
Abstract
Background
Differentiated service delivery models (DSDMs) are client-centered approaches to HIV care that improve efficiency through simplification, task shifting, and decentralization. However, utilization of Ethiopia's community-based DSDM remains low, and its determinants are not well understood.
Objective
To assess the utilization of and factors associated with community-based DSDM among ART users in Dessie public health facilities, Northeast Ethiopia, 2025.
Methods
A convergent mixed-methods cross-sectional study was conducted among 635 randomly selected ART users. Quantitative data were collected using interviewer-administered questionnaires and analyzed using multivariable logistic regression in STATA 16. In-depth interviews with purposively selected ART users were analyzed thematically to explore contextual barriers and facilitators.
Results
Overall, 17.1% (95% CI: 14.3-20.3%) utilized community-based DSDM. Utilization was positively associated with primary education, HIV status disclosure, and ART regimen change, but negatively associated with prior loss to follow-up and baseline CD4 ≥ 500 cells/mm3. Qualitative findings highlighted information gaps, stigma, and misconceptions as barriers, while peer support facilitated uptake.
Conclusion
Community-based DSDM utilization remains suboptimal, underscoring the need for strengthened counseling, stigma reduction, and targeted patient education to enhance uptake.
Plain Language Summary Title
Plain Language Summary
In Ethiopia, people living with HIV receive care through Differentiated Service Delivery Models (DSDMs), an approach that includes several ways of providing HIV services. These models can be facility-based or community-based, depending on patients’ needs and preferences. One option is a community-based model, which aims to make HIV treatment more convenient by offering services closer to where people live and by reducing the need for frequent clinic visits. Despite these advantages, use of the community-based option remains low, and the reasons are not well understood.
This study examined how many HIV patients in Dessie use the community-based DSDM and what factors influence their decision. Researchers surveyed 635 people receiving antiretroviral therapy (ART) at public health facilities and found that only 17 out of every 100 patients were using the community-based option.
Use of the community-based model was more common among people with primary education and those who had disclosed their HIV status, but less common among patients with a history of stopping treatment or with higher CD4 counts. Interviews showed that limited information and fear of stigma were major barriers.
The findings suggest that increasing awareness, reducing stigma, and improving access could help more people benefit from community-based HIV care.
Keywords
Introduction
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) remain major public health challenges globally. In 2024, an estimated 40.8 million people were living with HIV worldwide, with sub-Saharan Africa continuing to shoulder a disproportionate share of the global burden. 1 Although no cure currently exists, HIV can be effectively managed through lifelong Antiretroviral Therapy (ART), which suppresses viral load to undetectable levels, reduces morbidity and mortality, and prevents onward transmission. 2
To improve the efficiency and accessibility of HIV care, many countries have begun shifting from conventional, facility-based models to more client-centered and decentralized approaches. One such approach is Differentiated Service Delivery Models (DSDMs)-a strategy designed to tailor HIV services to the clinical needs, preferences, and Contexts Of People Living with HIV (PLHIV) while maintaining equity and quality of care.3,4 Community-based DSDMs in Ethiopia include interventions such as Community ART Refill Groups (CARGs), Community Drug Distribution Points (CDDPs), and outreach ART refill services. These models are designed to reduce facility congestion, lower patient costs, and improve retention in care. A distinctive feature in Ethiopia is that community-based ART groups are often facilitated by trained peer leaders, which helps strengthen peer support and reduce stigma, especially in urban settings like Dessie City. 5
Globally, the expansion of DSDMs aligns with the UNAIDS 95-95-95 targets ensuring that 95% of PLHIV know their status, 95% of those diagnosed receive ART, and 95% of those on ART achieve viral suppression by 2025. 6 Achieving these ambitious goals requires health systems to adopt innovative service delivery approaches that optimize resources, particularly in settings with constrained healthcare workforce and infrastructure.
Despite global progress in scaling up ART, HIV/AIDS remains a significant health burden. In Ethiopia, HIV prevalence is estimated at 0.9%, yet certain urban areas including Dessie City report substantially higher prevalence, reaching 8.5%, with ART treatment failure rates up to 15.9%.2,7–9 Although ART has transformed HIV into a manageable chronic condition, the growing number of stable patients has placed pressure on health facilities, reinforcing the need for decentralized and differentiated service delivery.4,10
Although Ethiopia has adopted WHO recommendations to scale up community-based DSDMs, their implementation and uptake remain limited. Evidence shows that many ART clients continue to prefer facility-based services because of perceived higher quality of care, stronger relationships with healthcare providers, and more flexible service hours.10–13 Furthermore, little is known about the determinants influencing the low utilization of community-based DSDMs among ART users in Ethiopia.
Importantly, quantitative data alone cannot fully explain the underlying reasons for low DSDM utilization such as stigma, misconceptions about community ART delivery, privacy concerns, or accessibility constraints. Thus, a mixed-methods approach is essential to capture both the measurable determinants and the contextual, experiential, and sociocultural factors that shape client decision-making. Integrating quantitative and qualitative evidence strengthens the explanatory power of the study and provides a more holistic understanding of DSDM utilization.
Therefore, this study aims to assess the determinants of community-based DSDM utilization among ART clients at public health facilities in Dessie City, Northeast Ethiopia, using a mixed-methods approach.
Methods and Materials
Study Design and Setting
The study was conducted at public health facilities providing ART follow-up services in Dessie city from December 15, 2024, to February 15, 2025. Dessie city is located approximately 401 kilometers north of Addis Ababa, the capital of Ethiopia, and serves as the administrative center of the South Wollo Zone in the Amhara Region. According to the 2023 population projection, the city has an estimated total population of about 328,016. Currently, five public health facilities in Dessie City provide ART services to PLHIV (23). A convergent mixed-methods cross-sectional study was employed to assess the determinants of community-based DSDMs among ART users in these facilities.
Source and Study Population
The source population consisted of all adult clients receiving ART at public health facilities in Dessie City, while the study population included adult ART users aged 18 years and above who had been on ART for at least 12 months in the selected health facilities.
Sample Size Determination and Sampling Procedure
The sample size for this study was determined using a single population proportion formula, assuming a 50% proportion (as a rule of thumb, due to the absence of prior similar studies), a 95% confidence level, and a 5% margin of error. The formula used was:

where:
n = required sample size, Zα/2 = 1.96 (Z-value for 95% confidence interval), P = 0.5 (assumed proportion), and D = 0.05 (margin of error).

Substituting these values yielded an initial sample size of 385. After adding a 10% non-response rate and applying a design effect of 1.5 to account for the multistage sampling approach, the final sample size was 635 participants.
For the qualitative component, the number of participants was determined based on the principle of data saturation, which was achieved after conducting in-depth interviews with eight purposively selected ART users. Although the sample size is relatively small for exploring complex barriers such as stigma, misconceptions, and cultural beliefs, participants were deliberately selected for their direct experience with CAG utilization, ensuring the collection of rich and relevant information. Participants were identified and recommended by ART focal nurses and community volunteers based on their knowledge and experience with ART services.
The study employed a convergent mixed-methods approach, in which quantitative and qualitative data were collected during the same study period, analyzed separately, and integrated at the interpretation stage. The qualitative findings were used to complement and explain the quantitative results by providing deeper insight into clients’ perceptions, experiences, and barriers related to CAG participation. The study focused exclusively on ART users rather than healthcare providers because the primary objective was to explore client-level perspectives; provider-related factors were considered beyond the scope of this study and are recommended for future research.
Study Variables and Measurements
The dependent variable of this study was the utilization of community-based DSDM models among ART users. For clarity, in this study, DSDM specifically refers to the CAG model, which is one of the major forms of community-based DSDMs. Although other models of differentiated ART delivery exist, only participation in a CAG was assessed. Utilization was defined as being documented by a healthcare provider as a member of a CAG. Participants were asked, “Are you a member of a CAG?” Those who responded “Yes” were coded as 1 (utilized the CAG model), and those who responded “No” were coded as 0 (did not utilize the CAG model).4,14
The independent variables included three major categories:
Sociodemographic characteristics: age, sex, residence, marital status, educational status, occupation, and monthly income.
Behavioral and facility-related factors: number of sexual partners, condom use, alcohol consumption, khat chewing, type of health facility, and distance from the clinic.
Clinical and treatment-related factors: level of ART adherence, history of LTFU, recent viral load result, ART regimen change, duration on ART, baseline CD4 count, missed clinical appointments, and HIV status disclosure.
Stable Clients were defined according to the 2016 WHO guidelines as individuals who had been on ART for at least 12 months and had a most recent viral load of <1000 copies/mL. In the absence of viral load testing, a CD4 count >200 cells/mm3 was used as a proxy for clinical stability.15,16
A missed clinical appointment was defined as failure to attend a scheduled clinic visit more than 5 to 7 days after the planned date.17,18
Data Collection Tools and Procedures
A pre-tested structured checklist was developed in English, adapted from various relevant literature sources.14,17 The checklist was reviewed for content validity by subject-matter experts in HIV care and public health. While no previously validated tool was available that fully matched the study objectives, the checklist was pilot-tested among a small group of ART users (n = 32) at Kombolcha 03 health center to ensure clarity, relevance, and feasibility prior to full-scale data collection. Data were collected electronically using the Kobo Toolbox platform, accessed via mobile phones or laptops at selected health facilities. The checklist was translated into Amharic to ensure cultural appropriateness and comprehension for participants. Prior to data collection, selected participants were asked for their informed consent and willingness to participate in the study.
The questionnaire was contextualized to include detailed information from ART follow-up records and intake forms. It covered a wide range of variables, including sociodemographic, personal, and clinical factors. The calculated sample size was 635 ART users, selected by simple random sampling from a total of 920 registered ART users. Data were collected using the structured checklist.
For the qualitative component, a semi-structured interview guide was developed in English and translated into Amharic. The guide was informed by literature related to the study's core research questions and was designed to elicit in-depth responses through probing. It aimed to capture participants’ perspectives on the utilization of community-based DSD models, with suggested prompts to guide the interviews. 19 The interview guide was reviewed by experts for face validity and pilot-tested with a small subset of participants to refine question wording and flow.
The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement (von Elm et al, 2007) [SUPPLEMENTARY FILE: STROBE_checklist_v4_combined]. The completed checklist is provided as a supplementary file to ensure transparency and adherence to the EQUATOR Network guidelines.
Data Quality Assurance
To ensure the quality of the data collected, a standardized and pre-tested structured checklist developed in English and adapted from relevant literature was utilized.2,20–22 The checklist was pretested on a sample of participants outside the study area, and its content validity was assessed by a panel of subject matter experts. Feedback from the pretest and expert review was used to refine ambiguous items and ensure cultural appropriateness. Reliability was assessed using Cronbach's alpha for internal consistency, and the checklist demonstrated acceptable levels of both validity and reliability.
Data collectors received two days of training on the data collection tools and procedures, including topics such as confidentiality, ethical conduct, and appropriate data collection techniques. During data collection, the principal investigator reviewed completed questionnaires daily to ensure completeness and consistency. Data were entered using Kobo Toolbox software, which helped minimize data entry errors. The research team maintained regular communication with data collectors, providing timely support and clarification to address any uncertainties or procedural issues.
For the qualitative component, the interview guides were reviewed by subject matter experts to ensure content quality and cultural appropriateness. A pilot test was conducted to assess the logical flow and sensitivity of the questions. Interviews were conducted using simple and clear language, employing semi-structured guides with probing questions to elicit detailed responses. An external audit was also conducted to verify the accuracy of the findings and ensure that conclusions were grounded in the collected data.
Data Processing and Analysis
Quantitative data were entered into Kobo Toolbox software to minimize data entry errors. The data were carefully edited and cleaned before being exported to STATA version 16 for analysis. Descriptive statistics were used to summarize the background characteristics of respondents and to assess the utilization of CAGs.
A logistic regression model was fitted to identify factors associated with CAG model utilization. Variables with a p-value < 0.25 in the bivariate analysis were included in the multivariable logistic regression model. Statistical significance was determined at a p-value < 0.05. The goodness-of-fit of the model was assessed, and the model was considered a good fit if the test result was not significant (p-value > 0.05). Additionally, multicollinearity among independent variables was checked using the Variance Inflation Factor (VIF), with a mean VIF of 1.93, indicating no significant multicollinearity.
For the qualitative component, audio-recorded interviews were first transcribed in Amharic and then translated into English. The transcripts were edited, formatted, and saved in text files. These were imported into Open Code software version 4.02 for analysis. Relevant segments of the text were coded, and the codes were grouped into themes such as:
Understanding of DSDM Perceptions toward DSDM Concerns about DSDM
Finally, triangulation was conducted by comparing and integrating findings from both the quantitative and qualitative data to enhance the validity and depth of the study results.
Ethics Declarations
This study was conducted following ethical approval obtained from the Research and Ethics Committee of Wollo University, College of Medicine and Health Sciences (Approval No: WU-REC-CMHS/1415/13/17), dated 05/05/2017 (Ethiopian Calendar). In addition, a formal permission letter was secured from the Dessie City Health Administration Office and the respective selected public health facilities prior to data collection.
All data collected from participants were used solely for research purposes. Participants were informed about the objectives of the study, and their voluntary participation was ensured. Written informed consent was obtained from all participants before enrollment. Confidentiality and anonymity were strictly maintained throughout the data collection and analysis processes.
Results
Characteristics of Study Participants
A total of 615 respondents were included in the study. The mean age of participants was 40.90 years (SD ± 8.12). The majority of respondents were above 35 years old, 417 (67.80%), followed by those aged 25–35 years, 159 (25.85%). Regarding educational status, 166 respondents (26.99%) were unable to read and write. In terms of residence, 483 participants (78.54%) were from urban areas, while 132 (21.46%) were from rural areas (Table 1).
Socio-Demographic Characteristics among ART Users in Public Health Facilities of Dessie City, Northeast Ethiopia, 2025.

Key: Others = Students, employed, female sex workers.
Clinical, Treatment & Health Service Delivery-Related Factors
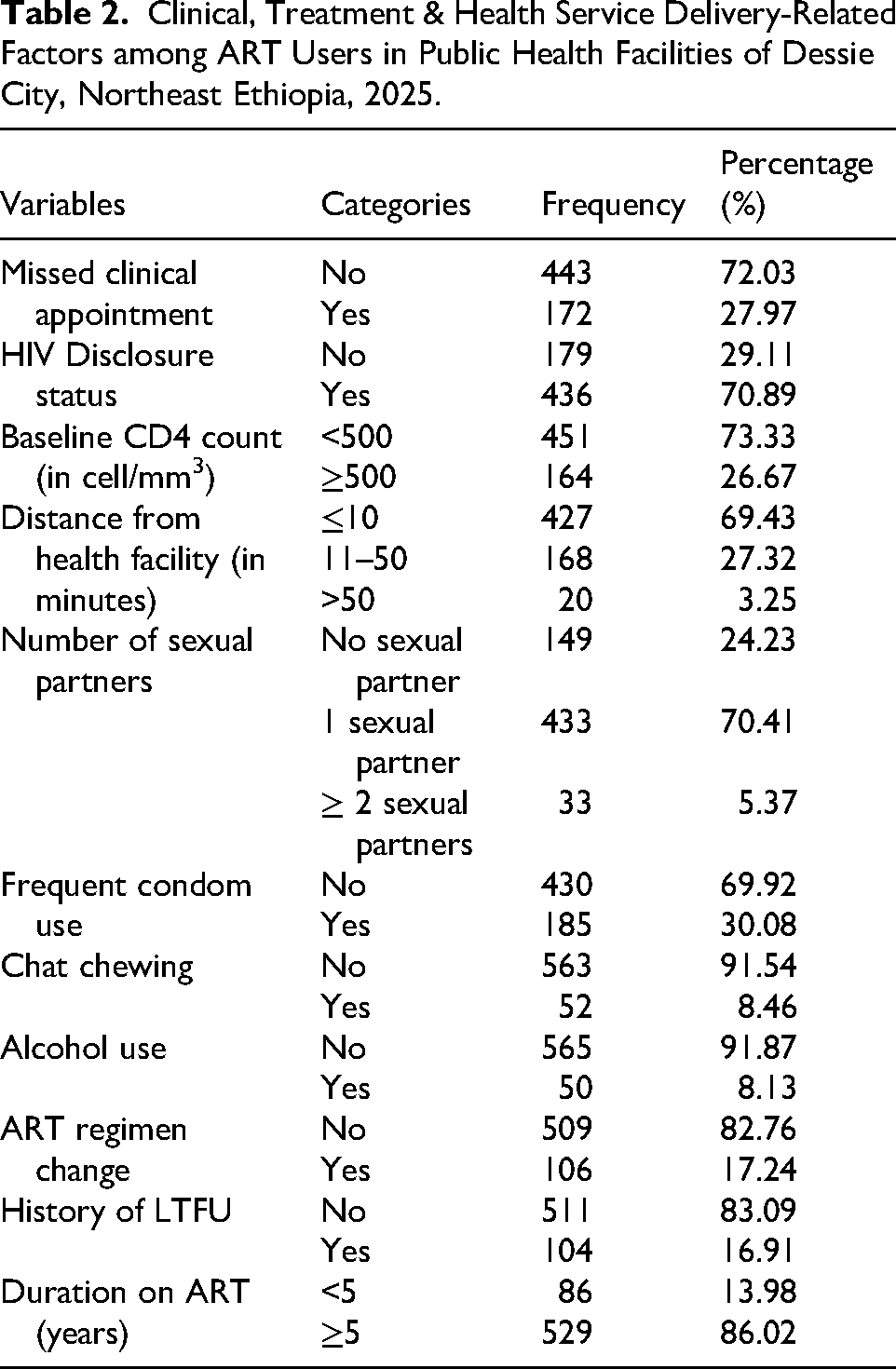
Regarding clinical and treatment-related factors, most respondents 443 (72.03%) did not miss clinical appointments, while 172 (27.97%) reported missing at least one appointment. In terms of baseline CD4 count, 451 participants (73.33%) had counts below 500 cells/mm3, and 164 (26.67%) had counts of 500 or above. The majority of participants 427 (69.43%) lived within 10 min of a health facility, while 168 (27.32%) lived 11 to 50 min away.
Regarding behavioral factors, 185 respondents (30.08%) reported frequent condom use, whereas 430 (69.92%) did not use condoms regularly. Khat chewing was reported by 52 participants (8.46%), and alcohol use by 50 (8.13%). Most participants 509 (82.76%) had not experienced an ART regimen change, while 106 (17.24%) reported a change in their regimen. Concerning duration on ART, 529 respondents (86.02%) had been on treatment for more than 5 years, and 86 (13.98%) had been on ART for less than 5 years (see Table 2).
Clinical, Treatment & Health Service Delivery-Related Factors among ART Users in Public Health Facilities of Dessie City, Northeast Ethiopia, 2025.
Utilization of DSDM Among ART Users
The current study revealed that 105 respondents (17.07%; 95% CI: 14.29%–20.26%) utilized the community-based DSDM. The quantitative findings indicated a low prevalence of community-based DSDM utilization in the study area. This limited uptake was associated with various clinical, treatment, and health service delivery-related factors. To complement these findings, qualitative data provided deeper insights into the underlying barriers.
Lack of Information and Misunderstanding of DSDM
While some ART users demonstrated a basic understanding of DSDM and its role in HIV prevention, many lacked accurate information. For example, one participant mistakenly believed that DSDM was a cure for AIDS and could be given regardless of HIV status: “…Proper DSDM use cures AIDS and it is given regardless of his/her HIV status.” 35-year-old participant
This highlights a critical gap in health education and awareness, which likely contributed to the low utilization of DSDM services.
Misconceptions about DSDM and its effects:
Misunderstandings about the purpose and effects of DSDM were common. Some ART users believed that participating in DSDM could lead to stigma and social isolation: “…DSDM ruins the stigma. I believe that it makes us isolated…” 32-year-old participant
Such misconceptions may stem from inadequate counseling and a lack of culturally sensitive communication in service delivery.
Cultural beliefs and stigma:
Cultural perceptions also played a significant role in hindering DSDM uptake. HIV was often viewed as a divine punishment, and some participants preferred traditional remedies over biomedical approaches: “…In our culture, HIV infection is considered a punishment sent from God… I use ‘tsebel’.” 32-year-old participant
Additionally, stigma surrounding DSDM led to fears of being identified as HIV-positive, discouraging open discussion and access: “…There is a fear that people consider us as already having HIV…” 26-year-old participant
Service delivery challenges:
Participants also expressed concerns about the availability and accessibility of DSDM services. Unlike facility-based ART, DSDM was not available in all areas, limiting its practical use: “…DSDM could provide an additional layer of adherence. But its availability is not nearby everywhere.” 35-year-old participant
In summary, the qualitative findings underscore that the low prevalence of DSDM utilization is not solely due to clinical or logistical issues, but is also deeply influenced by information gaps, misconceptions, and cultural beliefs. Addressing these barriers through targeted health education, community engagement, and culturally sensitive service delivery is essential to improve the uptake and retention of community-based DSDM programs.
Factors Associated with DSDM Utilization
A binary logistic regression analysis was conducted to identify factors associated with the utilization of DSDMs. Variables with a p-value < 0.25 in the bivariate analysis were entered into the multivariable logistic regression model. In the multivariable analysis, several factors remained significantly associated with DSDM utilization at a p-value < 0.05 (Table 3).
Factors Associated with DSDM among ART Users in Public Health Facilities of Dessie City, Northeast Ethiopia, 2025.

Key: *= p-value < 0.05, COR = Crude Odds Ratio, AOR: Adjusted Odds Ratio, CI = Confidence Interval &1= Reference.
Educational level was significantly associated with DSDM utilization. Participants who had completed primary education were more likely to utilize DSDM compared to those who were unable to read and write (AOR = 2.61; 95% CI: 1.17-5.78).
A history of LTFU showed a strong negative association with DSDM utilization. Participants with a previous history of LTFU were significantly less likely to utilize DSDM compared to those without such a history (AOR = 0.26; 95% CI: 0.09-0.72).
Participants who had experienced an ART regimen change were substantially more likely to utilize DSDM than those who had not changed their regimen (AOR = 19.12; 95% CI: 9.55-40.87), indicating a strong and statistically significant association.
Regarding baseline CD4 count, participants with a CD4 count ≥500 cells/mm3 at ART initiation were significantly less likely to utilize DSDM compared to those with a CD4 count <500 cells/mm3 (AOR = 0.33; 95% CI: 0.13-0.85).
HIV status disclosure was positively associated with DSDM utilization. Participants who had disclosed their HIV status were more likely to use DSDM compared to those who had not disclosed (AOR = 1.92; 95% CI: 1.43-4.97).
Participants who had missed clinical appointments were less likely to utilize DSDM compared to those who had not missed appointments; however, this association was borderline statistically significant (AOR = 0.42; 95% CI: 0.18-1.01).
Discussion
The present study found that the utilization of community-based differentiated service delivery models (DSDMs) among ART users was 17.07% (95% CI: 14.29-20.26%) in public health facilities in Dessie. This level of uptake is lower than that reported in South Africa, where utilization ranges from approximately 20% to over 50% in some settings, 23 such variation may be attributed to differences in program maturity, eligibility criteria, intensity of provider-led referral, and patient preferences for facility-based care. The relatively low uptake observed in this study highlights persistent implementation, demand-side, and health-system barriers to the expansion of community-based DSDMs in similar resource-limited settings. 20
Educational status was positively associated with DSDM utilization, with participants who had primary education being more likely to engage in community-based models. This finding underscores the importance of basic literacy in understanding eligibility requirements, service modalities, and the benefits of differentiated care, consistent with previous studies. 24 Strengthening health literacy through simplified counseling tools and patient-centered communication may therefore improve informed decision-making and increase DSDM uptake.
A history of LTFU was strongly and negatively associated with DSDM utilization. Patients with prior interruptions in care may experience persistent stigma, mistrust of the health system, or psychosocial vulnerabilities that limit their willingness or eligibility to participate in community-based ART delivery. Moreover, current DSDM eligibility criteria often prioritize clients with demonstrated adherence, potentially excluding those with prior LTFU. This finding highlights the need for targeted re-engagement and adherence support interventions to reintegrate this high-risk group into differentiated service models.
Notably, ART regimen change was strongly associated with higher utilization of community-based DSDMs. Patients who experienced regimen changes were substantially more likely to enroll in community-based services. This association may reflect intensified clinical follow-up, adherence counseling, and provider–patient interaction during regimen transition, which can increase awareness and referral to DSDM options. In addition, clinicians may preferentially recommend community-based models to patients who have successfully stabilized on a new regimen to support long-term adherence and continuity of care. This finding emphasizes the critical role of provider-driven referral practices and clinical decision-making in shaping access to DSDMs.
Participants with a baseline CD4 count ≥500 cells/mm3 were less likely to utilize community-based DSDMs. While this finding may appear counterintuitive given that DSDMs are designed for clinically stable patients it likely reflects provider-side and system-level barriers rather than patient-driven perceptions of reduced need. Clinicians may be less proactive in referring immunologically stable patients to community-based services due to conservative interpretations of eligibility criteria, concerns about reduced clinical oversight, or entrenched facility-centered care practices. Additionally, programmatic guidance may inadvertently prioritize retaining stable patients in facility-based care rather than actively transitioning them to community models. This suggests a need for clearer operational guidelines, provider training, and supportive supervision to ensure that stable patients are systematically identified and referred to appropriate DSDMs. 25
HIV status disclosure was positively associated with DSDM utilization. Clients who had disclosed their HIV status were more likely to participate in community-based services, likely due to reduced fear of stigma, increased social support, and greater comfort engaging in group-based or community-linked care models. 26 Promoting safe, confidential, and supportive disclosure environments is therefore essential for expanding community-based DSDMs.
Although prior studies have suggested that urban residence is associated with better ART adherence, 27 residence was not statistically significant in the multivariable analysis of the present study (AOR = 2.48; 95% CI: 0.89-6.85). This apparent inconsistency may be explained by the stronger influence of individual-level factors such as education, disclosure status, treatment history, and provider referral practices which may outweigh geographic differences. Furthermore, recent decentralization of ART services and expansion of community health platforms in both urban and rural areas may have reduced traditional residence-based disparities, thereby diminishing the independent effect of residence on DSDM utilization.
The qualitative findings provide important contextual insights into these quantitative results. While some ART users demonstrated a basic understanding of community-based DSDMs and their role in HIV care, substantial misconceptions and knowledge gaps persisted. Some participants believed that DSDMs could cure HIV or were provided irrespective of HIV status. Cultural beliefs, including perceptions of HIV as a divine punishment and preferences for traditional remedies such as tsebel, further influenced engagement with biomedical care. Persistent stigma and fear of unintended disclosure also discouraged participation in community-based services. These findings underscore the need for culturally sensitive health education, stigma-reduction strategies, and improved community-level communication to enhance DSDM utilization.
Overall, expanding the uptake of community-based DSDMs has important public health implications, including reducing health facility congestion, improving patient retention, and enhancing viral suppression rates critical for HIV epidemic control.28,29 Health programs should integrate health literacy promotion, strengthen provider training on DSDM eligibility and referral, support safe disclosure counseling, and implement tailored re-engagement strategies for patients with a history of LTFU. Addressing provider-level, structural, and sociocultural barriers particularly those affecting referral practices and patient understanding is essential for the sustainable scale-up and effectiveness of community-based ART delivery models.30–32
Strengths and Limitations of the Study
This study has several strengths that enhance the reliability and applicability of its findings. The very high response rate (98.96%) minimizes the risk of non-response bias and improves the representativeness of the study population. The mixed-methods design is another key strength, as it allowed triangulation of quantitative findings with qualitative insights, thereby providing a more comprehensive understanding of community-based DSDM utilization. In addition, the study generates important baseline evidence to inform Ethiopia's ongoing scale-up of community-based ART delivery and identifies priority areas for intervention to improve uptake and retention within these models.
Despite these strengths, the study has some limitations. The cross-sectional design limits the ability to establish causal relationships between identified factors and DSDM utilization. Self-reported data may be subject to recall and social desirability bias, particularly for sensitive issues such as HIV status disclosure, adherence behaviors, and treatment history. Although qualitative data were collected and provided valuable insights into participants’ knowledge, beliefs, and experiences with DSDMs, the qualitative component was not designed to comprehensively explore all psychosocial, structural, and health-system factors influencing utilization. In particular, provider-level perspectives and in-depth exploration of health-system barriers were beyond the scope of the qualitative inquiry.
Conclusion
The utilization of community-based differentiated service delivery models among ART users in the study setting remains suboptimal, at 17.07%. Key factors influencing utilization included educational level, history of loss to follow-up, baseline CD4 count, HIV status disclosure, and ART regimen change. Enhancing uptake requires strengthening health literacy, addressing barriers faced by patients with prior treatment interruptions, improving provider referral practices, and promoting safe and supportive HIV status disclosure. Optimizing the implementation of community-based DSDMs has the potential to improve ART adherence, retention in care, and viral suppression while reducing health system burden in resource-limited settings such as Ethiopia.
Overall Implication
The findings of this study have significant implications for HIV care delivery in resource-limited settings like Northeast Ethiopia. Despite the proven benefits of community-based DSDMs in improving ART adherence, retention, and viral suppression, the utilization rate among ART users in the study area remains low at 17.07%. This underutilization is influenced by a combination of clinical, behavioral, and structural factors.
Key determinants such as educational status, history of loss to LTFU, baseline CD4 count, and HIV status disclosure were significantly associated with DSDM uptake. These findings suggest that improving health literacy, supporting treatment continuity, and creating safe environments for disclosure are critical to enhancing DSDM participation.
Moreover, qualitative insights revealed that misconceptions, lack of awareness, cultural beliefs, and stigma are major barriers to DSDM utilization. These findings underscore the need for targeted community education, culturally sensitive communication, and strengthened counseling services to address misinformation and promote acceptance of DSDM.
From a health systems perspective, scaling up community-based DSDM can decongest health facilities, optimize resource use, and extend care to underserved populations, particularly in rural areas. Tailored interventions that address both individual-level barriers and system-level constraints are essential for the successful implementation and sustainability of DSDM.
Supplemental Material
sj-docx-1-jia-10.1177_23259582261423607 - Supplemental material for Utilization and Associated Factors of the Community-Based Differentiated Service Delivery Model Among ART Users in Dessie Public Health Facilities, Northeast Ethiopia: A Mixed Method Study
Supplemental material, sj-docx-1-jia-10.1177_23259582261423607 for Utilization and Associated Factors of the Community-Based Differentiated Service Delivery Model Among ART Users in Dessie Public Health Facilities, Northeast Ethiopia: A Mixed Method Study by Endalkachew Mesfin Gebeyehu, Eyob Tilahun Abeje and Lakew Asmare in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582261423607 - Supplemental material for Utilization and Associated Factors of the Community-Based Differentiated Service Delivery Model Among ART Users in Dessie Public Health Facilities, Northeast Ethiopia: A Mixed Method Study
Supplemental material, sj-docx-2-jia-10.1177_23259582261423607 for Utilization and Associated Factors of the Community-Based Differentiated Service Delivery Model Among ART Users in Dessie Public Health Facilities, Northeast Ethiopia: A Mixed Method Study by Endalkachew Mesfin Gebeyehu, Eyob Tilahun Abeje and Lakew Asmare in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
List of Abbreviations
Acknowledgments
We would like to express our sincere gratitude to Wollo University, College of Medicine and Health Sciences for providing financial support to conduct this research. We also extend our appreciation to the Dessie City Health Administration Office for their cooperation and for providing essential preliminary information during the research process.
Our heartfelt thanks go to the participating public health facilities, as well as the data collectors, supervisors, and study participants, whose time, commitment, and collaboration were vital to the successful completion of this study.
Ethical Approval and Consent to Participate
Ethical approval for this study was obtained from the Ethical Review Committee of the College of Medicine and Health Sciences, Wollo University (Ref. No. WU CMHS 1415/13/17), dated 05/05/2017 (Ethiopian Calendar). Additional permission was secured from the Dessie City Health Administration Office and the respective public health facilities included in the study.
Prior to data collection, written informed consent was obtained from all study participants after providing them with adequate information about the purpose, procedures, potential risks, and benefits of the study. Participants’ confidentiality and anonymity were strictly maintained throughout the research process, and all collected data were used solely for the intended scientific purposes.
Consent for Publication
Not applicable.
Authors’ Contributions
EMG conceptualized the study, led data collection, performed the analysis, and drafted the manuscript. LA contributed to the study design, supervised data collection, and provided critical revisions to the manuscript. ETA assisted with data analysis, interpretation of findings, and manuscript editing.
All authors contributed to the conception, design, data collection, analysis, and manuscript preparation, and approved the final version of the manuscript. Corresponding Author: EMG (endalkmes12@gmail.com)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Wollo University,
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.