
Abstract
Objective:
To determine the survival rate and predictors of HIV-infected children on antiretroviral therapy at two selected facilities in North Ethiopia.
Methods:
A facility-based retrospective cohort study was conducted in Debre Tabor General Hospital and Dessie Referral Hospital from December 2005 to November 2015. A total of 426 records were included in the study. Multivariable Cox proportional hazards regression model was used to identify independent predictors of survival.
Results:
At the end of follow-up, 97 (22.9%) HIV-infected children died and 325 (77.1%) were alive. The probabilities of survival at 12, 24, 36 and 48 months of on antiretroviral therapy were 0.91, 0.85, 0.84 and 0.80, respectively. The median survival time was 91.6 months (95% confidence interval: 89.0–94.2). Almost half (51%) of the deaths occurred within the first 2 years of treatment. Study participants who had poor adherence to antiretroviral therapy (adjusted hazard ratio = 3.0; 95% confidence interval: 1.2–7.5) and who started antiretroviral therapy with lower baseline weight-for-age Z-score (adjusted hazard ratio = 2.5; 95% confidence interval: 1.1–6.1) were significantly associated with high risk of mortality. On the other hand, study participants with a baseline CD4 count above 200 cells/mm3 (adjusted hazard ratio = 0.7; 95% confidence interval: 0.4–0.9) and those participants who had psychosocial support during follow-up (adjusted hazard ratio = 0.03; 95% confidence interval: 0.1–0.7) were significantly associated with less mortality event.
Conclusion:
Mortality of children on antiretroviral therapy was high. The risk of mortality is increased if the child was underweight at the commencement of antiretroviral therapy, had lower baseline CD4 count, had poor adherence to antiretroviral therapy and had no psychosocial support. Concerned stakeholders should focus on antiretroviral therapy adherence, nutritional interventions, psychological support and early initiation of antiretroviral therapy regardless of their CD4 count to enhance survival of HIV-infected children on antiretroviral therapy.
Background
Globally, approximately 34 million people were living with human immunodeficiency virus (HIV) as of 2011 and 3.3 million of them were children under 15 years. 1 More than 90% of these children are living in sub-Saharan Africa.2,3 In Ethiopia, more than 1.2 million people were living with HIV/AIDS by the year 2010. Out of these, 79,875 were children, which makes Ethiopia a country with an unacceptably high and overwhelming burden of HIV/AIDS.4,5
Antiretroviral therapy (ART) has improved the survival of HIV-infected children by boosting their immune function through increased CD4 lymphocyte count, decreased viral load and decreased HIV/AIDS-associated manifestations and minimized the risk of opportunistic infections (OIs).5–14 However, not all patients have an optimal response to ART, and they are exposed to morbidity and mortality. 10
The government of Ethiopia launched its ART initiative in 2003 based on a subsidized fee-based approach. Subsequently, the service was rapidly scaled up with the help of global and national initiatives, and ART has become available free of charge since 2005. 15 The ART program was significantly scaled up by decentralizing it to health centers in 2006 and implementing a nationwide campaign to achieve national targets for both ART and HIV testing and counseling, as recommended by the World Health Organization (WHO).15,16 The number of children enrolled in HIV/AIDS care and treatment program has increased in Ethiopia. 16 Despite the scale-up of ART, retention of patients and early mortality remain major challenges for the programs. 17 Some studies conducted in Ethiopia have shown that death of HIV-infected children after commencing ART ranged from 4.8% to 7.5%.18–20
Being WHO HIV/AIDS stage III and IV, anemia, poor adherence to ART, CD4 count <200 cells/µL during the commencement of ART, not taking cotrimoxazole preventive therapy (CPT), chronic diarrhea, OIs and nutritional status were some of the predictors of HIV-infected child mortality.7,18–22 The survival rate of HIV-infected children who have enrolled in ART care and support was a less researched area in Ethiopia. The findings of this study will contribute to the HIV-infected children’s survival rate literature and knowledge page to inform policymakers, program planners, clinician’s decision makings, ART care and support workforce and other interested stakeholders. Hence, the main purpose of this study was to determine the survival rate and its predictors among HIV-infected children on ART in Northern Ethiopia.
Materials and methods
Study design and setting
A facility-based retrospective cohort study design was conducted in Debre Tabor General Hospital (DTGH) and Dessie Referral Hospital (DRH) in Amhara Regional State, Northern Ethiopia among HIV-infected children (2 months to 14 years old) who have started ART from December 2005 to November 2015. The ART case-team in the hospital comprised trained physicians, nurses, pharmacists, laboratory technicians, data clerks and ART education adherence counselors. During baseline assessment of the cohort, a total of 3293 children had enrolled in the HIV care in DTGH (n = 201) and DRH (n = 3092). Of these, 200 and 1540 children were on ART during end line follow-up evaluation at DTGH and DRH, respectively. 7 HIV-infected children were assessed for nutritional status, screened for OIs and evaluated for clinical staging and eligibility for ART by nurses and physicians.
Study participants and eligibility
All HIV-infected children who were enrolled in ART care and support from December 2005 to November 2015 in the two hospitals were the study participants in this follow-up study. Known HIV-infected children (aged 2 months to 14 years) who had started ART at two hospitals within this period were included in the study. Unfortunately, children who had not taken CD4 count at the time of starting ART and who were losses to follow-up or transferred to other facilities were excluded from the study (Figure 1).

Schematic presentation of study participants’ recruitment and allocation process.
Adherence was assessed in the past 1 month of the date for the interview so as to determine the optimal adherence level. For an adequate level of viral load suppression, the patient needs to take 95% of the prescribed doses. According to the Guidelines for Pediatric HIV/AIDS Care and Treatment in Ethiopia (2008), good adherence is defined as taking 95% and above of the prescribed doses per month. Poor adherence is defined as taking less than 85% of the prescribed doses. Such information is already filled in the ART follow-up form as good and poor.
A developmental milestone is also categorized as development appropriate to age, developmental delay and developmental regression. When we say development appropriate to age, the child has the ability to perform the four developmental milestones which include cognitive development, gross motor/fine motor, language and social development according to the child’s age. Developmental delay is a delay in an age-specific ability for important developmental milestones and developmental regression is when a child loses an already achieved skill or fails to progress beyond a prolonged plateau after a period of relatively normal development.
Sample size determination and sampling procedure
The sample size was calculated by considering the two-population proportion formula using Epi Info version 7 and taking type one error 5% and 80% power. Two populations were categorized by CD4 count as the main exposure variable for HIV-/AIDS-related deaths during the follow-up period. The estimated proportion of probability of survival of children whose CD4 count was below the threshold was 56%. 19 Then the total sample size, after adding 5% as incomplete or inconsistent data, was 426 for exposed and non-exposed subjects. 19
Sampling procedure
Sampling frame containing 1740 medical records of HIV-infected children on ART from December 2005 to November 2015 at two hospitals were constructed. Then from the sampling frame, participants that fulfill the eligibility criteria were selected randomly using computer generating a random number. The primary outcome variable was time to event in months. HIV-infected children who began ART were followed until the date of death or censored. The survival time was calculated in months using the time between the date of treatment initiation and date of the event (death or censored). The predictor variables were caregivers’ age, caregivers’ sex, caregivers’ educational level, caregivers’ marital status, occupation, residence, functional status, WHO HIV/AIDS clinical stages, CD4 count, substance use and OIs (Figure 1).
Data collection procedures
The data were collected using a standard checklist adopted from ART intake and follow-up form and by reviewing similar literature. 23 Necessary information was extracted from electronic and paper-based ART registration and follow-up records in the ART clinics. Participant’s characteristics such as socio-demographic characteristics, residence, nutritional status, disclosure status, duration on ART (in months), presence of OIs, baseline and current WHO HIV/AIDS clinical staging and baseline and follow-up CD4 cell counts were retrieved from the clinical records of the HIV/AIDS patients and recorded on the data extraction sheet by trained ART data clerks. Four data clerks and two BSc nurses were employed as data collectors and supervisors, respectively. Data on deaths of the HIV-infected children on ART were obtained from medical cards.
Data quality control
Pre-testing was undertaken at Woreta Health Center before data collection and modification were made accordingly. Training was provided to a data clerk and two BSc nurses about the overall data collection process.
Data processing and analysis
Data were entered in Epi Info version 7 and exported to SPSS version 20.0 for further analysis. Descriptive statistics (mean, median and standard deviation (SD)) were computed. The Kaplan-Meier log-rank model was applied to estimate the survival time of HIV-infected children in ART care and support. Bivariate and multivariate Cox proportional hazards regression models were used to identify the predictors of mortality. Those variables with p-value ⩽0.2 in the bivariate analysis were included in the multivariate Cox proportional hazards model. The independent predictors of mortality were identified using adjusted hazard ratios (AHRs) at 95% confidence interval (CI) and p-value < 0.05.
Results
Socio-demographic characteristics of study participants
Of 462 study participants, 426 complete information was collected. Thirty-six questionnaires were excluded due to incompleteness. The majority (80.1%, n = 341) of the caregivers were female: 280 (63.4%) were married; 169 (39.6%) were illiterate, whereas 162 (38%) had completed primary school; 253 (59.4%) were Orthodox Christians; 334 (78.4%) were urban dwellers; and 204 (47.9%) were housewives. Regarding children, 217 (50.9%) children were female. The mean age at the commencement of ART was 77.3 (± 42.5) months (Table 1).
Socio-demographic characteristics of study participants on ART at two selected hospitals, 1 December 2005–31 November 2015 (n = 426).
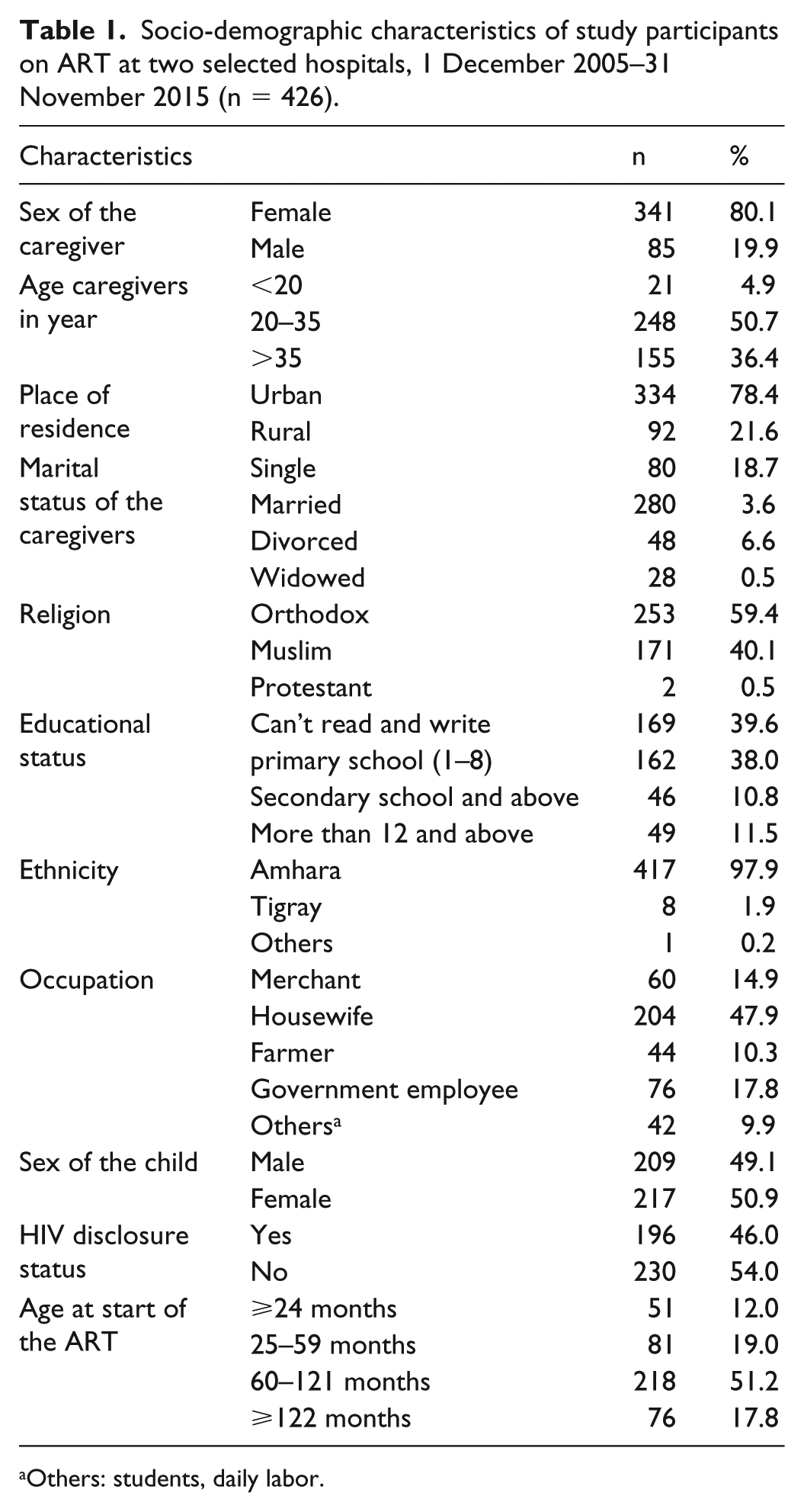
Others: students, daily labor.
Clinical and immunological status of HIV-infected children on ART
Of 426 HIV-infected children, 399 (93.7%) were in WHO HIV/AIDS clinical stage (I and II) and 170 (39.9%) had nutritional support. Of these, 148 (35.3%) and 46 (11.1%) of the children had less than 200 cells/mm3 CD4 count during baseline and end line assessment, respectively. The majority (83.8%, n = 357) were on CPT, 208 (48.8%) were moderately malnourished, 183 (45.0%) had anemia (<10 gm/dL), 240 (56.3%) had a history of OIs and 259 (62.3%) had no psychosocial support during follow-up. Eventually, 97 (23%) died and 325 (77.0%) were alive during the follow-up period (Table 2).
Clinical and immunological status of children on ART at two selected hospitals, Northern Ethiopia, 1 December 2005–31 November 2015.

OIs: opportunistic infections; TI: treatment stage I; TII: treatment stage II; TIII: treatment stage III; WHO: World Health Organization; ART: antiretroviral therapy.
Survival status of HIV-infected children after initiation of ART
A follow-up was carried out for 120 months with a median of 44 months that contributed a total of 18,583 child-months. The median survival time was 91.6 months (95% CI: 89.0–94.2). The cumulative probabilities of survival at 12, 24, 36 and 48 months of ART were 91%, 85%, 84% and 80%, respectively. The mortality rate was found to be 52.2 deaths per 10,000 child-months or 6.3 deaths per 100 child-years (Figure 2).

Kaplan-Meier survival curve among children on ART at Debre Tabor General Hospital and Dessie referral hospital, 1 January 2005–31 March 2015.
Predictors of mortality after initiation of ART
The hazard of child mortality was three times higher among children with poor adherence to ART than children who had good adherence to ART (AHR = 3.0, 95% CI: 1.2–7.5). In addition, children who had severe malnutrition during the commencement of ART had 2.5 times higher hazard of death than their counterparts (AHR = 2.5, 95% CI: 1.1–6.1). On the other hand, the hazard of mortality decreased by starting ART while children’s baseline CD4 cell count was above 200 cells/mm3 (AHR = 0.7, 95% CI: 0.4–0.9) and providing psychosocial support during follow-up (AHR = 0.03, 95% CI: 0.1–0.7) (Table 3).
Bivariate and multivariate Cox regression analysis of HIV-infected children on ART 1 December 2005–31 November 2015.

OIs: opportunistic infections; CPT: cotrimoxazole preventive therapy; HR: hazard ratio; CHR: crude hazard ratio; AHR: adjusted hazard ratio; Ref.: reference; WHO: World Health Organization.
p-value ⩽ 0.05.
Discussion
This study assessed the survival of HIV-infected children after initiation of ART and predictors of mortality at DTGH and DRH, Northern Ethiopia. Almost one-in-five HIV-infected child (22.9%, n = 97) deaths were recorded in 6.3 deaths per 100 child-years. This finding is higher than studies conducted in the Asia Pacific region (6.8% and 1.9 death/100 child-years), 18 Tigray Region, Ethiopia (4.81% and 1.4 deaths/100 child-years, 19 Felege Hiwot Referral Hospital, Ethiopia (7.5% and 4 deaths/100 child-years, 20 a study from Kenya 8.4%), 21 and Kinshasa, Democratic Republic of the Congo (10.1% and 3.2 deaths/ 100 child-years) 24 .
In this study, the majority (51%) of the deaths occurred within the first 2 years after starting ART. This finding is similar to the studies conducted in other places,18,19,21,25 reporting that the mortality rate was high in the early period after commencing ART. This premature mortality could be due to delays in ART initiation which decreased the risk of OIs and improved survival of HIV-infected children.
In this study, the hazard of mortality was high on HIV-infected children who had severely malnourished during the commencing ART. This finding is consistent with studies conducted in the Asia Pacific region, 18 Zambia, 25 Tanzania, 26 Ghana 27 and Ethiopia. 28 However, HIV-infection can also cause malnutrition associated with diarrhea, and also malnutrition has a negative influence on body resistance to infections that may speed up HIV-infection’s progress.26,29 The finding also showed that the hazard of mortality was high on HIV-infected children who had poor adherence to ART. This finding is consistent with a study conducted in the Asia Pacific region, 18 South Africa 30 and Ethiopia. 31 This could happen because poor adherence to ART negatively affects the suppression of viral replication, increasing the risk of drug resistance and treatment failure.
The hazard of mortality among HIV-infected children who had psychosocial support during follow-up was less than those children had no psychosocial support. This finding is consistent with a study conducted in Uganda, 33 a systematic review conducted by the United States Agency for International Development (USAID). 33 Moreover, the finding is also supported by national and international guidelines.23,34 In this study, the hazard of mortality was less among HIV-infected children who had a baseline CD4 count (above 200 cells/mm3) than those children who had less than 200 cells/mm3 during initiation of ART. This finding is consistent with other similar studies.10,18,21,30 This is because with a lower CD4 count, the immune system will be very weak and the patients are vulnerable to OIs they could normally fight off. In this study, more than half (56.3%) of the children had OIs during their follow-up period.
However, the present study does have some inherent limitations. Due to financial constraint, survival and predictors of mortality after initiation of ART was assessed retrospectively instead of prospectively. As data were collected from secondary sources, incompleteness, loss or transfer out was inevitable, and it was difficult to assess clinical and immunological responses. As a result, the study may fail to assess possible causes of death.
Conclusion
The hazard of mortality was higher among HIV-infected children in the early period of initiation of ART. Children with malnutrition while the initiation of ART, poor adherence to ART and lack of psychosocial support were significantly associated with HIV-infection related-mortality. Hence, assessment of nutritional status and adherence to ART should be carefully monitored. Further attempts are needed to encourage health care workers, families and community supporters to provide psychosocial support.
Footnotes
Acknowledgements
We are very grateful to Debre Tabor University for financial support. Our gratitude also goes to supervisors, the data collectors and the staff at the ART clinic of DTGH and DRH. G.A. designed the study, performed the statistical analysis and drafted the article. M.A., T.W. and A.S. participated in the study design and statistical analysis. T.W. and A.S. have drafted the article. All authors contributed their intellectual inputs, read and approved the final version of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance was obtained from the Institutional review board of Debre Tabor University. Following the approval, the official letter of co-operation was obtained from the College of Medicine and Health Sciences (Ref. no. DTU/RP/144/15) and given to the hospital managers, medical directors and ART focal persons.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been financially supported by Debre Tabor University for data collection. No fund received for publication of the article.
Informed consent
Permission was obtained from the hospital’s administration and ART focal persons before data collection. As we used a medical record review, written informed consent was not sought from the patients directly. However, retrospective data were collected anonymously. Confidentiality of participants’ information was maintained by collecting the de-identified (using unique ART number) data. As we used a medical record review, we were waived to use the participants’ de-identified data by the ethical review board/committee. Following the approval, official letter of co-operation was given to the hospital managers, medical directors and ART focal persons. Then, we obtained consent from the hospital’s administration and ART focal persons. Retrospective data were collected anonymously and confidentially.