
Abstract
Introduction
HIV/AIDS, with which 36.7 million people were living and 2.1 million newly infected at the end of 2016, has been one of the major health problems globally. From the beginning of the epidemic to 2016, 35 million people died from AIDS-related illnesses. 1 Although the burden of HIV continues to vary significantly across countries, Sub-Saharan Africa remains the most affected with almost 1 in every 25 adults (4.4%) living with it, accounting for nearly 70% of the global burden. 2
According to the 2014 estimate the national HIV prevalence in Ethiopia was 1.14%, and the number of people living with HIV is 769, 600 with 15, 700 new HIV infections and 35, 600 AIDS-related deaths each year. 3 Adherence is defined as a patient's ability to follow a treatment plan, take medications at prescribed times and frequencies, and follow restrictions regarding food and other medications. To achieve optimal results from ART, high levels of patient adherence to ART is essential. High levels of adherence to ART (at least 95%) is needed to ensure optimal benefits. 4
The Human Immunodeficiency Virus (HIV) infection does not only upset the health of individuals but also impacts on households, communities, and the development of nations. When countries are affected by HIV, they also suffer from other infectious diseases, food insecurity, and other serious problems. 5 Antiretroviral therapy has an impressive clinical effect in that it decreases the viral replication and viral load which in turn preserves the CD4 level, decreases the progress of AIDS, and reduces AIDS-related deaths. 6
Concerns about adherence and subsequent development of drug resistance, poor infrastructure, logistic and human capacity, and cost-effectiveness were the major issues. 7 The most frequently economic-related, therapy-related and behavioral related factors were identified as a factor related to non-adherence. In addition to this relationship and psychological related factors were identified as barriers to good adherence.8, 9
Non-adherence has been measured as the most public reason for treatment failure, which resulted in a potential risk of drug resistance development through suboptimal viral suppression 10, 11 Considering the Ethiopian government's commitment toward ending HIV by 2030, achieving the required level of suppressed viral load is more challenging compared to the increasing number of People Living with HIV that knew their status and an increasing number on treatment were 32%, 79%, and 65% respectively. Although, a low level of adherence that is below 95% has been reported in sub-Saharan Africa including Ethiopia suggesting the need to identify determinants of adherence to Antiretroviral therapy as paramount. 12
Therefore, this study aimed to assess magnitude of adherence to antiretroviral treatment and associated factors among seropositive people received treatment in Jimma town public health facilities,
Methodology
Study Design and Setting
A facility-based cross-sectional study design was employed in Jimma town public health facilities from March to April 2019. Jimma town is one of Oromia Regional State which is located 352 km southwest from the capital city of Ethiopia, Addis Ababa. Jimma town has two public hospitals (JUMC and Shanen gibe general hospitals), three private hospitals (Oda hullee, Hawetu and Firomsis hospitals), four health centers (Mandara kochi H/c, Jimma H/c, Bacho bore H/c and Higher 2o H/c) and two non-governmental health facilities (FGAE and Meri stope). The study focused on the four public health facilities (two hospitals and two health centers) which are providing antiretroviral treatment services for people living with HIV/AIDS (PLWHA).
Study Population
The study population was all systematically selected adult PLHIV who are on Antiretroviral therapy with the age of 18 years and above and duration on Antiretroviral therapy six months and above were included in the study. Those participants are seriously ill or unable to communicate during the study period were excluded from the study.
Sample Size and Sampling Procedure
The sample size was determined using single population proportion formula (n = (Z α/2)2 P (1-P)/d²) by considering the assumption of the prevalence of adherence to ART among adult PLWHA with unable to get quality of food in the study conducted in hospitals found in Tigray Regional State Northern Ethiopia was 46%, 13 95% confidence level, and 0.05 margin of error, 10% non-response rate. Calculated by the mentioned assumptions, the sample size was adjusted by correction formula due to the source population which was the total admitted patients (4232) in the study facilities were less than ten thousand, so the final sample size was 385.
The study participants were selected four Antiretroviral Therapy providing Jimma town public health facilities like Jimma medical center hospital, Shenen Gibe district Hospital, Jimma health center, and Higher two Health Center using a systematic sampling technique. The samples were drawn proportionally from each facility based on the number of seropositive peoples who received treatment.

Schematic presentation of the sampling proportion of the adherence to antiretroviral treatment among seropositive peoples on the treatment in Jimma town public health facilities, 2019.
Data Collection Tools and Method
Questionnaires were developed after reviewing different kinds of literature. A structured interviewer-administered questionnaire was used to collect data. Some changes were made to the questionnaire after the pretest result. The tools were clear and suitable for the participants, with modifications made to improve the clarity, sequence, consistency, and structure of the questionnaire. The content validity of the tool was checked by two experts and the reliability of the tools was checked by Cronbach's alpha after the pretested result.
Data were collected by five BSc nurses and supervised by two MSc nurses after two days of training. The questionnaire was translated into local languages and then retranslated back to English to maintain consistency by language experts of both languages. The data collectors completed the questionnaire for each respondent and it took about 20 min to complete the questionnaire. Participants were interviewed in a separate quite room to maintain confidentiality. Finally, the completed questionnaires were checked by supervisors.
Data Analysis
Data were cleaned and entered into Epi Data version 4.1 and exported to SPSS version 20 for descriptive and inferential analysis. Bivariate logistic regression analysis was done and variables with a p-value of <0.25 were included in multivariable logistic regression analysis. Variables with a p-value of <0.05 in the final regression were considered as statistically significant associated with the outcome variables.
Data Quality Management
To ensure the quality of data, a questionnaire was translated to the local language, training was given for data collectors and supervisor, a pre-test was done on 19 (5%) of the total sample size in Yabu health center and a necessary adjustment was made before used for actual data collection.
Variables of the Study
Dependent variable: Adherence to ART
Independent Variables
Socio-demographic variables, food security status, treatment related factors, client and social related factors, health facility and health care provider related factors.
Operational Definition
Adherence to ART
Ethics Approval and Consent to Participate
Ethical approval was obtained from Jimma University, Institute of Health, Institutional Review Board (IHRPGD/64/2019). A permission letter was obtained from the Jimma Zonal and district health office then offered to hospitals and health centers. Since the authors thought that there was no any potential risk associated on the provision of the data and it is a cross-sectional study, informed verbal consent was considered and obtained from each respondent before study. Participants were informed about their rights to decline if they didn’t want to continue. The questions were coded instead of using names, confidentiality was assured throughout the study. Involving the use of any animal or human data or tissue: “Not applicable” in this research section. Data from any individual person in any form (including individual details, images or videos): “Not applicable” in this research.
Results
Socio-Demographic Characteristics
The study was conducted on 385 study participants and the response rate was 100%. The mean age of participants was 37.61 (SD ± 8.71) years. Among the participants, 269 (69.9%) were females. The majority of the participants were Orthodox 318 (82.6%) followed by Muslim 132 (34.3%) in religion (Table 1).
Socio-demographic Characteristics of the Adherence to Antiretroviral Treatment Among Seropositive Peoples on the Treatment in Jimma Town Public Health Facilities, 2019. (N = 385)

Clinical and Behavioral status of Seropositive Peoples
This study showed 228 (59.2%) of respondents were having food insecurity. The majority of participants 238 (62.1%) did not use substances use. Among those 173(45.2%) were adhered to ART treatment. Out of the total participants, 68 (17.7%) were used other medication other than ART. Among those (6.8%) were used for the anti-hypertension medication. The majority of participants 344 (89.4%) have a good relationship with ART providers. More than half (56.1%) participants did not follow up their ART appointment regularly (Table 2).
Clinical and behavioral status of seropositive peoples on the treatment in Jimma public health facilities, 2019. (N = 385).

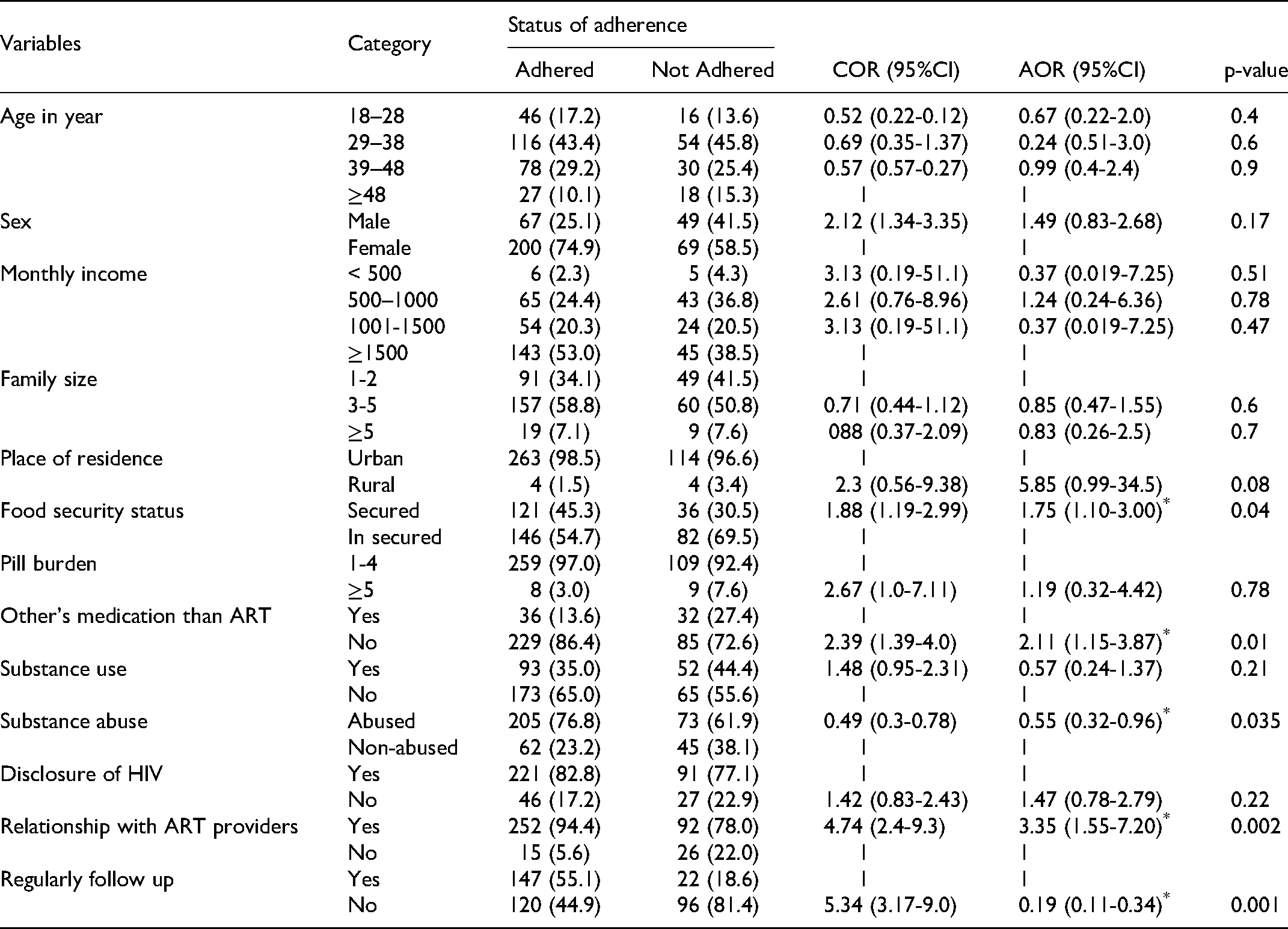
Factors Associated with Adherence to ART Treatment
Food insecure individuals were 1.75 times more likely to be ART to have non-adherence than those who were food secure (AOR = 1.75 (95%CI; (1.01-3.0), P = 0.04. Individuals who reported substance abuse were 45% less likely to be adherent than those who did not report substance abuse (AOR = 0.55(95% CI ;(0.32-0.96), P = 0.035.
Individuals who took other medications due to comorbidity were 2.11 times more likely to have non-adherence than those who did not use other medications (AOR = 2.11 (95%CI; (1.15-3.87), P = 0.01. Individuals who had no good relationship with ART provider were 3.35 times more likely to have poor ART adherence than those individuals who had good relation relationship (AOR = 3.35(95% CI;(3.17-9.0), P = 0.002.
Individuals who did not follow up appointment regularly were 81% less likely to be ART adherence than those individuals who followed their appointment regularly (AOR = 0.19 (95%CI; (0.11-0.34), P < 0.001 (Table 3).
Factors associated with adherence among seropositive peoples on the treatment in Jimma public health facilities, 2019. (N = 385).
Discussion
This study revealed that the magnitude of adherence to antiretroviral treatment was 69.4%. This result is inconsistent with findings of studies done in Nekemte 77.9% , 15 in Dessie 90% 16 in Arba Minch government hospital 77.10% , 17 in Gondar Referral Hospital 88.2% , 18 in Goba Hospital 90.8% adherence. 19 The possible explanation for the difference might be due to the socio-demographic, commitment of health care providers, accessibility of ART medication, and intervention-related factors.
This study revealed that participants who were Food in secured individuals were 1.75 times more likely to be ART to have non-adherence than those who were food-secure (AOR = 1.75 (95%CI; 1.01-3.00). This result is in line with studies conducted in Uganda where food insecurity was associated with ART non-adherence (AOR = 1.95; (95% CI; 1.65- 2.29). 20
This study revealed that participants who used substance abuse were 45% less likely to be ART adherent than those who did not report substance abuse (AOR = 0.55(95% CI; 0.32-0.96). This result is inconsistent with a study done in Areka town, southern Ethiopia reported an association of substance abuse and adherence (AOR = 2.360, (95%CI; 4.347-17.915). 21 The possible explanation for the difference might be due to the study area, availability types of substance abuse, cultural and socio-economic factors.
This study revealed that participants who took other medications due to co-morbidity were 2.11 times more likely to have poor medication adherence than those who did not use other medications (AOR = 2.11; (95%CI; 1.15-3.87). This result is in line with studies conducted in South Africa on observed co-treatment of HIV and other infections as one of the factors associated with adherence to ART. 22
This study revealed that patients who had no good relationship with ART providers were 3.35 times more likely to have poor medication adherence than those individuals who had a good relationship with ART providers (AOR = 3.35; (95% CI; 3.17-9.00). This result is in line with the study conducted in SSA showed that having a good relationship with a health provider was identified as one of the most frequently identified facilitators based on patient-reported barriers and facilitators to antiretroviral treatment (ART) adherence. 8
This study revealed that participants who did not follow their ART appointment regularly were 81% less likely to be ART adherence than those individuals who followed their appointment regularly (AOR = 0.19, (95%CI; 0.11-0.34). This result is inconsistent with the study done in SSA countries for missing scheduled clinic visits (OR = 2.77; (95%CI; 1.73-4.43). 23 The possible explanation for the difference might be due to the study area, being busy with other activities, forgetfulness, cultural and socio-economic factors.
Conclusion
The rate of adherence to antiretroviral therapy was low (69.4%) as compared to the World Health Organization standard ≥ 95%. Food insecurity status, substance abuse, comorbidities, patient's relationship with an ART service provider, and regular follow-up of appointment were associated factors of adherence to antiretroviral treatment among seropositive peoples who received treatment. Therefore, it is recommended that patients, health workers, adherence supporters, and case managers improve Antiretroviral Treatment adherence.
Strength and Limitation of the Study
The large sample size and study focused on all Jimma town public health facilities which are providing antiretroviral treatment services for people living with HIV/AIDS (PLWHA) were indicated as strength. Since the study was conducted at a single town public health facility, the results cannot be generalized to seropositive people received treatment in Ethiopia. Causality cannot be confirmed since the study design is cross-sectional.
Footnotes
Acknowledgments
We would like to thank Jimma University for financial support for the realization of this finding. We are also grateful to Jimma Zonal and the district health office for the provision of the needed data for our study. Special thanks and appreciation go to our respondents, the health facility manager and staff, data collectors, and supervisors.
Abbreviations
Author’s Contribution
ZD, AG, and AK participated in proposal writing, designed the study, coordinated and supervised data collection, data analysis, and supervised data entry. AK and LA wrote the draft manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials
All data apply to this study are available from the corresponding authors.
Consent for Publication
Not applicable
Competing Interests
This manuscript maintains no competing financial interest declaration from any person or organization, or non-financial competing interests such as political, personal, religious, ideological, academic, intellectual, commercial or any others.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.