
Abstract
In South Africa, 62% of female sex workers (FSW) are estimated to be living with HIV. Qualitative research indicates that FSW share antiretroviral therapy (ART) with peers to surmount treatment barriers. We quantitatively described ART sharing, its correlates, and its relationship with viral suppression (VS) among FSW living with HIV in eThekwini, South Africa. Among FSW on ART (n = 890), 30% ever shared (gave and/or received) ART. Sharing ART was more likely among those with higher levels of alcohol use, illicit drug use, depression severity, and physical/sexual violence in the adjusted model. There was a positive, dose-response relationship between number of pills given to peers in the last 30 days and VS likelihood (aPR: 1.05, 95% CI: 1.02, 1.08; p < 0.01). Giving pills may strengthen peer relationships, which may facilitate ART adherence. ART distribution through peer networks holds promise as a context-appropriate intervention for improving ART adherence among FSW in this setting.
Background
Female sex workers (FSW) have 13.5-times the risk of acquiring HIV compared to other women in low and middle income countries, and just 57% on antiretroviral therapy (ART) are estimated to have reached viral suppression (VS) globally.1,2 HIV prevalence among FSW in South Africa ranks among the highest in the world at estimated 62%.1,3-5 Research indicates recent improvements in continuum of care indicators, particularly HIV testing and ART coverage, among South African FSW in settings where sex worker-friendly programming is available.3,4,6 However, VS has been slower to progress, and only 56% of FSW living with HIV are virally suppressed (HIV RNA VL <1000 copies/mL).4,7 Maximizing ART adherence is key to increasing VS among FSW living with HIV, which in turn improves morbidity, mortality, and quality of life, and reduces risk of onward transmission of the virus.8-11 Research is needed to better understand determinants of adherence and develop tailored interventions for FSW in this context.
Barriers to adherence among FSW living with HIV globally include stigma from HIV clinic providers and partners, substance use, depression, food insecurity, violence, homelessness, and poverty.12-22 Social support from sex worker peers, friends, family, and partners,14,23-25 and positive perceptions of HIV providers20,21 appear to facilitate treatment adherence. Few studies have focused on factors influencing ART adherence among FSW living with HIV in the South African context despite their particularly heavy HIV burden. 26 One national survey found that FSW receiving HIV testing and treatment services through specialized sex work programs had a higher odds of VS compared to those who were not receiving these services through a sex work program. 4 In eThekwini (Durban), Parmley et al (2020) found that work-related migration, substance use, and anticipated stigma from FSW peers, clients, and sex work venue managers hampered FSWs’ access to HIV clinics for obtaining ART and their ART consumption. Sharing ART pills with peers was one strategy FSW used to overcome, and help others overcome, these barriers and avoid ART interruption. 26
ART sharing is a form of ART diversion, the distribution of controlled drugs from an intended user or use to an unintended user or use, encompassing multiple practices such as selling, trading, sharing, recreational misuse, and stealing drugs. 27 Limited research has investigated drivers of ART diversion and how it may affect ART adherence. Most diversion studies focus on non-sex working people in the U.S., such as those who buy and sell ART within illicit markets to meet economic and drug dependency needs28,29 and men who have sex with men (MSM) who use ART for HIV pre- and post-exposure prophylaxis.30-32 In southern and eastern Africa, research describes diversion of ARTs for recreational purposes among adolescents and adults (eg consumption as part of a drug cocktail).33-35 Similar to Parmley and colleagues (2020) above, Rosen et al 36 found that ART pill sharing among FSW peers and fisherfolk in Uganda was a common mode of overcoming occupation-related barriers to ART adherence, such as mobility and stigma. Parmley's and Rosen's qualitative findings suggest that ART diversion within peer networks could lead to higher levels of adherence and VS among FSW by helping them surmount social and occupational ART barriers. However, ART diversion is feared to lead to non-adherence, incorrect dosing, mixing types of ART, treatment failure, and ART resistance,37,38 and U.S.-based studies provide evidence that those who divert ART may be less likely to be ART adherent compared to others.29,39
To advance understanding of ART diversion and its consequences for treatment success among FSW living with HIV, we assessed the magnitude and correlates of sharing and its relationship with VS among FSW in eThekwini, South Africa's largest city.
Methods
Study Setting and Procedures
We analyzed baseline survey data (May 2018-March 2020) from Siyaphambili (n = 1391), a randomized intervention trial including FSW living with HIV in eThekwini, South Africa, in the Province of Kwa-Zulu Natal. Approximately 10,000 women practice sex work in eThekwini, more than half of whom are living with HIV, with prevalence peaking at nearly 90% for FSW 30–34 years. 40 Sex work is illegal in South Africa, and sex workers, clients, and brothel managers are subject to arrest and prosecution. 41 Antiretroviral therapy is available to FSW at no cost from TB HIV Care, a non-profit organization implementing the largest key populations program for FSW in the area, as well as from local primary health care centers.42,43 FSW were recruited and screened for eligibility within their communities from TB HIV Care's mobile vans and drop-in center by FSW peer case managers and other trained staff. 44
Ethical Approval and Informed Consent
Trained research assistants obtained voluntary written informed consent from participants, administered the baseline survey, and provided reimbursement. All consenting participants provided whole blood samples drawn by a clinician to assess baseline CD4 count and viral load following enrollment. 44 The Siyaphambili study protocol was approved by the University of the Western Cape Biomedical Research Ethics Committee in South Africa; the Johns Hopkins School of Public Health Institutional Review Board in the United States (approval number IRB00008196), and the eThekwini Municipality and KwaZulu-Natal Provincial Departments of Health.
Study Population
Women were eligible if 18 years of age or older, cisgender, reported earning at least half of their income through exchanging sex for money or goods (the definition of sex worker used by TB HIV Care), diagnosed with HIV for more than six months, not on ART or on ART for two or more months (to ensure time for VS), Zulu or English speaking, not pregnant at the time of enrollment, and not planning to relocate or travel outside of eThekwini for more than two months in the next year. 44
Measures
All Measures Were Self-Reported Except VS
Dependent Variables
Ever shared (given and/or received) ART. In two separate questions, participants were asked if they had ever received anti-retroviral medication (ARVs) from a sex work friend or peer, and if they had ever given or provided their ARVs to an FSW friend or peer. Those who responded affirmatively to either question were considered to have ever shared ART.
Viral suppression (VS). Participants were categorized as virally suppressed if their viral load was less than 50 HIV RNA copies/ml based on study laboratory results.
Independent Variables
Number of ART pills shared with peers in the last 30 days. Participants reporting ever sharing ARVs with a sex work peer were asked two separate questions regarding how many pills they gave and received in the last 30 days. To create a variable reflecting total number of pills shared (given and/or received) with peers in the last thirty days, responses were summed; to increase interpretability, results were scaled to assess the impact of sharing three pills. As the regimen in South Africa is one pill per day, every three pills taken over a three-day period represent a 10% increase in adherence. Two additional variables separately reflecting number of pills given to peers (per three pills given) and number of pills received from peers (per three pills received) in the last thirty days were also used in analyses.
Alcohol use frequency. Participant alcohol use frequency was assessed using a question from the AUDIT-C scale 45 that asked participants how often they have a drink containing alcohol: never, monthly or less, two to four times a month, two to three times a week, or four or more times a week.
Illicit drug use. Any versus no drug use in the past month was assessed based on participants’ reported use of marijuana, cocaine, “whoonga”/ “nyaope”/“sugar” (stimulants), ecstasy, “tik” (methamphetamine), heroin, crack/rock, “flakk” (bath salts), or other drugs in the past 30 days.
Homelessness. Participants reporting being homeless or living in a shelter in the past six months were categorized as homeless, while staying at a friend's or family's place, renting or owning a place, or staying in student housing or a brothel in the past six months were categorized as not homeless.
Lack of safety in daily life. The extent to which participants felt unsafe in their daily life was assessed by a question asking participants how safe they feel in daily life: not at all, a little, moderately, and very safe.
Violence victimization. A binary variable was created to assess the experience of physical and/or or sexual violence victimization. Participants who responded affirmatively to either of two violence questions adapted from the WHO Violence Against Women Instrument 46 -- “Has someone ever physically hurt you (pushed, shoved, slapped, hit, kicked, choked, or otherwise physically hurt you?” and “Has someone ever forced you to have sex when you did not want to?” – were categorized as having experienced violence victimization.
Depression severity. The Patient Health Questionnaire-9 (PHQ-9) was used to assess depression severity. Scores were coded as none/minimal, mild, moderate, moderately severe, and severe based on PHQ-9 standards. 47
Social support. Level of social support was assessed using the Social Support Scale (SSS), 48 which asked participants questions about how often they have various types of support, such as help if they were confined to bed or someone to confide in. A variable with three categories – low, moderate, and high—was created using tertiles of SSS scores ranging from 0–100.
Worksite. A binary variable reflected type(s) of worksites in which participants did sex work. Reporting sex with clients in a private home, brothel, bar, private party, hotel or guest house, or shelter were categorized as “indoor,” while reporting sex with clients in the street, park, public garden, beach, cemetery, or private vehicle were categorized as “outdoor.”
Mobility. A binary variable reflected mobility in the past six months based on participant reports of spending any nights outside of eThekwini in that period.
Enough money to meet needs. A three-category variable (not at all; a little; moderately, mostly or completely) was created using a question regarding the extent to which participants had enough money to meet their needs.
Manager. Participants reported whether or not they shared earnings with a person who provides a service when they sell sex, including but not limited to arranging clients or providing physical protection.
Enacted stigma. Enacted stigma is defined as the experience of being discriminated, stereotyped, or prejudiced against due to a social characteristic, eg living with HIV or sex working. 49 An HIV stigma variable was created by combining responses to seven binary survey items into a sum score (see Supplemental material A), which ranged from 0–7 and was treated as a continuous variable. A sex work stigma variable was created by combining responses to ten binary survey items into a sum score, which ranged from 0–10 and was included as a continuous variable. Enacted HIV stigma items and enacted sex work stigma items exhibited adequate internal reliability (Cronbach's alpha = .64 and 0.60, respectively). See Supplemental Material A.
Anticipated stigma. Anticipated stigma refers to expectations of discrimination, stereotyping, and/or prejudice from others due to a social characteristic, eg living with HIV or sex working. 49 An anticipated HIV stigma variable was created by combining responses to four binary survey items into a sum score (see Supplemental material A), which ranged from 0–4 and was included as a continuous variable. An anticipated sex work stigma variable was created by combining responses to five binary survey items into a sum score, which ranged from 0–5 and was included as a continuous variable. Internal reliability for anticipated HIV stigma items (Cronbach's alpha = .71) and anticipated sex work stigma items (Cronbach's alpha = .61) exhibited good and adequate fit, respectively. See Supplemental Material A.
Socio-demographic control variables: Age (18-24 years [adolescent girls and young women] vs 25 years + ), educational attainment (none to any years primary school; incomplete secondary school; complete secondary school; any years university or technical school), HIV status disclosure to family and/or partners, and relationship status (single; steady cohabiting partner; steady non-cohabiting partner).
Statistical Analysis
We described the prevalence of ever sharing ART and magnitude of ART sharing in the last thirty days (number of pills). We used multivariable robust Poisson regression to separately assess correlates of ever sharing and the relationship between number of pills shared in the last 30 days and VS (<50 copies/mL). We produced descriptive statistics for all variables and unadjusted bivariate associations between independent variables and the ever shared outcome. Furthermore, to assess the appropriateness of combining those who gave and received pills in the ever shared outcome, we used Pearson's chi-squares, Fisher's exact tests, and Wilcoxon-Mann-Whitney tests to assess differences in characteristics between those who had only ever received pills and those who had only ever given pills. Factors examined as correlates of sharing were identified in the literature as structural, psychological, and behavioral barriers to ART access and adherence experienced by FSW, which could spur ART sharing among peers.12-20,26 Variables related to ART sharing in bivariate models with p-value<0.20 were included in multivariable sharing correlates model. Finally, we examined the relationship between the number of pills shared in the last thirty days and VS in three separate models in which the focal explanatory variable was number of pills given and/or received; number of pills given; or number of pills received. These models controlled for structural, psychological, and behavioral variables believed to be predictors of both sharing and VS.
We assessed multicollinearity among independent variables based on correlations (>0.8) and variance inflation factors (≥10), and linearity of relationships using Loess curves. 50 To address missing data, we conducted multiple imputation using fully conditional specification with 20 imputations to address missing values. All analyses were conducted using SAS (version 9.4) statistical software.
Results
Study Population and Prevalence of ART Sharing
Overall, 890/1391 FSW enrolled into the trial were on ART and 50.0% of those had reached VS. Nearly one-third (30.2%) of participants on ART reported ever sharing (giving and/or receiving) ART pills with peers, 92.1% of which did so in the past 30 days (median pills shared: 3 [IQR:1-6; range: 0-34]). Among those who had ever shared (n = 269), 85.5% gave pills (n = 230), 62.5% received pills (n = 168), 48.0% both gave and received pills (n = 129), 37.5% only gave pills (n = 101), and 14.5% only received pills (n = 39).
Participants who ever shared (gave and/or received) and never shared ART differed statistically on relationship status, educational attainment, alcohol use frequency, illicit drug use, depression severity, physical and/or sexual violence victimization, and enacted and anticipated sex work stigma (Table 1). Those who had shared ART were more vulnerable compared to those who never shared—eg 65% of those who shared versus 54% of those who never shared used drugs in the previous month (p < 0.01) and 67% of those who shared versus 53% of those who never shared had ever experienced sexual and/or physical violence (p < 0.01)—although those who had any university or technical level education were more likely to have shared than those with no or primary-level education (7% vs 2%, respectively; p = 0.02). In addition, those who shared were more likely to have a steady non-cohabitating partner compared to those who never shared (40% vs 16%, respectively; p < 0.04). Participants who only ever gave and who only ever received pills did not differ statistically from one another on socio-demographic or behavioral characteristics (Supplemental Material B) and thus a combined sharing (giving and/or receiving) variable was used for the sharing correlates analysis.
Socio-Demographic and Behavioral Characteristics of FSW Living with HIV in eThekwini (Durban) by Ever Shared ART Pills (n = 889).

Chi-square p-values are reported for categorical variables and Wilcoxon-Mann-Whitney test p-values are reported for quantitative variables.
Missing n = 1; cMissing n = 19; dMissing n = 10; eMissing n = 11; fMissing n = 3; gMissing n = 2.
Indoors includes private home, brothel, bar, private party, hotel or guest house, or shelter; outdoors includes street, park, public garden, beach, cemetery, or private vehicle.
Homeless includes no place to live or staying in a shelter; not homeless includes staying with friends or family, at a brothel, in student housing, owning a place or renting a place.
Motivating Factors for ART Pill Sharing
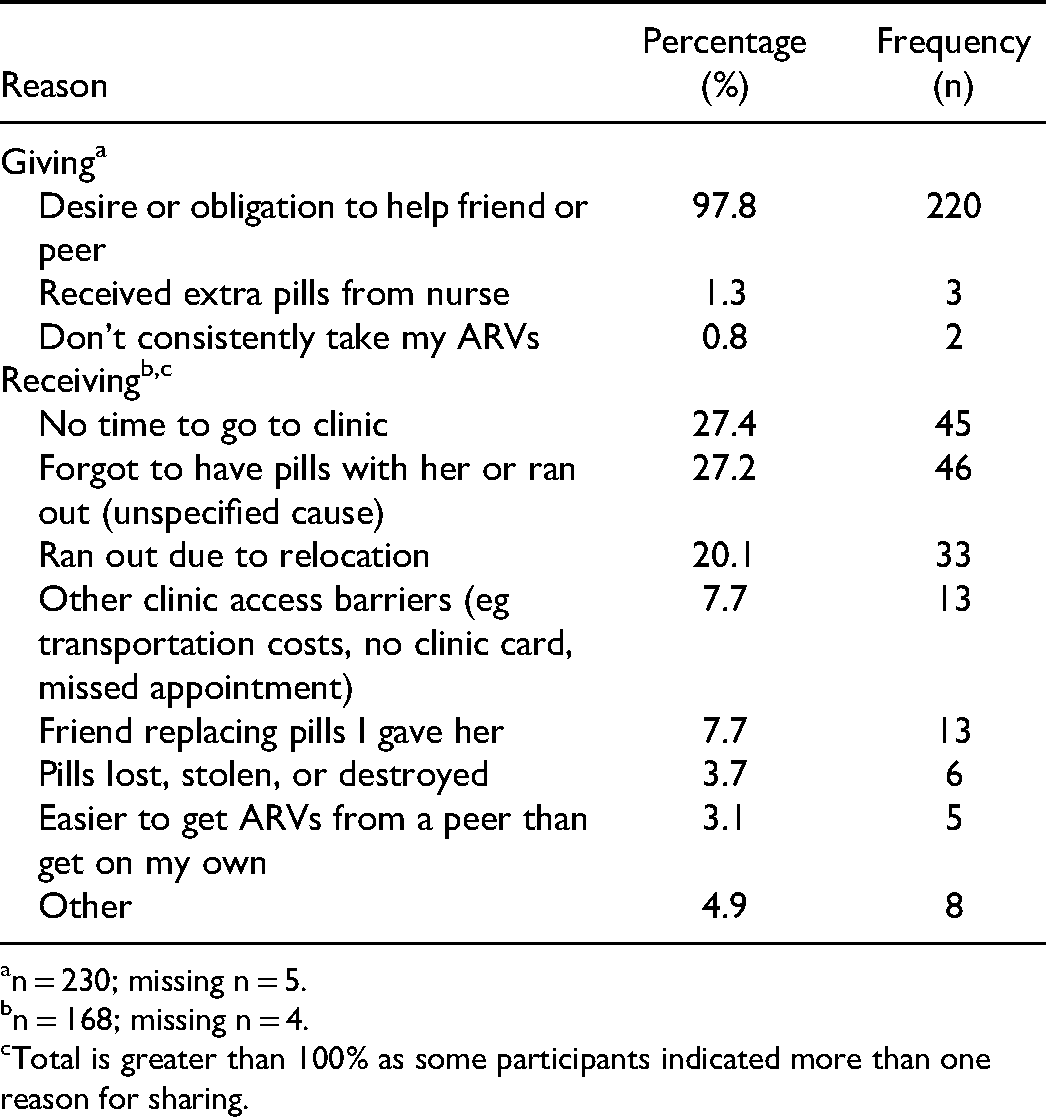
Table 2 presents reasons participants shared ART pills with peers. Nearly all (97.8%) participants who gave pills indicated that the desire or obligation to help a friend or peer was a reason they gave pills to peers, and a few reported receiving extra pills from a nurse (1.3%) and/or not consistently taking their ART (0.80%) as reasons they gave pills to peers. The most commonly reported reasons for receiving ART pills from peers were not having time to go to the clinic to collect pills (27.4%), forgetting to have pills with them or running out of pills (27.2%), and running out of pills specifically due to relocation (20.1%). Additional reasons for receiving pills from peers included other clinic access barriers (eg transportation costs, no clinic card, missed appointment) (7.7%), a friend replacing pills previously shared (7.7%), pills lost, stolen, or destroyed (3.7%), ease of access from a peer (3.1%), and other (4.9%).
Reasons for Giving and Receiving ART Pills among FSW Living with HIV who Ever Shared ART in eThekwini, South Africa (n = 269).
n = 230; missing n = 5.
n = 168; missing n = 4.
Total is greater than 100% as some participants indicated more than one reason for sharing.
Factors Associated with Ever Sharing ART
In bivariate analyses (Table 3), having a steady cohabitating partner and level of social support were significantly, negatively associated with ever sharing ART; factors significantly, positively associated with sharing ART with peers were greater alcohol use frequency, illicit drug use, symptoms of depression, and lifetime physical and/or sexual violence. In the adjusted model (Table 3), the following factors were significantly, positively associated with the likelihood of ever sharing ART: alcohol use frequency (monthly or less vs never: aPR: 1.54, 95% CI: 1.07, 2.20; 2-4 times/month vs never: aPR: 1.74, 95% CI: 1.25, 2.42; four or more times/week vs never: aPR: 2.02, 95% CI: 1.46, 2.82); illicit drug use (any drug vs none in past month: aPR: 1.25, 95% CIL 1.01, 1.55); depression severity (minimal vs none/minimal: aPR: 1.39, 95% CI: 1.00, 1.92; moderate vs none/minimal: aPR: 1.92, 95% CI: 1.34, 2.74; moderately severe vs non/minimal: aPR: 2.13, 95% CI: 1.48, 3.06), lifetime physical and/or sexual violence (aPR: 1.41, 95% CI: 1.13, 1.77), and university or technical level education (vs no or primary level education: aPR: 2.30, 95% CI: 1.03, 5.10). In the sharing correlates multivariable model, Pearson correlation coefficients and VIFs of explanatory variables were, respectively, under 0.8 (max: 0.53) and 10 (maximum: 1.5), indicating non-multicollinearity.
Factors Associated with Ever Sharing (Giving and/or Receiving) ART among FSW Living on HIV Treatment in eThekwini, South Africa (n = 890): Unadjusted and Adjusted Relationships.

Indoors includes private home, brothel, bar, private party, hotel or guest house, or shelter; outdoors includes street, park, public garden, beach, cemetery, or private vehicle.
Homeless includes no place to live or staying in a shelter; not homeless includes staying with friends or family, at a brothel, in student housing, owning a place or renting a place.
Relationship Between ART Sharing and Viral Suppression
There was a positive, dose-response relationship between number of pills given and VS in the adjusted model presented in Table 4. For every three pills given, there was a 5% associated increase in the likelihood of VS (aPR: 1.05, 95% CI: 1.02, 1.08). Number of pills received was not associated with VS (aPR: 1.00, 95% CI: 0.95, 1.05) and number of pills given and/or received was not associated with VS (aPR: 1.02, 95% CI: 0.99, 1.05).
Associations Between Number of ART Pills Shared (per 3 Pills Shared) in Last 30 Days and Viral Suppression among FSW on HIV Treatment in EThekwini, South Africa (n = 890)a.

Multivariable robust Poisson regression models adjusted for age, educational attainment, relationship status, alcohol use frequency, illicit drug use, depression severity, mobility, worksite, sharing earnings with manager, recent physical or sexual violence, homelessness, having money to meet needs, safety, enacted sex work stigma, enacted HIV stigma, anticipated sex work stigma, anticipated HIV stigma and HIV status disclosure.
“Pills given” and “pills received” are not mutually exclusive as some participants both gave and received. Pearson correlation coefficients and VIFs of explanatory variables were, respectively, under 0.8 (max: 0.53) and 10 (maximum: 1.7), indicating that multicollinearity was not problematic.
Discussion
We found that sharing ART pills with peers was a common practice among FSW receiving treatment for HIV in eThekwini, South Africa. Moreover, factors that can impede ART access and adherence including violence victimization, alcohol use, illicit drug use, and depression were associated with increased likelihood of sharing. The number of pills given in the previous month was associated with increased likelihood of being virally suppressed. Our findings suggest that ART diversion may support adherence among FSW who give their pills to peers, contrary to fears of negative impacts of sharing on HIV treatment success. Furthermore, increasing engagement of FSW peer networks may constitute a promising, underutilized strategy for improving access to ART and HIV treatment success rates that programs could leverage.
Nearly a third of our sample reported ever sharing pills with peers, the vast majority of which did so in the last thirty days. Although those who reported only giving and only receiving did not differ, differences were observed between those who did and did not engage in any sharing of ART pills. Those with higher levels of alcohol use, illicit drug use, depression severity, and/or violence victimization—factors that have previously been identified as barriers to HIV treatment18,51-54—were more likely to share ART with peers, suggesting that sharing is a response to ART adherence barriers. These findings are consistent with qualitative findings from Uganda, where FSW and fisherfolk described pill sharing within their occupational networks as a measure commonly taken to overcome occupation-related mobility and other impediments to ART adherence. 36 Similarly, in a qualitative study in eThekwini, when experiencing ART shortages due to alcohol and drug use that interfered with clinic attendance, FSW borrowed pills from peers. 26 Barriers to taking ART pills they already possessed, such as alcohol intoxication, also spurred giving pills to others in need by leaving them with extra pills. 26 Longitudinal and qualitative studies should further examine the relationships we found between violence victimization, depression, substance use, and sharing to better understand their mechanisms and direction.
Our finding that more pills given in the last thirty days was associated with greater likelihood of VS suggests that sharing may enable improved ART adherence for some FSW. This is consistent with the finding that ART sharing was more frequently discussed among FSW and fisherfolk reporting greater ART adherence in Uganda. 36 Giving pills to peers may constitute a supportive act that strengthens interpersonal peer relationships or FSW community social cohesion, ie trust, solidarity, and mutual aid in a given group. 55 Stronger peer relationships or more cohesive community may, in turn, support individuals’ ART adherence through various pathways, such as peers reminding each other to take pills, pooling money for transportation to clinics, or helping one another contend psychologically with stigma.23,25,26,56 Such benefits of strengthened peer relationships may outweigh any negative effects of sharing on ART adherence. Alternatively, giving may be characteristic of participants who have supportive relationships with peers that enable adherence. As the available survey measure of social support captured support from any source, we were not able to investigate the role of support specifically from peers in the relationship between sharing and VS—this is a needed area of further research.
In contrast to our findings, U.S.-based studies of low-income people who use substances and MSM have found lower self-reported adherence among those who divert ART compared to others.29,39 The discrepancy with our findings may be explained by differences in contexts of and motivations for diversion. While we and Rosen et al (2020) focused on ART diversion in the form of sharing with peers in order to maintain ART adherence or help peers do so, reasons for diversion among participants in the U.S. research included buying and selling ART via pill brokers in order to meet economic and substance use disorder needs. 29 Diversion motivated by the aim of maintaining ART adherence may tend to support adherence whereas diversion to achieve other aims may tend to undermine it. Additionally, while diversion in context of a peer network may have positive social effects (eg increased social capital or cohesion) that support adherence, diversion in an impersonal commercial market through illicit pill brokers likely would not have such effects. Finally, in a context like the U.S. where cost is a significant barrier to HIV treatment access, 57 it may be more difficult to replace shared pills—leading to greater likelihood of a negative impact of sharing on treatment adherence—than in a setting like South Africa where ART is available at clinics free of charge.
Overall, the consequences of ART diversion for ART adherence are likely not uniform but rather dependent on contexts and characteristics of diversion. Assessment of negative consequences of sharing among FSW, such as medication mixing, incorrect dosing, and resistance, is needed. The possibility of medication mixing is limited in this context, since regimens of ART are typically more uniform across non-facility-based providers serving FSW, but providers may offer varying regimens during roll-out of new regimens (eg dolutegravir). 58
Exchanging ART pills among FSW peers was commonplace, motivated by desire to help peers, and associated with greater likelihood of VS. Taken together, these findings suggest that distribution of ART through FSW peer networks could be a context-appropriate and effective intervention to increase treatment adherence among FSW in this setting. Though little studied, community-based distribution of ART through FSW peer networks has been successfully implemented in sub-Saharan Africa. In Uganda, in response to FSW advocacy for services already delivered to the general population, the AIDS Support Organization (TASO) conducted community ART delivery among FSW. 59 Peer support groups were formed and appointed peer leaders who distributed 3-month refills to group members, provided psychosocial support, and conducted monitoring of peer treatment. 59 Group members additionally received periodic clinical consultations and lab work to assess treatment success. 59 Such interventions may facilitate treatment adherence by building on existing pill sharing norms within peer networks while minimizing risks of negative consequences of informal sharing by supporting linkage to clinical services. 59
Limitations to our study include the cross-sectionality of the analyses, which impedes determination of causality as well as sharing patterns and their influence on VS over time. The cross-sectional design may also lead to underestimation of the relationship between pills shared in the last thirty days and VS, as effects of sharing on VS may not appear within the captured time period. Additional longitudinal assessments of the relationship over time may help to further unpack these relationships. Our findings may also not be generalizable to other groups of FSW. Study participants were recruited by a provider of HIV care and treatment for FSW, and thus likely have better than average access to these services. This may render them better able to manage potential negative consequences of pill giving, eg pill shortages. Finally, all measures except viral load were self-reported and thus subject to desirability and other forms of bias that could influence estimates.
Conclusions
This study expands the knowledge base on ART diversion and determinants of HIV adherence among FSW living with HIV in South Africa. Findings suggest that FSW peers share ART with peers as a consequence of barriers to ART adherence, including alcohol use, illicit drug use, depression severity, and violence victimization. Taken together with previous studies, our findings indicate that the impact of ART diversion on HIV VS depends on characteristics of diversion (eg giving vs receiving and motivations for diverting) and its context (eg within a social network vs commercial market). In eThekwini, South Africa, ART delivery strategies that build on FSW peer networks hold promise for improving health and wellbeing of FSW living with HIV. Future longitudinal research is needed to better understand positive and negative effects of ART sharing, including ART resistance, and mechanisms of the relationships we found.
Footnotes
Acknowledgements
We are grateful to the Siyaphambili study participants, community advisory board, and team members. This work was funded through National Institutes of Health National Institute of Nursing Research grant R01NR016650.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health National Institute of Nursing Research, (grant number R01NR016650).