
Abstract
Individuals testing HIV positive were interviewed at testing centers, followed prospectively and interviewed again when they registered at referral antiretroviral therapy (ART) centers (ARTCs). Those who did not register at ARTCs were traced and interviewed in the community. A total of 1057 newly diagnosed people living with HIV (PLHIV; 52% women; mean age, 34.7 years) were recruited. A total of 73.5% of PLHIV registered at referral ARTCs within 60 days, 17.9% did not register and were interviewed in the community, and 8.6% were not interviewed. The 2 main reasons cited for not registering were a perception of good health (30%) and work/family engagements (22%). Single clients (adjusted relative risk [ARR]: 1.54; 95% confidence interval [CI]: 1.02-2.34), participants who had not disclosed their HIV status (ARR: 2.32; 95%CI: 1.77-3.05), participants who knew a PLHIV (ARR: 1.89; 95% CI: 1.41-2.53), and participants from laborer households (ARR: 2.66; 95%CI:1.15-6.15) were more likely to not register. In conclusion, the majority of newly diagnosed PLHIV do reach ARTCs. Disclosure concerns and a perception of good health prevent PLHIV from accessing services.
Introduction
The effectiveness of antiretroviral therapy (ART) for the treatment of HIV infection and resultant reduction in morbidity and mortality is firmly established. 1,2 With the recent scale-up of services, ART has been made available through public health services in many developing countries. Despite this, many people living with HIV (PLHIV) do not receive treatment. It is estimated that only 36% of the 15 million people in need in low- and middle-income countries were receiving treatment at the end of 2009. 3
Care for HIV infection follows a cascade where each step is dependent on successful completion of the previous one. Thus, newly diagnosed HIV-positive people need to reach an ART center (ARTC). Once there, eligibility for ART is ascertained through a clinical assessment and CD4 test. Thereafter, those eligible for treatment need to initiate ART and those not eligible need to remain engaged in care for regular follow-up. Linkage, engagement, and retention in care are essential for optimal individual and community level outcomes. 4 Pretreatment loss-to-follow-up (LTFU) after HIV diagnosis varies from 45% to 47% in South Africa and 36% to 55% in Kenya; a US Centers for Disease Control and Prevention study from 18 states in the United States found that 28% of HIV-infected persons had delayed entry into care. 4 –9 Studies have shown that stigma, transportation difficulties, poor geographical access, and supplementary costs are important factors that prevent clients from accessing treatment even when it is provided free of cost. 10 –13
The National AIDS Control Organization (NACO) estimates that India has 2.3 million PLHIV. 14 In 2004, the Government of India initiated a national program to provide free ART for PLHIV. By the end of March 2009, there were 2487 integrated counseling testing centers (ICTCs) across India and 211 ARTCs; yet, only 320 074 PLHIV (cumulative) of the estimated 790 000 eligible for ART as per the World Health Organization 2006 treatment guidelines were receiving treatment by December 2009. 3 Increasing enrollment to reach all those who are eligible has been a challenge. 15 Each year a number of people test positive, but how many of them reach an ARTC to register and be assessed for ART eligibility, and the reasons for not registering at ARTCs, are not known.
Most of the existing evidence on barriers faced by clients in accessing ART services in India are drawn from the studies based on PLHIV who are accessing services—adherence to treatment or operational issues with ART service delivery and client access. 16 –22 A study exploring factors influencing treatment initiation among PLHIV found the lack of awareness of ART and eligibility criteria, financial difficulties, and deferral by physicians to be important barriers. 23 Another study highlighted the role stigma and disclosure concerns play in limiting the uptake of ART. 24
In this article, we present findings from a prospective cohort study conducted among newly diagnosed HIV-positive persons recruited from ICTCs across 6 Indian states to examine the enrollment into ART services and explore barriers to enrollment among those who do not register at ARTC.
Methods
A prospective cohort study was conducted. Over a 4-month recruitment period all newly diagnosed HIV-positive persons from participating ICTCs were invited to participate in the study after completing their posttest counseling. In addition to routine posttest counseling, the counselors informed HIV-positive persons about the 2 surveys (at the ICTC and ARTC), the need for detailed contact information, and willingness to be contacted in the community. Willing participants responded to a survey conducted onsite at the ICTC and were provided a referral slip for the ARTC. Refusals were noted. Data were collected on sociodemographic background, reasons for seeking HIV testing, family support, understanding of HIV infection and treatment available, and their experience of HIV pre- and posttest counseling. A second follow-up interview was conducted with the participants when they registered at the referral ARTC. Clients who did not register at the referral ARTC within 60 days were contacted in the community with the help of counselors and outreach workers linked to the ICTC and interviewed at a place of their choice: at the ARTC, ICTC, a non-governmental organization or at home. The follow-up interview focused on reasons for not registering at the ARTCs and treatment or other services obtained from other providers. All participants interviewed in the community were counseled to register at the ARTC and linked to community outreach workers as needed. Face-to-face interviews were conducted by trained staff after obtaining written informed consent from each participant. The inclusion criteria were ≥18 years of age; HIV-positive test result; willingness to participate, to provide contact information, and to be contacted in the community; and residence at the same address for the past 6 months and following 3 months (nonmigrant). The study was approved by the Population Council’s institutional review board in New York and NACO’s ethical review committee.
Site Selection
In consultation with NACO, 2 districts were selected in each of the high-HIV prevalence states of Maharashtra, Karnataka, and Andhra Pradesh and 1 district each in the low-HIV prevalence states of Uttar Pradesh (UP), Rajasthan, and Gujarat. In each district, 1 high-volume ARTC, that is, with >1000 HIV-positive clients receiving ART and a monthly accrual rate of at least 30 new registrations, was selected. Further, 3 high-volume ICTCs that referred clients to each of these ARTCs were selected. In the high HIV-prevalence states, every district has an ARTC that caters to ICTCs located within the same district; whereas in low-HIV prevalence states, as there are fewer ARTCs, each center serves clients referred from ICTCs from the same and other districts. Thus, selected ICTCs were located outside the district in the low-HIV prevalence states and within the same district in the high-HIV prevalence states. A total of 27 ICTCs and 9 ARTCs participated in the cohort study.
Stata 10.0 (Stata Corporation, College Station, Texas USA) was used for data analysis. Bivariate analysis using chi-square tests for categorical variables and Student t test for continuous variables were conducted to determine differences between the groups. Bivariate and multivariate modified Poisson regression with robust variance estimates were used to determine the relative risk (RR) estimates for the independent predictors of nonregistration at a referral ARTC within 60 days. Logistic regression was not performed as odds ratios (ORs) can overestimate the association between an independent variable and dependent variable if the outcome of interest is common (greater than 10%) as there is an increasing difference between the RR and OR with increasing occurrence of the outcome. 25,26 We used a fully loaded model to minimize the bias in our estimates. Open-ended responses were recorded for reasons provided for nonregistration at referral ARTCs; these were analyzed qualitatively.
Results
Recruitment and Retention of Cohort
Between September 2009 and January 2010, a total of 1600 people tested HIV positive at the 27 participating ICTCs and of those 1057 people were recruited into the cohort (Figure 1). Of these, 777 participants registered at ARTCs within 60 days and were interviewed at their respective ARTCs, while 189 of 280 who did not register were traced and interviewed in the community. Figure 1 provides details for the 91 participants who were not interviewed (32 died within 2 months of their HIV test, 28 were accounted for, and 31 were untraceable).

Recruitment and retention of study cohort.
The sociodemographic characteristics of the HIV-positive participants recruited into the cohort by state are shown in Table 1; variations were noted across the states. Overall, male participants were older (mean, 36 years; standard deviation [SD], 8.9 vs 33.4 years; SD, 8.7; P < .001) and more likely to be currently married (80% vs 51.5%; P < .001) than female participants. More female participants were widowed (34.8% vs 7.6%; P < .001) and more female participants reported the death of a spouse due to HIV (64.6% vs 30.8%; P < .001) than male participants. A total of 12 pregnant female participants were tested at baseline and were linked to the prevention of parent to child transmission program. Overall, men were more likely to report employment than women (87.3% vs 70.9%; P < .001). The majority of employed participants were agricultural or manual laborers.
Sociodemographic Profile of 1057 Newly Diagnosed HIV-Positive Persons Recruited from 27 ICTCs across 9 Districts in 6 Indian States (2009-2010).

Abbreviations: ARTC, antiretroviral therapy center; ICTC, integrated counseling testing center; IQR, interquartile range.
a Of those employed.
b Denominators vary because of missing information.
Participants Registered at ARTC
In all, 777 participants were interviewed at referral ARTCs within 60 days of their posttest counseling after a median of 7 days (interquartile range, 3-18); this included 9 of the 12 HIV-positive pregnant women. More than half (59.8%) of the participants registered at the ARTC within 7 days of collecting the test result, 29.9% by 30 days, and 10.3% after 30 days. The highest registration was observed in Gujarat and the lowest in Rajasthan (Table 1).
Results for CD4 cell counts assessing eligibility for ART were available for 730 of the registered participants. Overall, 55.2% (403 of 730) of the participants had CD4 counts <250 cells/mm3 making them eligible to start ART immediately. A higher proportion of participants in the low HIV-prevalence states of UP (61%), Rajasthan (68%), and Gujarat (63%) had <250 cells/mm3, compared with 58% of the participants in Maharashtra, 55% in Karnataka, and 47% in Andhra Pradesh. CD4 cell counts were not available for participants interviewed in the community.
Participants Interviewed in the Community
The 189 participants who did not register at the referral ARTC within 60 days were traced and interviewed in the community. Most participants had been informed about the availability of free ART and had been provided referral slips at the ICTC (Table 2). The national program recommends linking newly diagnosed HIV-positive persons with members of the positive network for support; only 17% of the participants interviewed in the community had received this assistance.
A small proportion of the participants had consulted other physicians and undergone a CD4 test privately; 18 had registered for ART at nonreferral ARTCs. The majority (90.4%, n = 171) of the participants had not registered for any HIV treatment services. The most frequently cited reason was that participants were in good health and did not feel the need to start treatment (29.8%, 51 of 171) as told by this 31-year-old married female:
I do not have any health problem now—I am fine so why should I go for ART treatment? And my husband is also opposed to me going to the ARTC.
Health Services Accessed by the 189 Participants Interviewed in the Community.
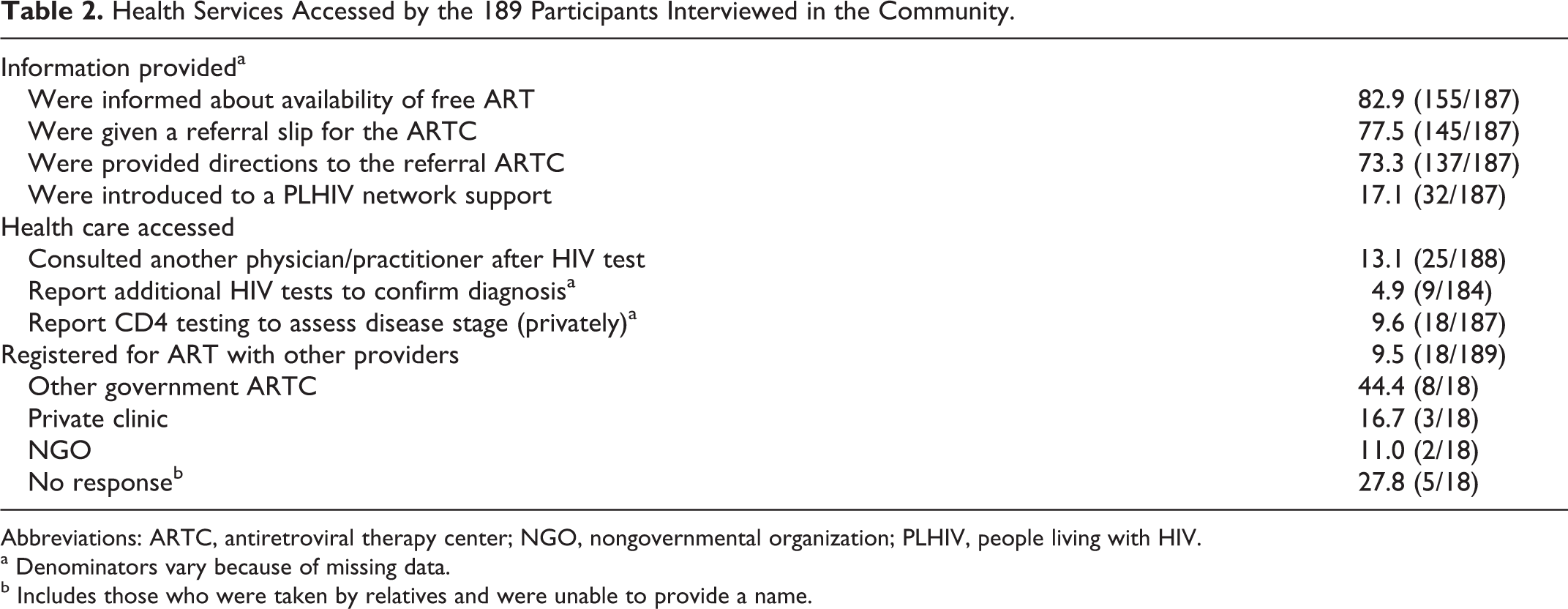
Abbreviations: ARTC, antiretroviral therapy center; NGO, nongovernmental organization; PLHIV, people living with HIV.
a Denominators vary because of missing data.
b Includes those who were taken by relatives and were unable to provide a name.
Several participants (22%, 38 of 171) told the researchers that they were occupied with work or family responsibilities; work often overlapped with financial concerns (8.8%, 15 of 171) as illustrated in the following quote from a 25-year-old male manual laborer:
I have to do agriculture work, I do coconut business, and this is its season. So I did not go as I was busy. I cannot go leaving two children outside. We need to earn when we have work. We are daily wage labour if we do not earn it is difficult to survive.
Other participants (8.8%, 15 of 171) cited fear of disclosure of their HIV status in their communities as the main reason for not seeking treatment, as illustrated by this 45-year-old man from Karnataka:
… I did not visit ART centre for taking treatment because (in that centre) my relative is working … I did not disclose my status to anybody; it is a matter of prestige. If they come to know about this then they will disclose my status to all my relatives then it will create a problem for the family.
While treatment is provided free of cost at government ARTCs, the cost of travel was burdensome for some participants (3.5%, 6 of 171).
I do not have money to travel to this district hospital. We are poor, I am widowed and not doing any work; there is no income for my family. I have two children. I am struggling to feed my family daily. (Narrated by a 35-year-old woman.)
Other participants (4.7%, 8 of 171) felt that ARTCs were too far; logistical difficulties in reaching centers especially for sick participants were mentioned, as by this 55-year-old man:
I am becoming very weak. I do not have the capacity to go to ART centre by bus … I have been admitted in government hospital here.
Some participants preferred to consult traditional healers and priests (2.3%, 4 of 171), as this 28-year-old woman stated,
I will take ayurvedic medicine for 6 months, if I am not recovering, then I will take the ART medicine.
While another 43-year-old woman explained:
I believe in God. I do not want to go to ART centre. Without treatment my HIV status will cure. The pujari (priest) of temple (Priest in a Hindu’s place of worship) has told me to fast for 21 days then it will cure.
Around 4 (2.3%) participants could not register at the ARTC because of a strike by health workers at ICTCs and ARTCs in 1 state. Participants also reported other barriers, such as family objection (5.3%, 9 of 171), ill-health, and not having “proof of residence” documents (ration or election ID cards) for registration purposes (2.3%, 4 of 171). A 40-year-old female participant lamented:
When I received my test report the counsellor told me to go to ART centre with HIV report and also election ID card or ration card. But I do not have these cards … that is why I did not visit the ARTC.
Some participants (2.9%; 5 of 171) reported that they had been asked by physicians to first complete their tuberculosis (TB) treatment prior to registering at the ARTC. In all, 2 (1.2%) participants felt strained by the number of visits required to receive their HIV test result and referral to the ARTC.
ICTC counsellor did not give me the HIV report and so I visited the ICTC many times … I have no energy. I do not know the city. I do not know how many times I (will need to) visit the ART centre. I (am) scared with no one ready to come with me. 37-year-old man.
A few participants (3.5%; 6 of 171) were not convinced that they were HIV positive and wanted to confirm the result by testing again; some of those wanted to repeat the HIV test at a private laboratory for better quality of testing. A 25-year-old woman reported:
I do not believe this ICTC result and I did not tell my husband about my status. I will not take treatment in government hospital; I will go to a private hospital for another HIV test … I think private treatment is good.
In all, 8 (4.7%) participants did not provide any reasons.
Factors Associated with Nonregistration at ARTC
On bivariate analysis, single or illiterate participants, those with a household income of less than Rs 1500/month, those belonging to a household where the principal occupation was manual labor, participants who had not disclosed their HIV-positive status to anyone, those who knew another HIV-positive person in the community and participants from Karnataka were more likely to not register at the referral ARTC (Table 3). Age >36 years had a protective effect. Number of HIV tests taken, receipt of referral slip, satisfaction with counseling services at the ICTC, and having a family member receiving ART were not associated with nonregistration at an ARTC (data not shown).
Factors Related to Nonregistration at Referral ARTCs Within 60 Days of Posttest Counseling among 948 Newly Diagnosed HIV-Positive Participants (ARTC: 777; Community: 171a).
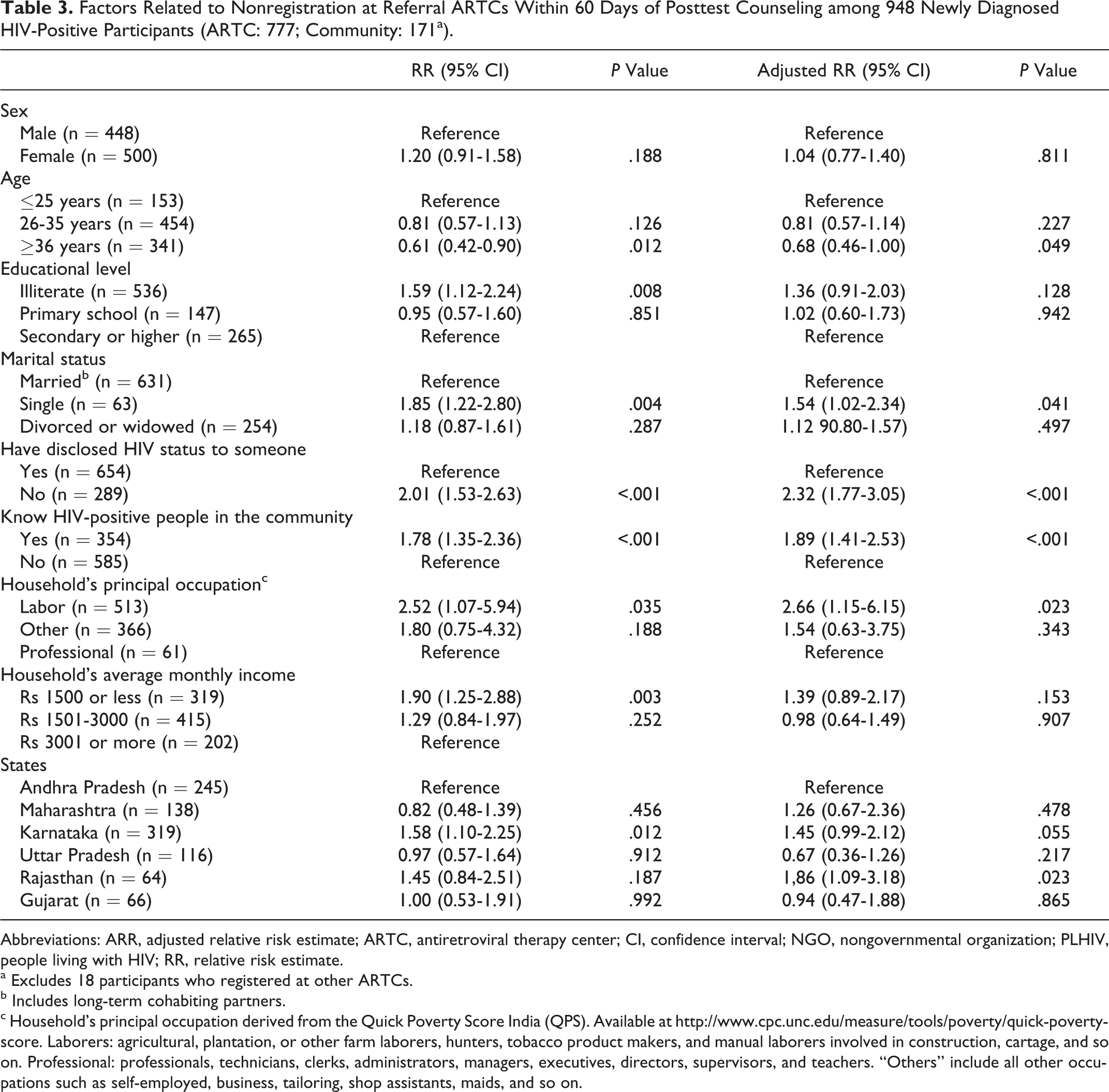
Abbreviations: ARR, adjusted relative risk estimate; ARTC, antiretroviral therapy center; CI, confidence interval; NGO, nongovernmental organization; PLHIV, people living with HIV; RR, relative risk estimate.
a Excludes 18 participants who registered at other ARTCs.
b Includes long-term cohabiting partners.
c Household’s principal occupation derived from the Quick Poverty Score India (QPS). Available at http://www.cpc.unc.edu/measure/tools/poverty/quick-poverty-score. Laborers: agricultural, plantation, or other farm laborers, hunters, tobacco product makers, and manual laborers involved in construction, cartage, and so on. Professional: professionals, technicians, clerks, administrators, managers, executives, directors, supervisors, and teachers. “Others” include all other occupations such as self-employed, business, tailoring, shop assistants, maids, and so on.
On multivariate analysis, being single, belonging to a household with a principal occupation of manual labor, nondisclosure of HIV status, personally knowing another HIV-positive person in the community, and receiving care in Karnataka or Rajasthan were independent risk factors for nonregistration at referral ARTCs (Table 3). Older participants (>36 years) were at lower risk for nonregistration.
Discussion
This is the first multisite study in India to follow a cohort of newly diagnosed HIV-positive persons to determine the proportion of clients accessing care and treatment services. Almost three-fourths (73.5%) of the newly diagnosed HIV-positive participants registered at referral ARTCs and were evaluated for ART eligibility within 2 months of collecting their HIV-test result. The pretreatment LTFU was much lower than the 45% to 47% reported by Losina et al 6 and Scott et al 8 from South Africa and 36% to 55% reported by Hassan et al 5 and Zachariah et al 9 from Kenya. Two-thirds of the 280 nonregistered participants were successfully traced and interviewed in the community providing important insights into reasons for nonregistration; a further 21% were accounted for but not interviewed, and only 11% were untraced.
The majority of the HIV-positive participants who did not register at ARTCs were not accessing ART nor had been assessed for treatment eligibility placing them at risk of delayed treatment. A very small number of HIV-positive clients had registered at government ARTCs in other districts for reasons of confidentiality or travel constraints. Further, just a handful of participants accessed private health providers, suggesting that the public sector is still the main provider of services for this population.
Reasons for nonregistration varied. A perception of relatively good health removed the urgency to register immediately for many, while work and family engagements kept others away. The fear of disclosure of their HIV status, being recognized by villagers or relatives, and the resulting stigma was the overriding concern for many others; this has been found in other countries 11 –13 and in India. 24 Results from the multivariate analysis show that participants who had not disclosed their status to anyone or those who knew HIV-positive persons were less likely to access care; this provides additional support to the issue of stigma. Although ART is offered free at government centers, financial difficulties and travel-related expenses were deterrents for some participants; this has also been reported by other studies in India and Africa. 6,15,16,23 For participants earning their livelihood through daily wage labor where a day off results in lost wages further highlights the challenge these people face. Traveling distances to reach ART centers proved onerous for participants with advanced disease and poor health, limiting access for participants who probably needed ART most. 6 Losina et al reported a distance of more than 10 km to the ARTC as a key factor contributing to pretreatment LTFU in their study. In a few cases, participants waited to complete TB treatment prior to registering at ARTCs 6 ; Losina et al report this as an important factor delaying access. We observed differential registration between the states. On multivariate analysis, participants from Rajasthan and Karnataka were found to be at a higher risk for nonregistration. In Rajasthan the 3 ICTCs (Ajmer, Alwar, and Sikar) were located at a distance from the ARTC in Jaipur (average around 130 km). In Karnataka, 75% of the participants were illiterate and 55% were women. Older participants in our study were less likely to delay registration; it is possible that older clients take their infection more seriously and access care quickly. However, 3 studies exploring pretreatment LTFU did not find age to be related. 5,6,9
This study provides important insights on barriers to uptake of ART services. The study was conducted in high- and low-HIV prevalence states of India and although there are interstate differences in the characteristics of the HIV-infected population, we feel the findings can be generalized to other ARTCs and states in the country. The counselors at ICTCs and health workers at TB and antenatal clinics and medical/pediatric wards where clients are routinely sent for HIV testing should be made aware of these factors and trained to identify at-risk clients and initiate a closer follow-up through community outreach. It is of concern that 32 newly diagnosed HIV-positive people had died within 2 months of their HIV test. These participants, with presumably advanced HIV disease, did not receive the benefit of the free ART program.
Intensive counseling and support to address and facilitate disclosure of HIV status and manage fears related to loss of confidentiality are needed. Simplifying registration procedures and reducing the need for multiple visits are important. A provision for HIV-positive participants to be offered a choice of government ARTCs, especially in states where a wider network of ARTCs exists, could be considered. Giving people a choice would go a long way in addressing some of the confidentiality issues confronting newly diagnosed HIV-positive people. Accelerating the expansion of the network of ART service delivery through the opening of link/satellite ARTCs would serve to reduce travel and related costs. 14 Best practices that could be emulated include the provision of travel concessions on public transport for PLHIV as is being provided in Rajasthan; and the informal arrangement of transport services (hospital ambulance) from ICTCs to referral ARTC on a fixed monthly schedule being done in Mahesana, Gujarat. Finally, benefits of engaging PLHIV support groups have not been fully utilized. In UP, members of the positive network were actively engaged in advising and accompanying PLHIV to the ARTC in Varanasi; this practice could be replicated in other states.
The study is not without limitations. We did not follow participants beyond the initial registration process, and thus we are not able to provide information on retention after registration. The study would have benefited from CD4 counts for participants interviewed in the community to assess what proportion of those in need of ART did not register. A total of 191 newly diagnosed HIV-positive persons refused to participate in the study which could potentially bias the results because of systemic differences between those who agreed and those who refused to participate. Unfortunately, because of lack of consent, we were unable to collect and analyze their sociodemographic information from the ICTC registers. As we included only high-volume ICTCs in our study, it is possible that the heavy workload for counselors could have influenced the quality of counseling offered and therefore the registration at ARTCs; the experience could be different at low-volume ICTCs.
In conclusion, the majority of newly diagnosed HIV-positive people do present themselves and register at ART centers. Although barriers that deter HIV-positive people from accessing treatment services do exist, they are not insurmountable. Addressing client and health system barriers would serve to increase uptake of services.
Footnotes
Acknowledgments
We would like to thank Dr K. Chandramouly, ex-Secretary, Department of AIDS Control and Director General, NACO, for his support. We would like to extend our thanks to the District Nodal Officers, Medical Officers in-charge, and counsellors at all participating ARTCs and ICTCs. Finally, we would like to thank all the participants for their contribution and time.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the National AIDS Control Organisation, Ministry of Health and Family Welfare, Government of India.