
Abstract
Introduction
Tuberculosis (TB) is the leading cause of death in human immunodeficiency virus (HIV)-infected people worldwide. Patients with HIV and latent TB are 20 to 30 times more likely to develop active TB. 1 Integrated antiretroviral therapy (ART) early in the treatment for tuberculosis is recommended due to improved morbidity and mortality, 2 However, there can be serious drug interactions.
Among ART, dolutegravir (DTG) has been recommended as one of the first line medication for HIV by the World Health Organization. 3 DTG is metabolized mainly by the uridine diphosphate/glucuronosyltransferase; but is also a minor substrate for the cytochrome P450 (CYP) system. Rifamycins are potent inducers of the CYP3A4 isoform, which can cause sub-therapeutic concentrations of anti-retroviral drugs, 4 among these, rifabutin (RBN) is a less potent inducer of CYP3A4. Pharmacokinetic (PK) studies done on healthy adults showed that rifampin decreased DTG concentrations by more than 50% whereas RBN decreased it by 30%. Current recommendation is for DTG to be dosed twice daily with rifampin, while a daily dose of DTG was recommended with RBN. 5
RBN has been preferred given that its favorable pharmacokinetic and toxicity profile. 6 Currently there are no studies examining the use of RBN and DTG in co-infected persons. This is a case series of 4 co-infected patients receiving both agents who underwent PK analysis.
Methods
We carried out a retrospective chart review of patients in the respiratory care unit (RCU) at Jackson Memorial hospital in Miami, Florida. Inclusion criteria included: patients older than 18 years old, concomitant diagnosis of HIV and active TB, receiving DTG and RBN, and undergoing measurement of DTG and RBN plasma concentrations. Furthermore, the adherence of these medications is high as these patients were evaluated in the inpatient setting where administration of medications is monitored by clinicians.
Blood Sample Collection
On admission to RCU, the patients are started on a TB regimen and undergo PK sampling 2 weeks after the regimen is established. When changes are made to the TB medications, or HIV medications are added, a repeat sampling is done. Blood sampling is done when fasting.
DTG: Samples are drawn at the end of dosing interval to assess trough plasma concentration (Cmin) and at 2 and 6 h to assess peak (Cmax) concentration. The typical DTG peak and trough concentrations are approximately 3.3 mcg/mL and 0.80 mcg/mL, respectively. 7 However, we do agree that there is an acceptable range and trough concentrations that may be higher than the in vitro protein-adjusted IC90 for wild-type virus.
RBN: Samples are drawn at 3 and 7 h to assess peak plasma concentration (Cmax) to capture either early or delayed absorption. Expected concentrations are 0.45-0.9 mcg/mL. 8
Pharmacokinetic Analysis
Blood samples were sent to the Infectious Disease Pharmacokinetics Lab at the University of Florida in Gainesville, Florida. Phoenix® WinNonlin® v.8.0 (Certara USA, Inc., Princeton, NJ, USA) was used to perform the non-compartmental analysis and calculate the area under the concentration-time curve (AUC) for DTG and RBN. The area under the concentration-time curve for the dosing interval (AUC0-tau) and 24-h period (AUC0-24) were calculated. AUC0−tau and AUC0−24 were extrapolated from the elimination phase captured during the PK sampling of each drug. If the elimination phase was not captured during that time, the AUC0−last sample was reported instead. Tables 1 and 2 shows the calculated AUCs for DTG and RBN. In addition to therapeutic drug monitoring (TDM), patients underwent blood collection for evaluation of CD4+ cells and viral loads.
Patients’ Pharmacokinetics of DTG.

AUCX−Y: area under the concentration-time curve from time X to Y hours; AUC0−tau: area under the concentration-time curve from time zero to the end of the dosing interval; DTG: dolutegravir; TDM: therapeutic drug monitoring.
AUC0−6 was calculated.
Ethical Approval and Informed Consent
Our study was approved by the institutional review board, University of Miami, Jackson Memorial Hospital; number: 20191069. This is a retrospective study with chart review for data collection; no written informed consent was required by the institution.
Results
Four patients met inclusion criteria during the years 2017 and 2018.
Patient 1
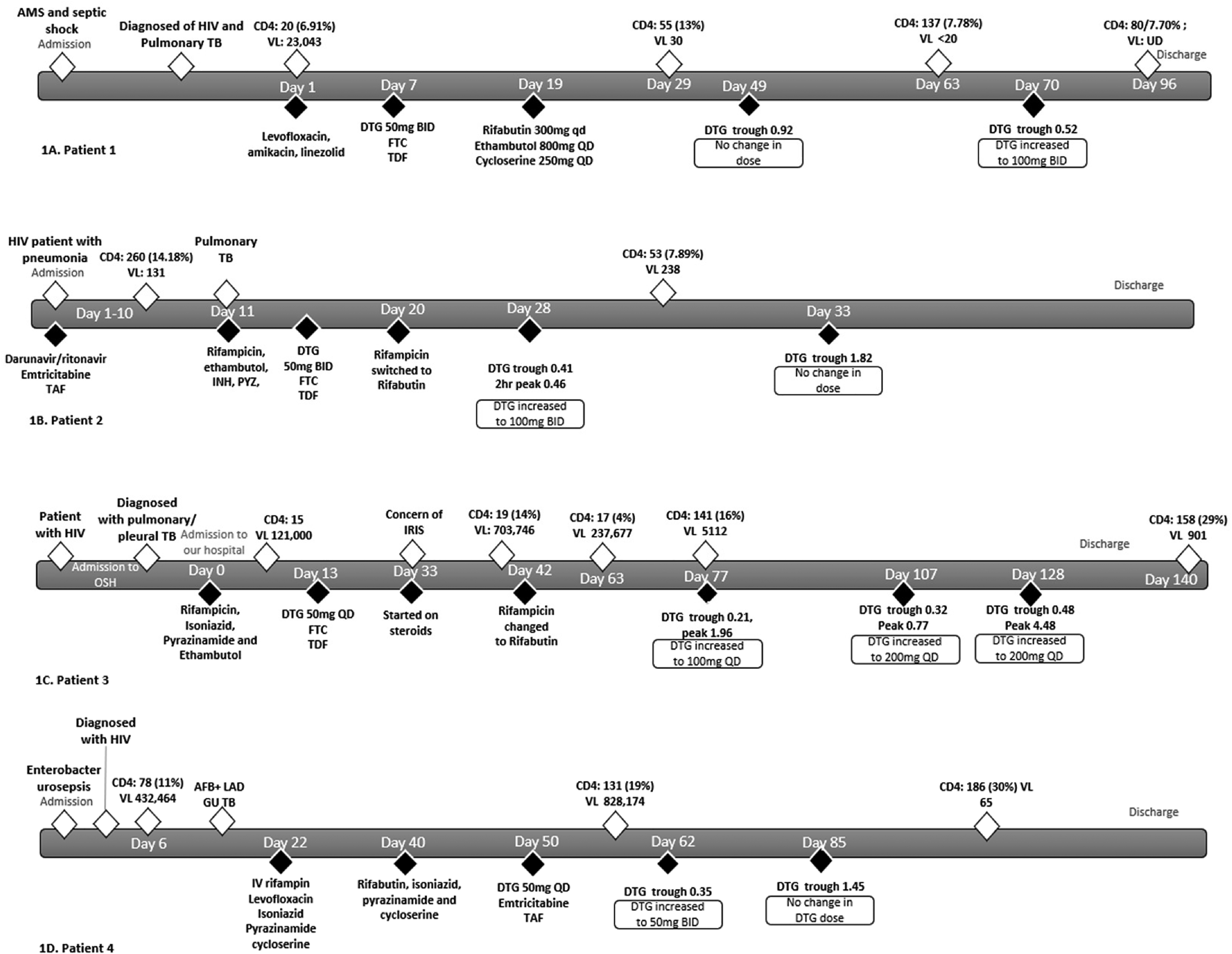
34-year-old, prior healthy, male hospitalized with septic shock; diagnosed with acquired immunodeficiency syndrome (AIDS) and pulmonary TB. Initial evaluation revealed a CD4+ of 20cells/mcL and a viral load of 23 043 copies/mL. Polymerase Chain Reaction testing of sputum was negative for rpoB mutation. Due to elevated liver enzymes, he was started on a liver sparing regimen consisting of levofloxacin, amikacin, and linezolid. Seven days later, the patient was started on ART including DTG 50mg twice a day, emtricitabine (FTC) and tenofovir disoproxil fumarate (TDF) daily. Once his condition improved, treatment was changed to RBN 450 mg three times weekly, ethambutol 800 mg daily, and cycloserine 250 mg daily. Twenty-two days after initiation of ART, a repeat CD4+ cell improved with a viral load of 30copies/mL (Figure 1A). TDM was performed 30 days after the new TB regimen was started, DTG trough was 0.92 mcg/mL, and the RBN concentration was 0.65 mcg/mL. No changes were made to either medication. On day 51 after RBN was started, TDM was repeated; DTG trough was 0.52 mcg/mL and RBN peak was 0.37 mcg/mL. DTG was increased to 100 mg twice a day, and no changes were made to RBN dosing. One month later, the viral load was undetectable.
Patients’ clinical course.
Patient 2
68-year-old male with HIV diagnosed 12 years ago, on darunavir/ritonavir, emtricitabine and tenofovir alafenamide. He was admitted for pneumonia and found to have TB diagnosed with a positive GenExpert without evidence of rpoB mutation. On admission, the CD4+ was 260 cells/mcL and a viral load of 131 copies/mL. The patient was started on rifampin, isoniazid, pyrazinamide, and ethambutol. ART was changed to DTG 50 mg twice a day, FTC, and TDF. Nine days after treatment was started, rifampin was switched to RBN 300 mg daily. Eight days later, TDM was performed, and DTG trough was found to be 0.41 mcg/mL, and RBN peak was 0.12 mcg/mL. DTG was increased to 100 mg twice a day (Figure 1B), and RBN was increased to 600 mg daily. Testing at this point showed no significant change in low level viremia with a drop in CD4+ cell count, 238 copies per mL and 53cells/mcL respectively. Five days after, the dose of DTG was increased, TDM of DTG revealed a trough of 1.82 mcg/mL and RBN a peak of 0.53 mcg/mL at 7 h. The same dose of both medications was continued. Patient was discharged but lost to follow up.
Patient 3
41-year-old woman with a history of poorly controlled HIV and a history of refractory headaches, cough, and fevers; admitted to an outside hospital. Patient was diagnosed with pulmonary TB complicated with pleural effusion and pleural loculations requiring chest tubes; CD4+ on admission was 15 cells/mcL with a viral load of 121 000 copies/mL. Lumbar puncture was negative for TB central nervous system involvement. She was started on rifampin, isoniazid, pyrazinamide, and ethambutol and then transferred to the RCU unit in our hospital. Patient was started on DTG 50 mg daily, FTC 200 mg, and tenofovir 300 mg 13 days after admission. Twenty days after ART was started, patient started developing fevers; a presumptive diagnosis of immune reconstitution inflammatory syndrome (IRIS) was made, and she was started on prednisone. On day 42, rifampin was switched to RBN 300 mg daily. During hospitalization, patient underwent multiple TDMs (Figure 1C). 35 days after RBN was started, DTG trough was 0.21 mcg/mL and RBN peak was 0.88 mcg/mL. DTG was increased to 100 mg daily, and RBN dose was not changed. One month later, TDM was performed again with a DTG trough concentration of 0.32 mcg/mL and RBN peak of 0.26 mcg/mL. The RBN dose was increased to 450 mg daily and DTG was increased to 200 mg daily. Three weeks later, DTG trough value was 0.48 mcg/mL and RBN peak was 1.01 mcg/dL. Patient was discharged with that dose. 12 days after the last medication adjustment, the patient's CD4+ was 158 cells/mcL, with a viral load of 901 copies/mL reflecting a 2 log10 drop in viral load.
Patient 4
54-year-old man admitted to the hospital with sepsis of urinary source caused by Enterobacter spp. Found with advanced HIV infection with profound immunosuppression. Further work up revealed diffuse intra-abdominal lymphadenopathy. A lymph node biopsy showed necrotizing granulomas with acid fast bacilli present; GeneXpert confirmed M. tuberculosis, without rpoB mutation. Initial evaluation revealed a CD4+ 78 cells/mcL with a viral load of 432 464 copies/mL. Patient was started on intravenous rifampin and levofloxacin and oral isoniazid, pyrazinamide, cycloserine due to concern of poor absorption. Due to stable and at-goal concentrations of these medications 18 days later, he was switched to oral medication, including RBN 300 mg daily, isoniazid 450 mg daily, pyrazinamide 1250 mg daily and cycloserine 250 mg daily. About a month later after diagnosis, patient was started on ARTs at DTG 50 mg daily and emtricitabine and tenofovir alafenamide. Twelve days later TDM was performed, DTG was found to be 0.35 mcg/mL, and dose was increased to 50 mg twice a day. The RBN peak was 0.44 mcg/mL, so the dose was unchanged. Prior to this change, CD4+ was 131 cells/mcL (19%) with a viral load of 828 174 copies/mL. TDM, which was done 23 days later, revealed an appropriate DTG trough (1.45 mcg/mL) and RBN was 0.37 mcg/mL. Doses of both medications were maintained unchanged. Prior to discharge, the patient's CD4 improved to 186 cells/mcL with a viral load of 65 copies/mL.
Two months after discharge, he was readmitted with congestive heart failure due to tricuspid valve endocarditis due to Enterococcus spp. Unfortunately, he had multisystem failure, later transferred to hospice and where he passed away.
Patients’ Pharmacokinetics of RBN.
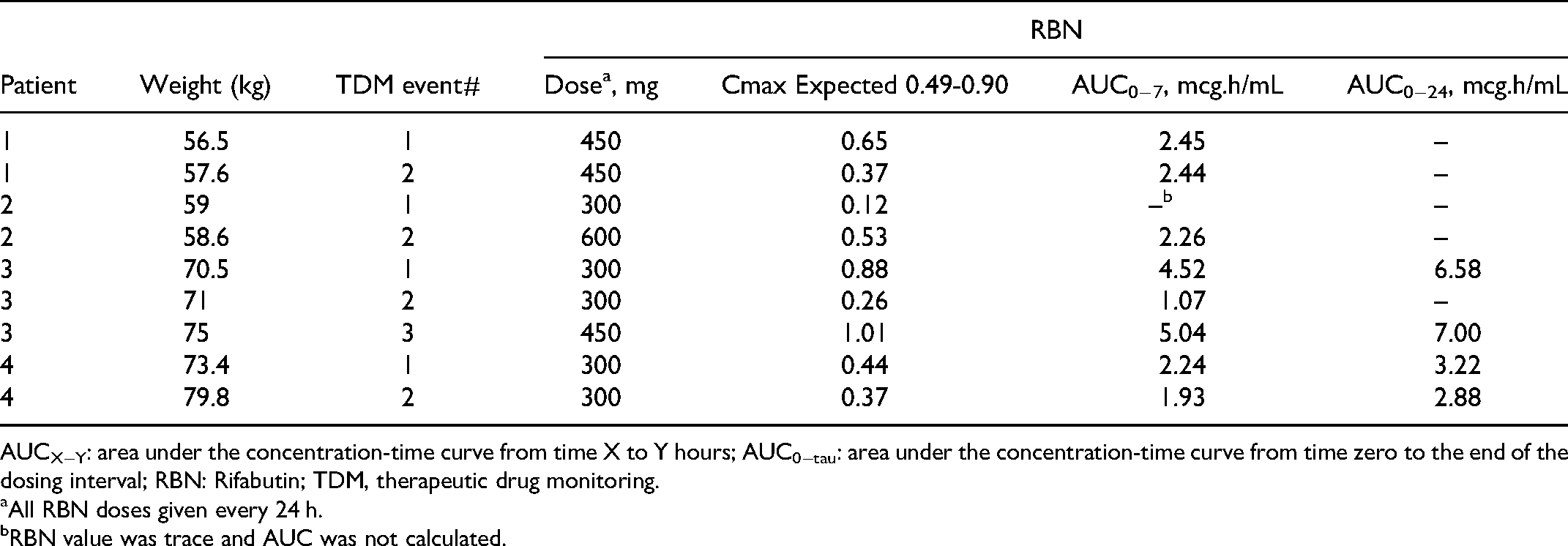
AUCX−Y: area under the concentration-time curve from time X to Y hours; AUC0−tau: area under the concentration-time curve from time zero to the end of the dosing interval; RBN: Rifabutin; TDM, therapeutic drug monitoring.
All RBN doses given every 24 h.
RBN value was trace and AUC was not calculated.
Discussion
Drug Concentrations
All 4 cases had lower than expected DTG concentrations at least once, including those patients on the current recommended dose of DTG when used with RBN, and even those receiving higher doses. Patient 1 had a within range concentration on first TDM, but lower than expected on second TDM on the same dose. Patient 2 had first TDM eight days after changing treatment from RIF to RBN. It takes about 2 weeks for the CPY 3A4 system to readjust from the induction effects of RIF after it is stopped; thus, the first TDM may had been impacted by residual effects of RIF. RBN concentrations were frequently lower than expected, requiring dose adjustment. In three of the patients who had low DTG concentrations, the RBN concentrations were also lower than expected. Therefore, it is difficult to determine how much of the lower DTG concentrations were a direct result of RBN induction of the CPY 3A4 system. This may be also related to poor gastrointestinal malabsorption as it has also been shown in critically ill patients as well as patients with HIV.9‐12 This was also recently shown in our target population by Le et al, who found significant reductions of DTG trough concentrations by 59% and low average trough concentrations as well in the patients taking RBN concomitantly. 13
Virologic Response
Incomplete virologic response has been defined as failure to suppression viral load to <200 copies/mL after 24 weeks of treatment, 14 Patient 1 had viral suppression with increased CD4 cell count 8 weeks after starting ART. Patient 2, who presented with low level viremia, had no change in viral load, with a significant decrease in CD4 cell count 6 weeks after he was changed from a protease inhibitor-based regimen to a DTG-based regimen. Patient 3 had a 2 log10 drop in viral load, with an increase in CD4 cell count after 13 weeks of ART. Patient 4 had a 4 log10 drop in viral load and increased CD4 cell count after 4 weeks of ART.
In HIV-infected patients naïve to treatment who are started on DTG, the median drop in VL is 3.4 logs after 4 weeks of treatment. 15 In our report, one patient had an adequate virologic response after 8 weeks of treatment. Two patients had a decrease in viral load, but complete suppression of virus could not be determined due to short periods of observation. For the patient who had his ART switched, there was no change in low level viremia with a decrease in CD4 count 6 weeks afterwards.
Conclusion
All patients with HIV and TB who were treated with RBN had low concentrations of DTG.
There was evidence of a favorable response to treatment in 2 patients, with a less than robust response in the others. Adequate suppression of viral load could not be determined for 3 of the patients because of the short time of observation. This case series demonstrates that for optimal concomitant use of rifabutin and dolutegravir it is highly recommended to use TDM. The published recommended doses can lead to subtherapeutic concentrations, and if the doses are not adjusted, this may lead to therapeutic failure and probably increase drug resistant strains in both HIV and TB infections. Prospective clinical studies are needed to further determine the PK interactions between RBN and DTG and virologic response to treatment.
Limitations
This is a small retrospective study using convenience PK sampling in a clinical setting. Full PK curves could not be collected. Adequate virologic response could not be determined on all patients due to short periods of observation. The lower DTG concentrations were consistent with induction of the CPY 3A4 system by RBN, but other contributing causes could not be ruled out. Finally, some of the RBN concentrations were low, but the minimum amount of RBN required for enzyme induction has not been determined. On the other hand, we do not have more patients undergoing TDM in our hospital system as these are usually performed when admitted due to the severity of the disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Our study was approved by the institutional review board, University of Miami, Jackson Memorial Hospital; number: 20191069. This is a retrospective study with chart review for data collection; no written informed consent was required.