
Abstract
Non-Langerhans cell histiocytosis is a rare disease which seldom affects adults. We report a case of a 32-year-old Bulgarian woman living with HIV. She developed severe anemia, extreme splenomegaly, requiring splenectomy and vertebral tumor formations leading to fracture. The diagnosis was confirmed by histological examination of the spleen, but subsequently questioned and a cumulative disease was discussed. After genetic testing, a cumulative disease was ruled out and the condition was determined to be Non-Langerhans cell histiocytosis. According to literature data, the disease has a high mortality rate. However, in our case, we should also note that there was a delay in diagnosis by several months due to difficulties in the clarification of the hematological disorder.
Intoduction
We report a case of a 32-year-old Bulgarian woman with HIV infection and Erdheim-Chester disease (ECD). We found no cases in literature of Erdheim-Chester disease in HIV-infected patients. ECD is a rare disease in adulthood, with no more than 100 cases described with a slight predominance of male gender.1–3
Case Presentation
The patient was admitted to the Department of Acquired Immune Deficiency for the first time on November 18, 2020 and was hospitalized for 3 months. Upon admission to the ward, the patient was febrile, with clinical manifestations of pneumonia - cough and shortness of breath, cachexia and candidal plaques in the oral cavity. The laboratory tests revealed severe anemia (hemoglobin values of 54 g/l) and elevated leucocytes upon admission (11,2 G/l). There were no pathological changes in the patient's biochemical profile. The patient's immune status revealed extremely severe immune deficiency as follows: Cluster of differentiation 4 (CD4) + T-cell count of 12 cells/µl; CD8 + T-cell count of 347 cells/µl. Her viral load (VL) was 10 1000 c/µl. The patient's x-ray showed bilateral pneumonia, and microbiological analysis showed Pneumocystis jirovecii and Candida albicans from sputum, as well as Candida albicans from throat secretions and faeces. Accordingly, the patient was treated with trimethoprim-cotrimoxazole, fluconazole, and antiretroviral therapy (ART) was initiated with emtricitabine/tenofovir alafenamide/darunavir/cobicistat. The patient was discharged from the department at the end of February, after the pneumonia had cleared, with negative microbiological tests, and controlled immune status as follows: CD4 count at 144 cells/µl; CD8 count at 1278 cells/µl. Her VL was 313 c/µl. At the end of March, she was hospitalized again because of high fever, chills, vomitting and severe lethargy. Laboratory tests showed severe anemia again - hemoglobin values of 45 g/l and thrombocytopenia - 109 G / l, with high c reactive protein (CRP) – 208 g/l, low albumin - 20.3 g/l and elevated gamma-glutamyl transferase (GGT) - 244 IU/l. Lung radiography showed no pathological findings. Computed tomography of the abdomen showed expressed hepatosplenomegaly. Of the microbiological tests performed, only Candida albicans was isolated from the faeces. During the hospitalization, the patient received empirical antibiotic combination - Ceftriaxone + Vancomycin, Fluconazole, multiple blood transfusions and infusion of human albumin. During the hospitalization, the patient had a temporary improvement of her condition, but a gradual progression of splenomegaly was observed. On April 20, due to acute pain in the left hypochondrium, the patient was transferred to a surgical clinic, where splenectomy was performed, with evidence of multiple splenic infarctions. Histological examination of the spleen showed histiocytic infiltration and the diagnosis of Erdheim Chester's disease was observed. After discharge from the surgical clinic, the patient was referred to the hematology department to clarify the diagnosis. During the hospitalization of the patient in the hematology ward in May, Gaucher's disease was observed, for which samples for genetic testing were sent to Germany. Meanwhile, during spontaneous bending, the patient suffered severe back pain and was immobilized from the waist down, experiencing severe back and limb pain. A magnetic resonance imaging /MRI/ revealed tumor formation and fracture of the ninth vertebra (Figures 1 and 2), similar tumor formations of the sixth thoracic and first lumbar vertebrae. In May, the patient's immune status and viral load were as follows: CD4 + T - cell count of 164 cells/µl; CD8 + T - cell count of 1634 cells/µl; and viral load (VL) was undetectable <2° c/µl. The patient was referred to a neurosurgical clinic, where a biopsy of the relevant formations in the vertebrae was performed and the fracture was filled with bone cement. The histological analysis result of the material from the vertebrae showed an infiltration of macrophages/histiocytes with abundant, mostly small vacuolated or foamy rather than fibrillary cytoplasm. Immunohistochemical study revealed CD 68 ( + ) positive abundant cell composition, S100 granular and diffuse marking; PAH8 - negative marking. Simultaneously, we received the data from the enzyme tests for Niemann's - Pick and Gaucher diseases from Germany, which were negative. Under the corticosteroid treatment, the fever subsided, but the anemic syndrome and swelling of the lower extremities persisted. A tumor formation of the skull was also observed. It was located on the right temporal bone with dimensions of about 2 cm and was painless. Following another consultation with a hematologist and after obtaining consent for performing high-risk chemotherapy, she was transferred to the haematological clinic. The patient underwent two courses of chemotherapy with Ciclophosphamid, Prednisone, Vincristin. However, she died five days after the second chemotherapy treatment.
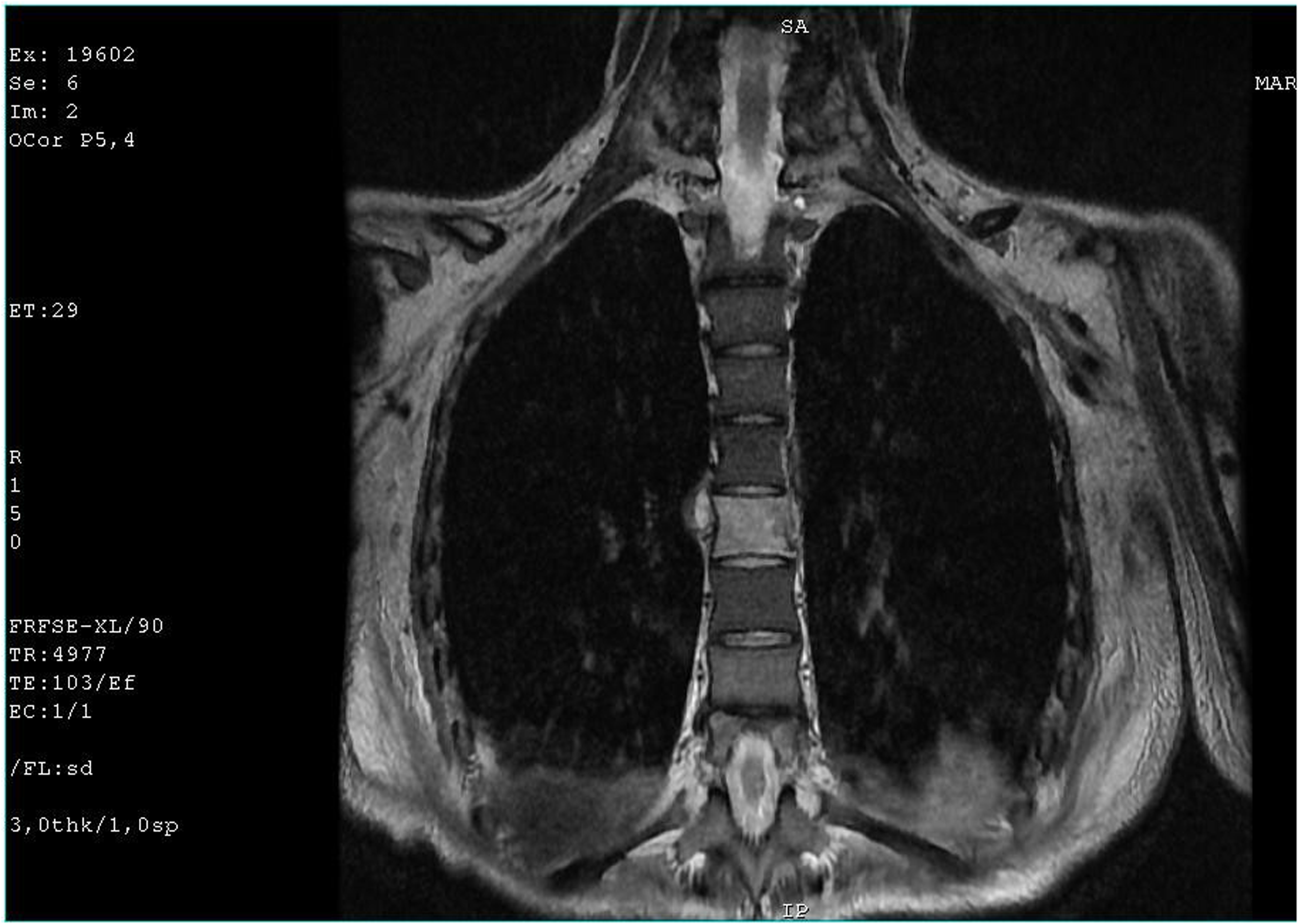
MRI revealed tumor formation and fracture of the 9th vertebra.

MRI revealed tumor formations of the 6th thoracic and first lumbar vertebrae.
Discussion
Erdheim-Chester disease (ECD) is characterized by the infiltration of tissues by foamy CD68( + )CD1a(-) histiocytes,3–5 as was found in our patient. In our patient, histiocytic infiltration involves the bones, which according to the literature data is observed in 15% of cases. 1 It has been established a high mortality rate associated with this disease.1–3 However, in our case, we should also note that there was a delay in diagnosis by several months due to difficulties in the clarification of the hematological disorder.
Conclusion
The presented case shows the need for a multidisciplinary team in clarifying comorbidities in patients with HIV infection, especially in the stage of advanced immune deficiency. We should point out the importance of recognizing a rare neoplastic disease in patients with HIV infection, especially in the course of immune reconstitution in patients with severe immune deficiency.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.