Lori Baxter, AIDS Committee of Windsor and AIDS Support Chatham-Kent, St Catherines, Ontario, Canada; Craig Maguire, Access AIDS Network Sault Ste. Marie, Sault Ste. Marie, Ontario, Canada; Jag Parmar, People Living with HIV/AIDS Foundation Toronto, Ontario, Canada; Tiff Idems, AIDS Committee of Durham Region, Oshawa, Ontario, Canada; Julie Henshaw, AIDS Committee of Cambridge, Kitchener, Waterloo and Area, Kitchener, Ontario, Canada; Jackie Barrett-Greene, AIDS Niagara, St Catherines, Ontario, Canada; Alexandra Beasse, AIDS committee of London and AIDS Action Committee of Perth County, London, Ontario, Canada; Shannon Dougherty, AIDS committee of London, London, Ontario, Canada; Rebecca Skibinski, AIDS Network of Hamilton, Hamilton, Ontario, Canada; Bridget Marsden, AIDS Network of Hamilton, Hamilton, Ontario, Canada; Haran Vijayanathan, AIDS Committee of York Region, Newmarket, Ontario, Canada; Roy Male, Centre Francophone de Toronto, Toronto, Ontario, Canada; France Dorian, Centre Francophone de Toronto, Toronto, Ontario, Canada; Rai Reece, Prisoners with AIDS Support Action Network, Toronto, Ontario, Canada; Sandy Garnet, Huron County HIV/AIDS Network, Clinton, Ontario, Canada; Anne-Marie Zajdlik, Masai Centre, Guelph, Ontario, Canada; Corinna Quan, HIV Care Program, Windsor Regional Hospital, Windsor, Ontario, Canada; Haoua Inoua, AIDS Committee of Ottawa, Ottawa, Ontario, Canada; Wendy Wobeser, Department of Medicine, Queen’s University, Kingston, Ontario, Canada; Alan Li, Regent Park Community Health Centre, Toronto, Ontario, Canada; Cheryl Wagner, Private Practice, Toronto, Ontario, Canada; Greg Gamble, AIDS Thunder Bay, Thunder Bay, Ontario, Canada; Suzanne Paddock, Toronto People With AIDS Foundation, Toronto, Ontario, Canada; Gord Arbess, Department of Family & Community Medicine, St Michael’s Hospital Toronto, Ontario, Canada; DeSheng Su, University Health Network, Toronto, Ontario, Canada; Michael S. Silverman, Lakeridge Health Centre, Oshawa, Ontario, Canada; Kevin Gough, Department of Medicine, St Michael’s Hospital, University of Toronto, Toronto, Ontario, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by peer-reviewed grants from the Canadian Foundation for AIDS Research (Grant# 018-033) and the Ontario Ministry of Health and Long-term Care, AIDS Bureau. Five investigators are also the recipients of salary support from the Canadian Institutes of Health Research (CIHR; MRL) and the Ontario HIV Treatment Network (TAH, SLW, JBA, JMR). Seven authors are investigators of the CIHR Canadian HIV Trials Network (CTN; MRL, TAH, SLW, FS, AR, JBA, JMR) and one is a CTN Community Advisory Committee member (SM). The CTN provided funds for the translation of the questionnaire.