
Abstract
In India, the nationwide lockdown was implemented from March to May 2020 due to COVID-19 pandemic. As of March 2020, there were 13.08 lakh PLHIV availing ART free of cost from Government run ART centres, To maintain the continuum of care, National AIDS Control Programme (NACP) of India adopted Multi Months Dispensation (MMD) through ART centres and Community Dispensation of ART through the various Targeted Interventions (TI) and Community Based Organizations (CBO). A mixed methods study was designed, with desk review of programmatic data, semi qualitative interviews of 250 PLHIV and 15 In-Depth Interviews of ART centre and TI/CBO staff to document the process, strengths and challenges of these strategies in Surat city of South Gujarat. While administrative, technical and networking strengths were documented, manpower constraints, interrupted laboratory services, migration and relatively passive role of PLHIV in availing services were major challenges described in this study among several others.
Keywords
Introduction
National AIDS Control Programme (NACP) encompasses the major HIV/AIDS prevention and control activities in India. NACP, with a number of interventions in communication, counseling, diagnostics and treatment, has remained responsive to the changing epidemiological and sociopolitical scenarios concerning HIV/AIDS.1,2 The ability of the NACP to regularly deliver the Care, Support and Treatment facilities to the People living with HIV (PLHIV) and sustain them in HIV care-continuum cascade form the core of NACP interventions to achieve the 90-90-90 Fast-Track Targets 3 and the outcomes envisaged in the National Strategic Plan (NSP).4,5
COVID-19 pandemic was a unique challenge to the health systems, because it challenged the sustainability of the health care delivery system in the backdrop of a nationwide lockdown. In India, the first nationwide lockdown due to COVID19 pandemic 6 was between 24th March 2020 and 31st May 2020. The nationwide lockdown was anticipated to “pose major setbacks to previously gained successes of National health programmes”, 7 including HIV/AIDS. 8 The Global Fund to Fight HIV, TB and Malaria urged countries to “protect essential HIV services” by addressing the interruptions in HIV testing and treatment cascade. 9
One major intervention suggested by different agencies to continue Antiretroviral therapy (ART) dispensation during the lockdown was the Multi-Months Dispensation (MMD) and Community Dispensation of ART drugs. MMD and Differentiated Service Delivery (DSD) model are endorsed by the WHO with the objective of decreasing frequency of visits and hospital exposure among PLHIV, thereby reducing costs and increasing adherence. It is found to improve quality of care and is well suited to resource constrained health care systems.10,11
National AIDS Control Orgranization (NACO) adopted the MMD strategy, by which all stable patients on first line, second line ART and unstable PLHIV (after additional counseling) were given three months-MMD. 12 Apart from ART drugs, prophylactic drugs were also made available as multi-month dispensations. Community Dispensation (through Care and Support Centers, home delivery through Targeted Interventions/Community Based Organizations, PLHIV networks) was also adopted. 12
The process, operational successes and gaps in implementation of MMD and Community Dispensation of ART in the Indian setting need to be carefully documented to assess the suitability of strategies of MMD and Community Dispensation of ART on a long term, and during times of peace, war or pandemic. With this background, the present study was undertaken in Surat city of South Gujarat, India with the following objectives:
To document the Process of MMD and Community Dispensation of ART during the lock-down period, To explore the strengths and challenges of the MMD and Community Dispensation Strategies adopted during the lock-down period
Methodology
Study Setting
The study was conducted in the ART centre, attached to the Government tertiary care hospital of Surat and four Targeted Interventions (TI) of Surat city: PARAS PSM Unit II, PARAS PSM Unit III and Community Based Organizations (CBO): SAHYOG and Ekta Mahila Mandal. These TIs and CBOs cater to the welfare and health needs of female sex workers of Surat city.
Study Design
The study used a sequential, explanatory mixed-methods design. 13
Quantitative Methods
The ART centre staff and Project Managers of the four TI/CBOs were briefed about the study purpose and methods. Desk review of monthly progress reports of the ART centre was carried out to compare the variables of interest over a period of 2018–2020 with lockdown phase.
The semi-qualitative semi-structured questionnaire was piloted and peer reviewed before using in the study. The study team leaders trained a team of 7 field investigators in the use of this questionnaire, participation information sheet and obtaining written consent. The participants for the semi-structured interviews were 250 PLHIV who were recruited conveniently when they came for their regular visits to the ART centre or to the TI/CBOs, between 02 and 11 June 2021. Each investigator interviewed 5–10 participants per day, spending an average of 20 minutes with each participant. The investigators were trained in the use of a data validated Microsoft Excel 2010 sheet, in which the data collected was entered. The team leaders also verified the data entry by cross checking the manual entry of data with the Excel Sheet before analysis.
Qualitative methods: The qualitative responses in the semi structured interviews (less than 50 words each) were entered in a Microsoft Word document and treated as qualitative data. These questions focused on PLHIV's perspectives on challenges in availing HIV care and general health care services during lockdown, role of PLHIV network/TI/CBO and ART centre staff in providing services during lockdown, experiences regarding MMD and Community Dispensation of drugs. In Depth Interviews (IDIs) of four ART centre staff members, and eleven project staff of TI and CBOs were conducted. Participants were selected by purposive sampling and interviewed at their place of work. All the participants had rendered their services in the same capacity during COVID-19 pandemic. IDIs lasted for 45 minutes to 1 hour. The IDIs explored four main themes that had emerged through the desk reviews and semi qualitative interviews:
Procurement of ART drugs, logistics and commodities Planning and supplying ART through MMD and community dispensation. Human resource constraints Clinical experience with MMD and Community dispensation of ART.
The qualitative responses from 250 semi-qualitative interviews of PLHIV and 15 IDIs were transcribed and translated into English. The transcripts of IDIs were cross checked with the audio records for accuracy. Inductive coding was done using Atlas-Ti Software for thematic analysis of the transcripts.
Data Interpretation and Reporting
The main findings of quantitative and qualitative methods are presented together theme- by-theme, using a “weaving technique”. 14
Ethical Approval and Informed Consent
The study was approved by the Gujarat State AIDS Control Society (GSACS/SIMU/Research/2020-21/02/11010-13) and Institutional Human Research and Ethics Committee (No.GMCS/STU/ETHICS/27294, Government Medical College, Surat). Written informed consent was obtained from all the participants of the study.
Results
Process of MMD and Community Dispensation of ART
The process of MMD (from the ART centre and/or through peripheral health centre) and community dispensation of ART (through HIV care and support partners like TI/CBO/PLHIV networks/Care and Support organizations) was a step-wise activity, initiated at the ART centre and involving multiple partners such as health care staff of peripheral centres (PHC/CHC/sub district hospitals), TI/CBO and the PLHIV themselves (Figure 1).

Process of ART dispensation during COVID-19 lockdown with strengths and challenges.
Different approaches were used to cover beneficiaries in different “contexts”. Firstly, PLHIV residing within Surat city and capable of coming to the ART centre were given 3 months MMD from the ART centre itself. Secondly, a list of beneficiaries linked with different agencies such as TI/CBO was prepared for community dispensation of ART through these agencies. The beneficiaries who were staying in the city limits but unable to come to the ART centre were also contacted through the Care and Support Organization or PLHIV network. These agencies collected the ART from the Centre and dispensed them at the Drop In Centres or through house to house delivery. Thirdly, a list of beneficiaries who were residing outside the city limits but within the Surat district was prepared and drugs required for these PLHIV was calculated, to be dispensed through peripheral health centres. The ART drugs were transported to these peripheral health centres by the DAPCU (District AIDS Prevention and Control Units). PLHIV who had migrated outside the District were linked with nearest Government ART centres in their respective districts.
Strengths and Challenges of the MMD and Community Dispensation Strategies
The strengths and challenges faced during MMD and Community Dispensation of ART have been described under five different domains.
Human Resource Utilization Pattern at ART Centre
Systematic division of work
There was a systematic division of work among all ART centre staff based on geographic locations of peripheral centres and PLHIV's residences. This ensured effective communication with the healthcare staff of the peripheral healthcare centre and linkage of the PLHIV to these centres.
“We had adopted this strategy whereby each staff was assigned a group of peripheral centres. All the PLHIV who were to be given drugs through these centres had to be contacted by that particular staff. So were able to follow up the PLHIV, keep a track of who took the medicines, who did not and what problems were there. The staff members would be in touch with the counselor of those peripheral centres also.”—IDI3 (ART centre staff)
Timely intimation and follow up
All PLHIV were contacted telephonically by the ART centre staff at least two days prior to their due dates to inform them regarding the availability of MMD and where to avail them. They were also contacted by the peripheral health care centres or TI/CBO/CSO/PLHIV networks to confirm where and how the PLHIV wanted to collect the medicines. All the PLHIV were followed up by the ART centre staff again, to confirm whether they received the medicines and consumed them. This follow up phone call was used to enquire regarding the general well being of the PLHIV also.
Deputation of staff to COVID-19 duties
The process of communication with the PLHIV was a time consuming process
“There was a sense of burn out among counselors. We had to deploy counselors to COVID HelpDesk also. This also led to shortage here. So we had to manage the entire load of OPD and all the other work with half the number of counselors. Among those available, if one had to take a sick leave, it was even more difficult. During those special situations, we had to add more efforts to maintain the continuum of care among the beneficiaries and it was tiring. The only satisfaction is that we were able to deliver quality care to all.”—IDI 4 (ART centre staff)
Role of TI, CBO and Other Agencies
Networking with TI/CBO and other support partners
The ART centre has a well established network with the all the TI/CBO/PLHIV networks/Care and Support organizations working in the city for HIV care and support, who regularly help the ART centre in tracking “Missed” or “Lost to Follow Up” PLHIV. During the lockdown, these agencies also took up the responsibility of transporting ART drugs from the ART centre to PLHIV.
“When the PLHIV is associated with some NGOs or TIs there is a dual benefit. Firstly, we would have the phone numbers of responsible contacts of the PLHIV—such as an ORW or peer educator of the NGO. Secondly, the NGOs also have some responsibility in keeping a track of the PLHIV—has the PLHIV taken ART? Is the PLHIV still in the town? Has the PLHIV been linked in his hometown? Has the PLHIV missed out treatment or is lost to follow up? They have to report the same data. So they help in keeping a track of the PLHIV and help us providing the data.”—IDI4 (ART centre staff)
The TIs, CBOs and other HIV care and support partners regularly update all the treatment details of the PLHIV linked with them in a digital format.
“"I knew I had to come (to ART centre). But what would I tell my family? Earlier, my husband would go to work and children would go to school. I could come and take my medicines without letting them know. During lockdown, I had no reason to be out. So I called up Bhai (TI project staff). He told me not to worry—the next day I got my pills.”—P68 (40 year old PLHIV)
The peripheral health centres and TI/CBOs submitted a missing persons report if they failed to contact the PLHIV. These persons were included in the new list of beneficiaries by the ART centre staff, so that attempts were made to contact them again.
Response of PLHIV
Knowledge of PLHIV regarding treatment details and Migration
Among the 250 PLHIV interviewed in this study, MMD of ART and Community Dispensation of ART was done through the ART centre itself in 85.2% of the participants (Table 1). Among those who migrated, 82% collected MMD from the ART centre before leaving the city during the pandemic. On the other hand, among 7 of the 250 PLHIV interviewed, unplanned and hasty migration had resulted in missing ART.
ART Provider During COVID-19 Lockdown (n = 250).

The knowledge among the PLHIV regarding their ART treatment details and availability of ART across the country varied from person to person. While 63% knew how to contact the ART centre in case of emergency, only 39% knew that ART was available to them in designated Government centres anywhere in the country, free of cost.
Dependency on the TI/CBO to provide ART
It was noted that there were instances, where, some PLHIV who were linked to TIs or CBOs had become dependent on them for it.
“I got a call from one of our KPs (key population) one night. She was yelling at me—‘I don’t have any pills for tomorrow morning. Where are my pills? I told her that we will arrange it the next day. She shouted at me—‘How can you be so irresponsible? You have to supply ART on time’. She still had a few more days before her due date. If she had informed me earlier that something had happened to her pills, I would have arranged the refill."—IDI 12 (TI staff)
Fear of disclosure
The TI/CBO and ART centre staff had to take steps to protect confidentiality of the PLHIV. This had to be taken care of at all steps—during phone calls to the PLHIV, contacting PLHIV using local tracking mechanisms and delivering the ART. The fear of disclosure also led to refusal of ART in some PLHIV. Among the 250 interviewed PLHIV, 22% (55) said that they had asked the ART centre staff not to call or visit them, for the fear of disclosure.
“There were a lot of cases like that. For instance, there was one PLHIV who would not attend any calls of the ORW. Then we had to counsel the patient several times over phone. We explained how ART was being supplied to door step, even in times of complete lockdown. Then the PLHIV told that family members were home and none of them knew about the HIV status; “If I take these medicines from ORW and take it back home, they will ask me what it was. What can I tell them?”. Then the ORW acted as a friend who had come to meet and discreetly passed on the ART in a cover of sweets. Every situation was different and we had to sort out different ways to deal with each one of them.”—IDI3 (ART centre staff)
Fear of COVID-19
It was noted that fear of COVID-19 among PLHIV was one of the reasons for missing the visits to the ART centre. The COVID-19 hospital was located in a separate building, isolated from the rest of the hospital. In the main hospital building, all other services, except the ART centre and certain emergency services, remained closed during the lockdown. Nevertheless, the location of the ART centre in the same tertiary care hospital campus catering to COVID-19 patients “scared” the beneficiaries. The ART centre and TI/CBO staff engaged in repeated phone calls with these PLHIV to facilitate ART delivery.
Before the COVID-19 lockdown, 171 participants (68.4%) underwent general health checkup (other than HIV related) in the tertiary care Government hospital where the ART centre is located and 77 participants (30.8%) in other hospitals (Table 2). Of these, 17 had co morbidities such as Diabetes and Hypertension. During the COVID-19 lockdown, the number of PLHIV who underwent general health checkup in the tertiary care hospital decreased to 127 (50.8%). They sought medical care from ART Medical Officer, instead of General OPDs. This was attributed largely to the fact that the other General OPDs of the Government hospital catered exclusively to COVID-19 patients during the pandemic, while the ART centre remained functional throughout the pandemic. Thus, the number of medical checkup was restricted to the number of times the patient came for ART, which, according to the participants, was enough for chronic diseases such as Diabetes and Hypertension.
General Health Services Before and During Lockdown.

However, those who had acute illness and required medical attention went to other centres for treatment. About 41% participants (24) who availed general health care services in peripheral centres (PHC/CHC/UHC) reported that the quality of health care service was compromised during the COVID-19 lockdown, due to overburdened medical staff and preference to COVID-19 (or Acute respiratory illness patients). About 27% participants (10) who availed general health services in private hospitals recounted how the cost of treatment escalated during the COVID-19 lockdown.
Three participants had suffered from COVID-19 themselves. Among 28 participants who did not avail any general health services during lockdown, three participants had co morbidities and missed on their Anti-diabetic medications for varying periods of time.
Preference of location of ART centre
Among the 250 PLHIV interviewed, 25 participants had taken ART from other peripheral centres and 12 had “missed” on ART for varying periods of time before re-initiating ART at different peripheral centres. Thus there were 37 participants who had visited peripheral centres to receive ART. They were interviewed regarding their perspectives of receiving ART from peripheral centres, as opposed to the ART centre itself (Figure 2).
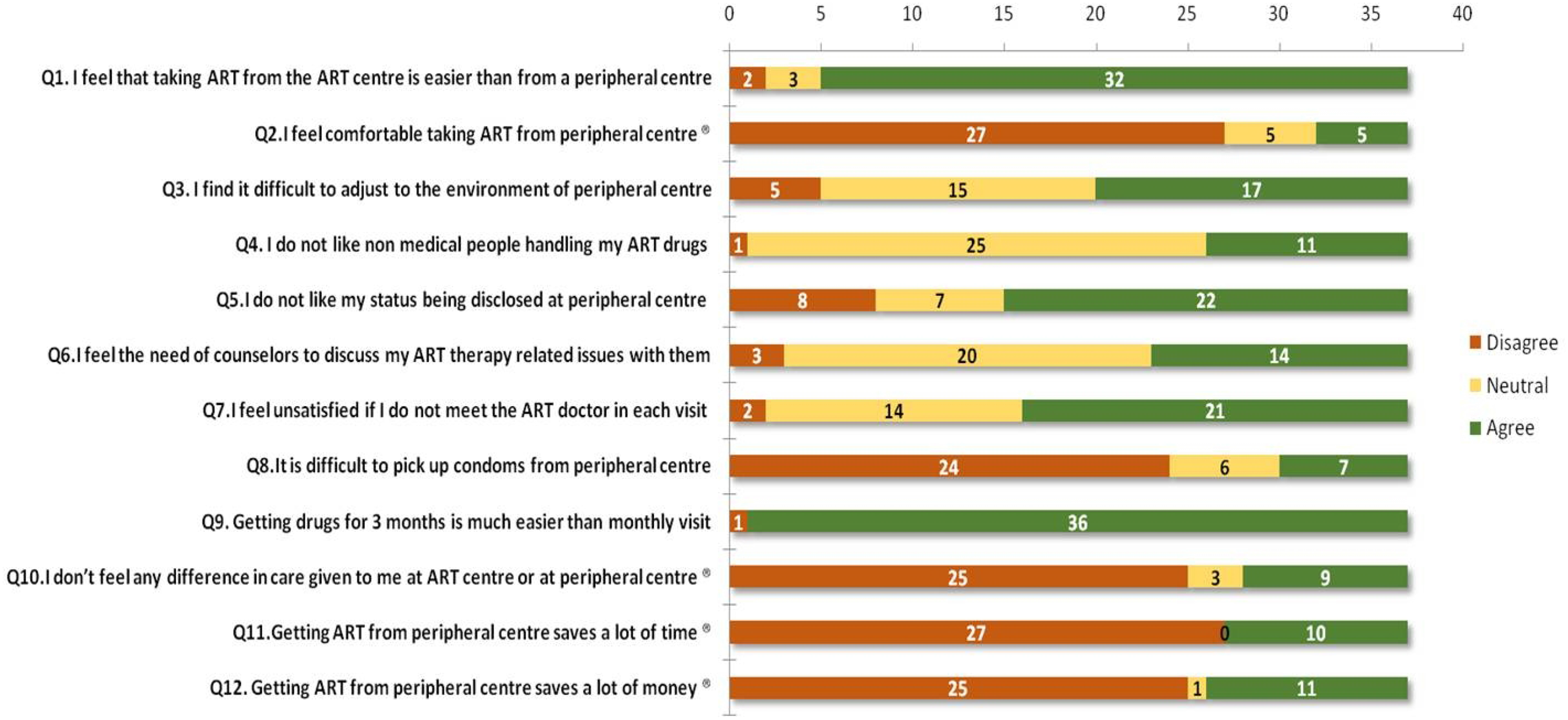
Participants’ perspectives on taking ART at ART centre compared to peripheral centre (N = 37).
One major reason to prefer taking ART from the ART centre was to maintain discretion, which was not possible in the peripheral Government health centres.
“Even before the lockdown, I knew that these medicines are available at our local Government Hospital. But I know many people there personally. So I do not wish to disclose my HIV status there. I am happy taking ART here. I have no issues travelling”—P29 (50 year old PLHIV from Tapi)
Government tertiary care hospital is one time stop for PLHIV to avail both HIV and non HIV related health services. This prompted them to prefer the ART centre at the tertiary care hospital over other levels of health care facilities.
“During lockdown, I got the pills from the nearby PHC. It was good, because I did not have to travel. But then, I cannot get this 6 monthly blood check up there. I cannot get my eye check up there. If I come here, I take medicines for myself, get blood tested and also take medicines for other sick family members.”—P49 (42 year old PLHIV from rural Surat)
The PLHIV who were interviewed also suggested that they preferred receiving ART through the dedicated ART centre since this meant that they did not have to wait in the queue with General outpatients. They were also accustomed to the fixed routine of the ART centre, which ensured that working PLHIV were able to plan their schedule and get back to work after their appointment at the ART centre. Some (27) participants had previously tried obtaining ART services nearer home but found them “unfriendly”. In 9 cases, the participants felt that they did not want to “tell their story all over again” to a new team of ART staff.
“I have been taking ART for the past 4 years. Once in every two months, I travel 12 hours from Rajasthan in my truck to Surat and collect medicines for next 2 or sometimes 3 months. I was diagnosed here. I tried to get medicines in a hospital nearer home. They asked for paperwork and were not cooperative at all. I cannot adjust to that environment. So I decided to come here. I plan so that when I come here I also do some other business related work. Even during the lockdown, I had pills enough for 2 months. I did not miss the pills even a single day”—P63 (45 year old PLHIV from Rajasthan)
In the semi qualitative interviews, PLHIV reported that it was “difficult” to get ART from ART centres of some other States on a temporary basis, as in case of an emergency, because of different work policies in those States. This belief was rooted in their previous experiences, which discouraged them from approaching the peripheral centres or ART centres in their hometown for a refill or MMD during the pandemic.
“The last time I went to my village, I had been to the (ART) centre there. They said they cannot give me ART without transfer certificate from here. I told them that I would be staying only for 2 months or so. They told me that they could give me (ART) for only 15 days. I have to travel nearly 45 km to reach this place. How would I do it every 15 days? So this time, I sought the help of our Sarpanch (village head) to negotiate with them. Staff from here also had called them. I got ART for 2 months together”—P30 (50 year old PLHIV)
Poor utilization of social support schemes
The average monthly per capita income of the 250 PLHIV interviewed declined from Rs.4667 (62 USD) before lockdown to Rs.1474 (19.7 USD) during lockdown (Figure 3). However, only 8 of the 45 participants eligible for social support schemes of the Government, such as use of Ration card in Public Distribution System for food grains and other commodities were actually availing it. This was despite 17 participants possessing a BPL Ration card. Other eligible participants (28) did not possess a ration card. Similarly, only three of the eleven widows interviewed were getting widow pension. Almost all the participants (238) had a personal bank account. The most common reason cited by the PLHIV for not possessing a Ration card or other social support schemes, despite being eligible for it was the lengthy procedure involved in enrolling for such schemes. The other issues included the lack of adequate information regarding the eligibility and need of middlemen to complete procedures. Such PLHIV also faced exploitation in the course of availing these services.

Average monthly per capita income before and during lockdown (in Rs.), in participants of different socioeconomic status (based on modified B.G Prasad classification 15 ).
Use of Technology
Updated, computerized data
Availability of updated, computerized information at the ART centre of the PLHIV, including contact details made data retrieval for contacting the PLHIV easy and efficient.
“Even before the pandemic, when the patients came to collect ART, we would not only dispense drugs, but also ask them regarding any changes in their address and phone number. This was a regular activity, especially for with those a temporary address. We would also build a rapport with the patients in such a way that they would report any changes themselves.”—IDI3 (ART centre staff)
Availability of pan-India digital platform
NACP has introduced IT-enabled platforms such as SOCH (Strengthening Overall Care for HIV-patients), that enables migrated PLHIV to get ART anywhere in the country, even without any paperwork.
“We have provided drugs to many patients like that. Patients came with practically no record of treatment so far—just stating that they are on ART. We have been able to retrieve the data using SOCH platform and provide them ART. Another advantage of this platform is that when the drugs are dispensed using SOCH platform, the home ART centre would get the notification that this patient has received ART from somewhere else. So this saves a lot of manual tracking.”—IDI1 (ART centre staff)
However, two major challenges were noted here. Firstly, the use of IT platforms was not uniform across different centres. Hence, it was reported in the IDI that, in some cases, PLHIV who had migrated to other districts or states had received ART at other centres without being the reporting through the IT platforms. Thus, these patients were considered as “missed” till they reported back. Secondly, despite digitalization of the ART centre, the peripheral centres continued to manually report the data to the ART centre, which had to be later computerized at the ART centre.
Service Delivery
Uninterrupted supply of ART
Throughout the COVID-19 pandemic, there was no disruption of supply of ART, and prophylactic drugs. The ART centre continued to maintain stocks enough for 2.5 months, thus enabling them to cater to the newly migrated PLHIV as well. The stocks were routinely monitored by the GSACS.
PLHIV “missed” on treatment
According to the desk review of data, about 4–6% PLHIV “missed” the ART every month in 2018–2019. Immediately before the lockdown (March 2020), the number of person “missed on ART” increased to 7%. During the two months of lockdown, there were 5750 PLHIV alive and on ART, of whom 11% (April) and 6% (May) “missed” ART (respectively). The percentage of persons “missed” remained 7% and above till September 2020, when it dropped back to 5%
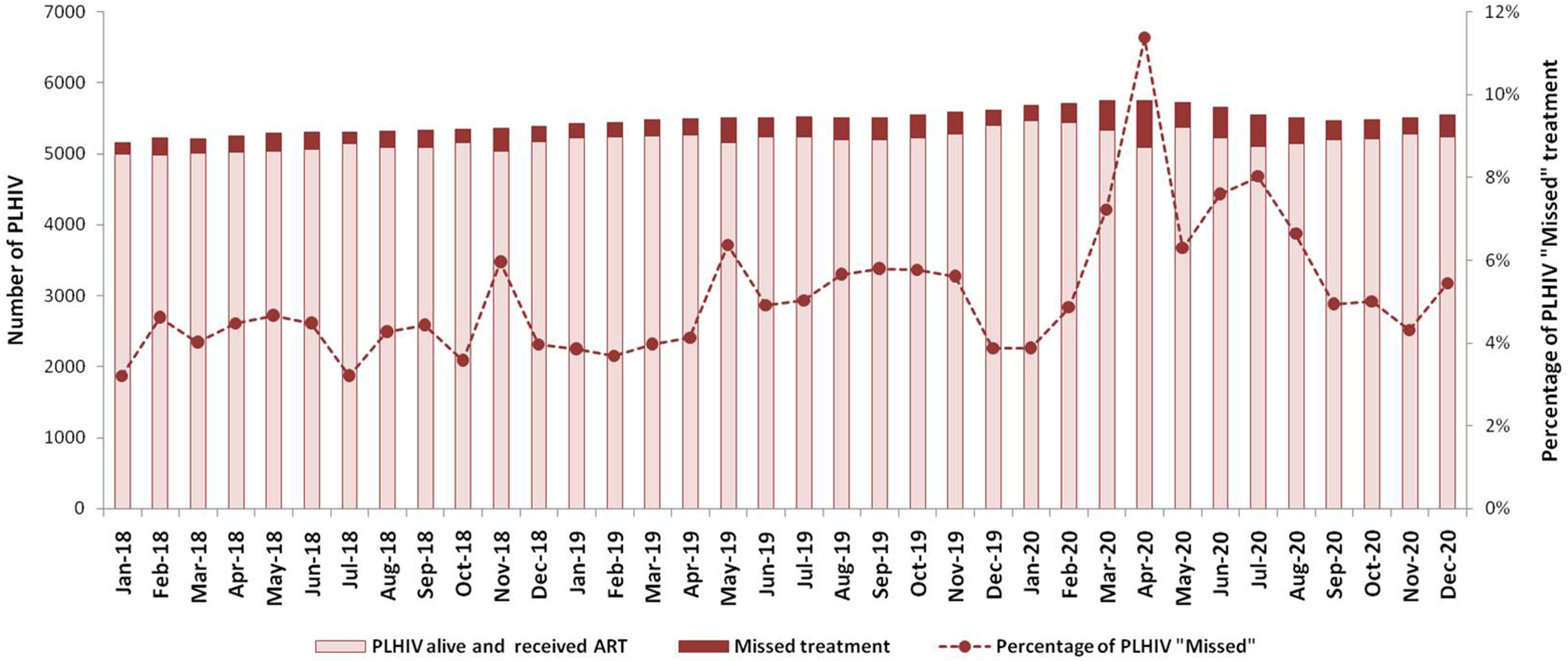
PLHIV “missed” on ART during COVID-19 lockdown in 2020, compared to 2018-2019.
Low TB case detection rate
The number of PLHIV attending the ART centre every month ranged between 2928-4157 in 2019. There was a reduction in the average number of ART centre attendees to 2296 during and after lockdown.
Symptom (4S) screening for Tuberculosis (TB) was routinely carried out in all the PLHIV attending the Centre. Among all the PLHIV who came to the ART centre, about 5% were tested and about 0.5% were diagnosed with TB using diagnostic tests every month.
During the two months of lockdown, less than 2400 PLHIV attended the ART centre every month, of whom only less than 1% was tested for TB using a diagnostic test and less than 0.5% was detected with TB. In two months of lockdown (April-May 2020), a total of 10 new cases of TB were detected, as opposed to 10–30 cases every month before lockdown. The percentage of PLHIV tested remained less than 3% till August 2020, after which the percentage increased to pre lockdown levels. The percentage of PLHIV detected with TB showed a slight increase 3 months after the lockdown (from September 2020 onwards) though the absolute numbers remain low (less than 10) (Figure 5).

PLHIV attending ART centre, tested for and detected with TB.
Treatment adherence
Among all the PLHIV attending the ART centre, during the years prior to lockdown (2018-19) and during lockdown, 86–87% had Good adherence (>95% adherence) to treatment, while 10–11% had average adherence (80-95%) adherence. However, among the PLHIV assessed for adherence between August and December 2020, the percentage of PLHIV with Good adherence dropped to 80%, while the percentage with Average and Poor adherence was 12% and 8% respectively. This paradoxical dip in adherence in the post lockdown period is due to the reporting method, wherein the PLHIV attending the ART centre in a particular month are always assessed for adherence in the months immediately preceding it. Hence, the low adherence reported in August-December 2020 correspond to months preceding it ie, during and immediately after lockdown (April-July 2020).
Among the 250 PLHIV interviewed in this study, average 6 month adherence prior to the lockdown and during lockdown were recorded. There was a small but significant decline in overall adherence to ART from an average of 98.8% to 96.2% during lockdown (t = 3.528, df = 249, p = 0.000). The six month adherence of participants availing ART services from different ART providers (through MMD from parent ART centre, other peripheral centres and those who “missed” ART for a period of time during the lockdown) were estimated separately (Table 3).
ART Provider During Lockdown and Comparison of Adherence to ART Before and During Lockdown.

CD4 count measured in the months prior to lockdown (within 3 months prior to lockdown) and measured immediately after “Unlock” (within 3 months of unlocking) were compared. Post lockdown CD4 count was not available in 61 participants.
Overall, CD4 count showed no significant difference before (508 ± 246 SD) and after lockdown (511 ± 246 SD), (t = −0.365, df = 188, p = 0.715). Among participants who had missed ART for varying periods of time during lockdown, the mean CD4 count dropped from 431 to 416 cells/cumm, though this was not statistically significant (t = 0.705, df = 11, p = 0.495). Among participants who had taken ART from peripheral centres, the mean CD4 count before (542 cells/cumm) and after (573 cells/cumm) lockdown did not differ significantly (t = −0.707, df = 17, p = 0.489). Similarly among those who had received ART as Multi-month dispensation from ART centre, the mean CD4 count before (509 cells/cumm) and after (511 cells/cumm) lockdown did not differ significantly (t = −0.185, df = 158, p = 0.854), (Figure 6). However, this analysis is applicable only to the PLHIV interviewed

Cd4 count before lockdown and after unlock (N = 189), in PLHIV who availed ART at different centres.
Interrupted laboratory services and delayed detection of virological failure
Routine laboratory services were hampered, during the lockdown. The laboratory technicians had been diverted to COVID-19 related lab work and the number of PLHIV attending the ART centre was also low, because of MMD, Community dispensation of ART, “Missed” PLHIV and migration. In 2018 and 2019, the number of PLHIV undergoing CD4 count estimation was 918 per month, on an average. During lockdown, the number of samples collected per month for CD4 count estimation was, on an average, 10 per month. This increased to an average of 583 per month after June 2020. Similarly, increasing number of PLHIV were being offered Viral load estimation, with an average of 498 samples collected per month in January–March 2020. However, samples were not collected in April-May 2020 (during lockdown). Viral load estimations were restarted in July 2020, and as many as 610 samples were collected every month on an average (Figure 7).
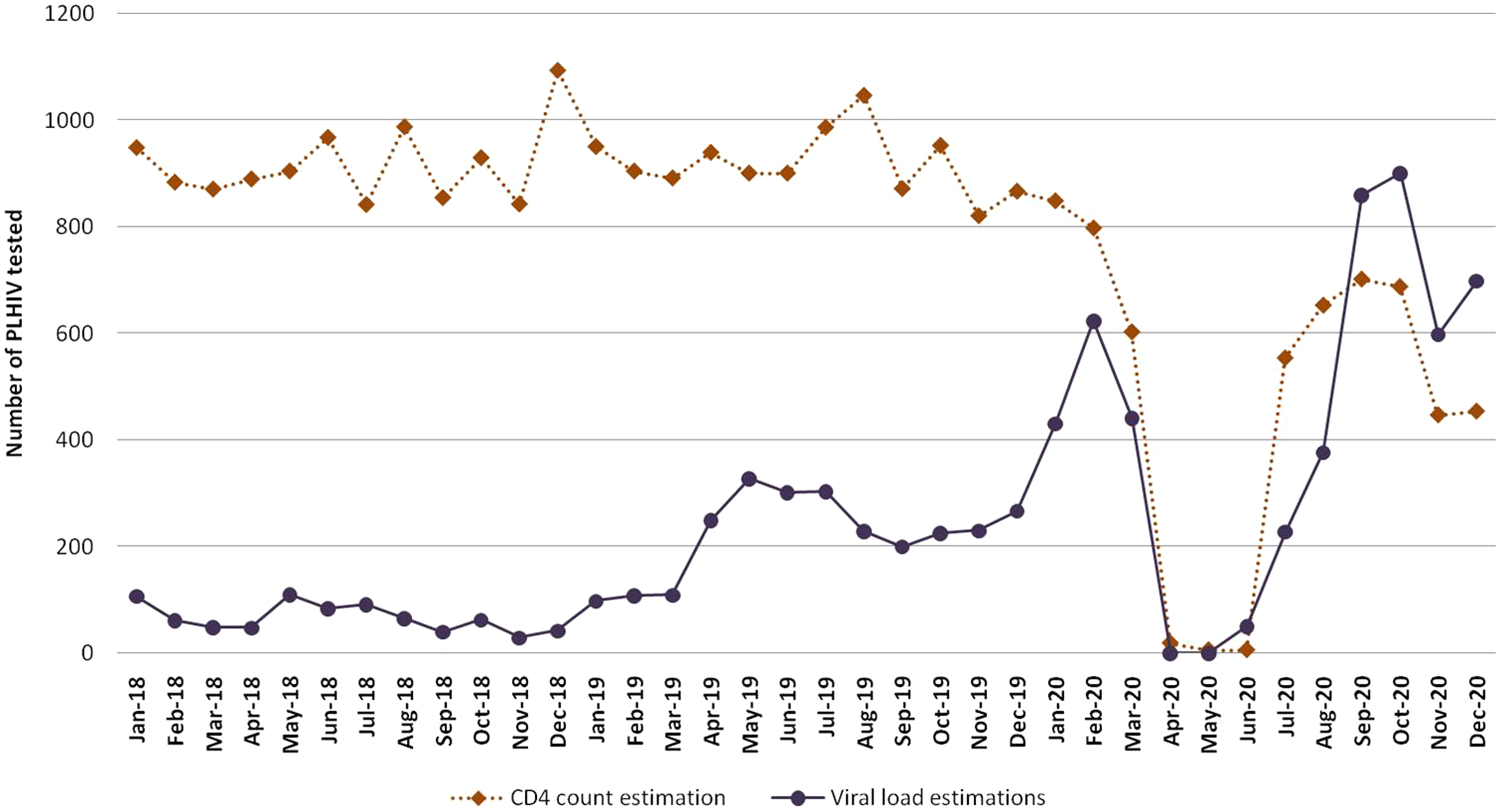
Cd4 count and viral load estimation per month (2018-2020).
A total of 74 PLHIV were started on second line ART in post lockdown period (average 10 per month) between June-December 2020. This was comparable to 2019, where on an average, 9 PLHIV were started on second line ART every month. However delayed testing led to delay in second line initiation, resulting in higher enrollment in the initial months of Unlock phase.
Discussion
COVID-19 is one of the largest pandemics in the history of modern medicine. Apart from the millions of deaths it caused worldwide, the pandemic has been able to shake the foundations of countries, by their challenging the health care systems and economic structures. It was naturally anticipated that the COVID-19, especially the periods of lockdown, would stall and even reverse the years of progress achieved in health care in countries, including India. In this study, we studied the impact of COVID-19 lockdown (2020) on the care and support of people living with HIV, in urban South Gujarat. The backdrop of this study was the nationwide lockdown due to COVID-19 pandemic, between 24th March 2020 and 31st May 2020, which was followed by phased “Unlock”. Under NACP guidance, the ART centre in this study setting had started Multi- Months Dispensation (MMD) and Community dispensation of ART.
At the outset, one of the major achievements of the ART centre in COVID-19 lockdown, was that it remained functional throughout the lockdown period and catered 5750 PLHIV (directly or indirectly), including new and transfer-in PLHIV. In a study involving 19 countries of Europe, in March 2020, the authors reported that while there were no HIV clinic closures, only 6 countries reported that HIV clinics were “operating normally”. 16 In the ART centre in this study, the internal organization of the ART centre staff, with division of work among all the available staff was a key administrative step towards uncomplicated process and accountability of work. Another favorable condition of the ART centre studied was that the staff members were not given duties in both HIV clinic and COVID care simultaneously, unlike in other studies. 16 The staff members coordinated with the peripheral health centres, TI/CBO, Care and Support Centres or other ART centres to ensure continuum in care. On the other hand, the process was laborious and required extra time and effort of the staff involved. Multiple phone calls had to be made to different stakeholders and PLHIV. Apart from ART dispensed through the other centres or partners, about 40% (more than 2000 per month) PLHIV continued to visit the ART centre for MMD. The unstable PLHIV receiving MMD had to be given “additional counseling”. The diversion of staff to COVID duties of the hospital was a setback in terms of man power. The staff also reported having experienced “burnout”. Several studies have reported exhaustion and burnout among frontline healthcare workers during COVID-19, and recommend adjusting work shifts and workload assessment to deal with such situations. 17 Similarly, exhaustion and burnout among health care workers providing non-COVID services during the pandemic needs to be addressed.
The ART dispensation to PLHIV who could not reach the ART centre was achieved by systematically coordinating with peripheral health centres of the District, communicating effectively with the HIV Care and Support Centres, TI/CBO for Community Dispensation of ART to the PLHIV residing in the city and facilitating the linkage of migrated PLHIV to ART centres across the State of Gujarat and other States as well. The well established network of the TI/CBO and other HIV care and support partners (CSO, PLHIV network) with the ART centre, which is routinely involved in tracking and linking “Missed” or “Lost to Follow Up” PLHIV proved useful during COVID lockdown also. However, in some instances, dependence of PLHIV on the TI/CBO was found, which might adversely impact the system in the long run. The success of Out of Facility Individual model of Differentiated Care for HIV is based upon the availability and efficiency of lay cadres, comprising of outreach workers and volunteers. 11
One major challenge was dealing with unplanned migration and ensuring continuum of care in them. The percentage of PLHIV reported “Missed” peaked in April 2020% to 11%. Studies have highlighted the plight of migrant workers due to the lockdown measures and unavailability of ART.18,19
Despite the good coordination with the ART centres of other states, the different working policies of different States warranted rounds of negotiation. On the other hand, it was reassuring to note that 63% of the PLHIV interviewed knew how to contact the ART centre in case of emergencies. Awareness among the PLHIV regarding the availability of ART in other centres and regarding basic operational aspects of ART centre, such as the ART number and whom to contact for assistance, were beneficial, because in such cases PLHIV took a lead themselves to contact the ART centre and remain in the continuum of care.
Despite being in contact with the ART centre, PLHIV were found to miss on ART for other reasons, such as fear of disclosure and fear of COVID-19 among the PLHIV which had to be addressed in a client specific manner. Several authors have reported or raised concerns about the fear of contracting COVID-19 as a barrier among people to avail ART services in hospitals.19,20 In this study, we found that the fear of COVID-19 and fear of inadvertent disclosure could be successfully addressed through repeated counseling and client specific planning of ART delivery.
The general acceptance of MMD was good, with most of the PLHIV mentioning how it saved time and money by reducing the frequency of visits to the hospital. The Community Dispensation of ART and provision of ART through peripheral health centres was perceived generally as a “temporary arrangement” to tide over COVID crisis. It was noted that mutli- months dispensation through the same ART centre was preferred, where as the choice of ART centre largely depended on a number of factors such as confidentiality, discretion, availability of other medical services and availability of dedicated services to PLHIV. Hence, any decision to decentralize the HIV care services to PHC/CHC or sub district levels must also address these factors.
Computerization of data helped in easy retrieval of data to prepare the beneficiary lists, sharing of data and reporting. However, the ART dispensation through peripheral centres and TI/CBO involved collection of data manually and then computerizing them at the ART centre. The availability of IT based platforms such as SOCH made tracking of PLHIV to other ART centres and reporting easier. Moreover, State to State non uniformity in utilization of digital platforms led to several migrant PLHIV being reported as “Missed” even when they had actually availed ART elsewhere. Hence the percentage of PLHIV who had “Missed” ART tends to be lower than 11% reported.
There was an uninterrupted supply of ART throughout the lockdown period that was enough to provide MMD to those registered in HIV care in the ART centre and also to those who migrated/transferred in during the lockdown. Interruption of ART supply would have proven disastrous, even though it is unclear whether the extent of its impact in India would have been as severe as suggested by the modeling study in Africa which estimated that even a three-month disruption of ART supply would lead to half a million excessive HIV/AIDS related deaths in Africa alone. 21
Disruption of TB-HIV services, including new case detection was a major concern during lockdown. 22 In our study, it was found that screening and testing PLHIV for Tuberculosis was affected, because the turnout in the ART centre was low and continued to remain low after “Unlock”. There was no rebound increase in the monthly average number of TB cases reported in the “Unlock phase”. Given that less number of PLHIV are attending the centre even after Unlock, it is yet to be ascertained whether the low number of new cases signifies the presence of hidden, undetected cases or the low transmission during COVID-19 lockdown. Modeling studies suggest that “accumulation of undetected cases is a principal driver” of at least a million additional new cases of TB in the country and how a “catch up” TB detection should be adopted as soon as the lockdown eases. 23
Desk review of data suggested that there was no increase in average number of patients shifted to Second Line ART in the 6 months following lockdown, though the adherence to treatment had declined overall. However, the enrollment on Second line ART was higher in the initial months of Unlock phase, suggesting that there was delay in detection of PLHIV who were in treatment failure. This is attributable to the disruption in lab services (CD4 count and Viral load estimation) during lockdown. Hence available data suggests that COVID-19 lockdown did not primarily result in treatment failure, but resulted in delayed the recognition of treatment failure. In this context, the limitation of this study is that it does not include the data from those who were lost to follow up or died. A study from South Africa also reported that while ART provision was maintained in 65 primary health care centres studied, new detection and ART initiation had been “severely impacted”. 24
Conclusion and Recommendations
Despite the initial anticipation and setbacks, ART delivery through MMD and Community Dispensation to PLHIV continued satisfactorily during the COVID-19 lockdown, although not without challenges, such as disruption in laboratory services. The HIV Care and Support system needs to be strengthened at the levels of various of stakeholders by:
This study has documented several good practices that helped in implementing MMD and Community Dispensation of ART. COVID-19 experience must be used for strengthening the NACP to be prepared for emergency response to different contexts, such as pandemics, natural disasters and man-made conflicts.
Footnotes
We are grateful to the Gujarat State Health System Resource Centre (SHSRC), under the Health and Family Welfare Department, Government of Gujarat, for the financial support, reviewing the study protocol and providing valuable inputs. We thank Dr Rajesh Gopal, Additional Project Director and his team at Gujarat State AIDS Control Society (GSACS) for permitting this study in ART centre, Government Medical College, Surat. We thank the Nodal Officer and staff of ART centre, Government Medical College, Surat for facilitating the study. We thank all the Project Staff of PARAS PSM Unit II, PARAS PSM Unit III, Sahyog and Ekta Mahila Mandal who enriched the study findings with their inputs. We thank all the PLHIV whose experiences and perspectives shaped our vision of future of HIV care.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This project was funded by Gujarat State Health System Resource Centre (SHSRC), Health and Family Welfare Department, Government of Gujarat [No. SHSRC/OR/1614-17/2021], India.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Gujarat State Health System Resource Centre (SHSRC), under the Health and Family Welfare Department, Government of Gujarat, (grant number No. SHSRC/OR/1614-17/2021).