
Abstract
Little is known about the adaption of community-based organizations (CBOs) during the COVID-19 crisis. This study aimed to study how HIV CBOs and their community health workers (CHWs) faced the COVID-19 outbreak. Semi-structured interviews (n = 53) were conducted among CHWs in Burundi, Mauritania, and Lebanon in 2021. A thematic content analysis was performed. Results showed that CBOs had succeeded in maintaining HIV services and integrated COVID-19 prevention and awareness in their activities. COVID-19 led to innovation in terms of HIV services (eg, telemedicine and online psychosocial support) and to opportunities to try new modalities of antiretroviral therapy dispensation. Field workers (a specific group among CHWs) were negatively impacted by the COVID-19 crisis and showed resilience in their adaptation to ensure the continuity of their activities. Considering the essential role of field workers during the crisis, their status and the sustainability of their activities should be clearly supported by health policies and programs.
Plain Language Summary
This study explores how HIV community-based organizations (CBOs) and their community health workers (CHWs) adapted during the COVID-19 pandemic. We conducted interviews with 53 CHWs from Burundi, Mauritania, and Lebanon in 2021 to understand their experiences. We found that despite the challenges posed by COVID-19, CBOs managed to continue providing essential HIV services. They also incorporated COVID-19 prevention and awareness efforts into their work. The pandemic prompted innovation, such as the use of telemedicine and online psychosocial support, and provided opportunities to explore new ways of dispensing antiretroviral therapy (ART). However, field workers, a specific group of CHWs, faced significant negative impacts due to the pandemic. Despite these challenges, they showed remarkable resilience and adapted to ensure the continuity of their services. Given the critical role of field workers during the crisis, it is important for health policies and programs to support their status and ensure the sustainability of their activities.
Keywords
Introduction
Governmental restrictions during the COVID-19 pandemic disturbed healthcare services through lockdowns, curfews, and limitation to travel, 1 having an impact not only on people seeking healthcare during this time but also on health service providers. 2 Health workers have faced a high level of stress which could lead to an increase of burnout, depression, and anxiety among other mental health disorders. 3 All public and private health organizations had to adjust their activity to face the COVID-19 crisis which generated several challenges, including an increase in the demand of health care services and workloads, new and more complex (work) processes/practices, continuous updates of COVID-19 information and an increase of risk of exposure of health workers and their loved ones.3-5
The COVID-19 outbreak highlighted the need for pandemic prevention, preparedness, and response (PPR). 6 A comprehensive and holistic approach of strengthening PPR could be based on preexisting systems (prepandemic) and on lessons learned from prior pandemic responses, including community engagement. 6 For example, the 2019 Ebola outbreak in Democratic Republic of Congo illustrated the failure of the response and the difficulties to reach exposed people. The lack of community involvement in the response was pointed as one of the main factors related to this failure. 7 In the HIV response, on the other hand, community mobilization and engagement have been able to increase access to and retention in HIV prevention and care.
Community health workers (CHWs) have shown the capacity to support health systems serving as a bridge between communities and healthcare.8,9 Community health workers cover a heterogeneous profile of workers from peer educators (belonging to the populations targeted) to physicians working in community-based organizations (CBOs). Given their role in the context of both COVID-19 and HIV responses, it is crucial to document the adaptation of HIV CBOs and CHWs facing COVID-19 outbreak and supporting vulnerable populations. A rapid review of COVID-19 response-related publications from the South-East Asia region showed that CHWs expanded their regular tasks to take on new COVID-19-specific activities while maintaining essential services (Bezbaruah et al, 2021). However, this review also pointed to a lack of protective equipment for CHWs and a (preexisting) lack of recognition (monetary and non-monetary) of their contribution to health systems (Bezbaruah et al, 2021). Within the HIV field, published studies showed that the COVID-19 crisis has led to an acceleration of differentiated service delivery (DSD) models of antiretroviral therapy (ART) through CBOs1,10 to support the continuity of ART dispensation for people living with HIV (PLHIV). Continuation and scale-up of these models may further improve engagement and retention in care of PLHIV.
The role of CBOs and CHWs in HIV care is major in certain regions, such as Sub-Saharan countries and in South Africa, where public services were not well adapted and connected to PLHIV and to HIV key populations.11,12 Therefore, the objective of this exploratory qualitative study was to describe, on the one hand, the structural adaptations of HIV CBOs to face the COVID-19 crisis and, on the other hand, the personal experience of CHWs and their role regarding HIV key populations in Burundi, Mauritania, and Lebanon where CBOs play an important role in HIV care.
Methods
Design of the Study
This study was conducted within the framework of the community-based research program EPIC, a multicountry, cross-sectional, mixed methods and community based research program led by Coalition PLUS, an international union of CBOs involved in the fight against HIV and viral hepatitis since 2008.
The EPIC program aimed to (1) to study the impact of the COVID-19 crisis on populations exposed to (namely people who use or inject drugs, sex workers, men who have sex with men, trans people, and migrants; named thereafter key populations), or living with, HIV and/or HCV (PLHCV); (2) to study the impact of the COVID-19 crisis on CHWs (including peer educators, medical, and non-medical staff), and (3) to identify the key innovations and adaptations in HIV/HCV services that could be maintained and extended beyond the COVID-19 health crisis (Riegel et al, 2021). The EPIC program collected data between June 2020 and May 2022.
As a community-based research program, 13 EPIC was developed thanks to a collaboration between academic and non-academic-researchers, international experts, CHWs, and representatives of the key populations. The EPIC study group designed a general protocol and data collection tools that could be adaptable to the target populations and specific objectives of the organizations willing to implement EPIC in their country or region (Delabre et al, 2023). Therefore, to match the diverse themes of interest and target populations of the organizations participating in the EPIC program, as well as the specific local COVID-19 restrictions, each organization could adapt the general protocol and decide whether they wanted to implement a qualitative and/or a quantitative survey, targeting one or more key populations and/or CHW.
A total of 79 organizations implemented the EPIC program across 32 countries. Overall, a total of 119 studies were conducted: 67 quantitative and 52 qualitative.
Among 9 qualitative studies conducted among CHWs in 9 different countries, we selected interviews and transcriptions from 3 countries—Burundi, Mauritania, and Lebanon (n = 53)—for the present study, as they met the 2 study criteria: (1) interviews and transcriptions were of high quality and were suitable for scientific analysis; and (2) the chosen countries were quite similar in terms of their socioeconomic and cultural contexts (i.e., not including interviews from Asia or Latin America for instance).
Study Population
Community health workers in the current study were either HIV CBO volunteers or staff members who took part in the EPIC program. The term “CHWs” was defined within the framework of the EPIC program and refers to a broad spectrum of professionals and volunteers, including peer educators and healthcare providers at CBOs. 14 Interviewers contacted CHWs by phone or email from the CBOs in Burundi, Mauritania, and Lebanon that implemented the EPIC program. This included medical and non-medical staff (nurse, doctor, project/program coordinators, administrative staff, peer educators, and/or psychologists) working or volunteering at CBOs. The interviews were conducted among those who accepted to participate in the study.
Data Collection
In 2021, using a socio-constructivist approach, semi-structured interviews were conducted among CHWs to collect information on their experiences during COVID-19 crisis. To ensure consistency in methodology, a methodological webinar was organized with all the consultants prior to data collection. The interviews were conducted in the CHWs’ native language and recorded for transcription. Discourses were then transcribed in French for joint analysis, with identifying information removed. Data were securely transferred for analysis to the research team of Coalition PLUS in collaboration with participating CBOs.
The interview guide (see Supplemental Material) was developed in collaboration with the Coalition PLUS network and was based on literature on Ebola health crisis. 15 The interview guide focused on 2 main topics: (1) personal experiences of CHWs at work during the COVID-19 crisis and (2) impact of the crisis on their beneficiaries, which including HIV key populations and PLHIV or PLHCV. The first topic included questions related to work reorganization, the relationship of CHWs with their beneficiaries and co-workers, opinions about the reorganization, COVID-19 vaccination, and professional skills acquired during the crisis. The second topic included questions regarding the concerns CHWs had for their beneficiaries since the beginning of the COVID-19 crisis (needs, access to prevention and care, vulnerabilities), their own professional concerns, and the adequacy of services provided during the crisis with regard to meeting the needs of beneficiaries. The interviews were conducted in a private office space in the different CBOs’ premises to assure confidentiality.
Qualitative Analysis
We conducted a qualitative content thematic analysis of the full corpus of collected data (n = 53) (Bardin, 2016). First, we extracted the main discourse themes, and then we found correlations and relationships between these themes. To identify the themes, we conducted the analysis in 2 phases. First, we performed a vertical analysis for each interview, followed by a horizontal analysis using the continuous thematization approach, which consisted in identifying discourse themes and constructing the thematic tree simultaneously (Paillé & Mucchielli, 2013). Differences and similarities between themes were then explored (i.e., identification of relationships between themes). This analysis was performed using the NVivo® software.
The present study was conducted and reported in accordance with the COREQ checklist statement. 16 The COREQ checklist is provided in the Supplemental File.
Ethical Approval and Informed Consent
Ethical approval for the present study was obtained at the local level (Lebanon: Université Saint-Joseph: USJ-2021-129; Mauritania; Ministère de la santé/Comité d’éthique provisoire de la santé: 000580; Burundi: Comité national d’éthique pour la protection des êtres humains sujets de la recherche biomédicale et comportementale: CNE/21/2021). Before the start of each interview, the interviewers explained the study's purpose, and guaranteed data confidentiality and security. In accordance with the recommendations of local ethics committees to ensure the protection of individuals’ identity and the confidentiality of their participation in sensitive studies related to HIV and COVID-19, we chose to only collect oral—as opposed to written—informed consent for study participation, in order to minimize potential risks for participants. Oral consent was audio recorded in all cases. The interviewers were all external consultants (qualitative study experience) to ensure the confidentiality and the security of participants’ discourses. Two interviewers were men and one was a woman.
Results
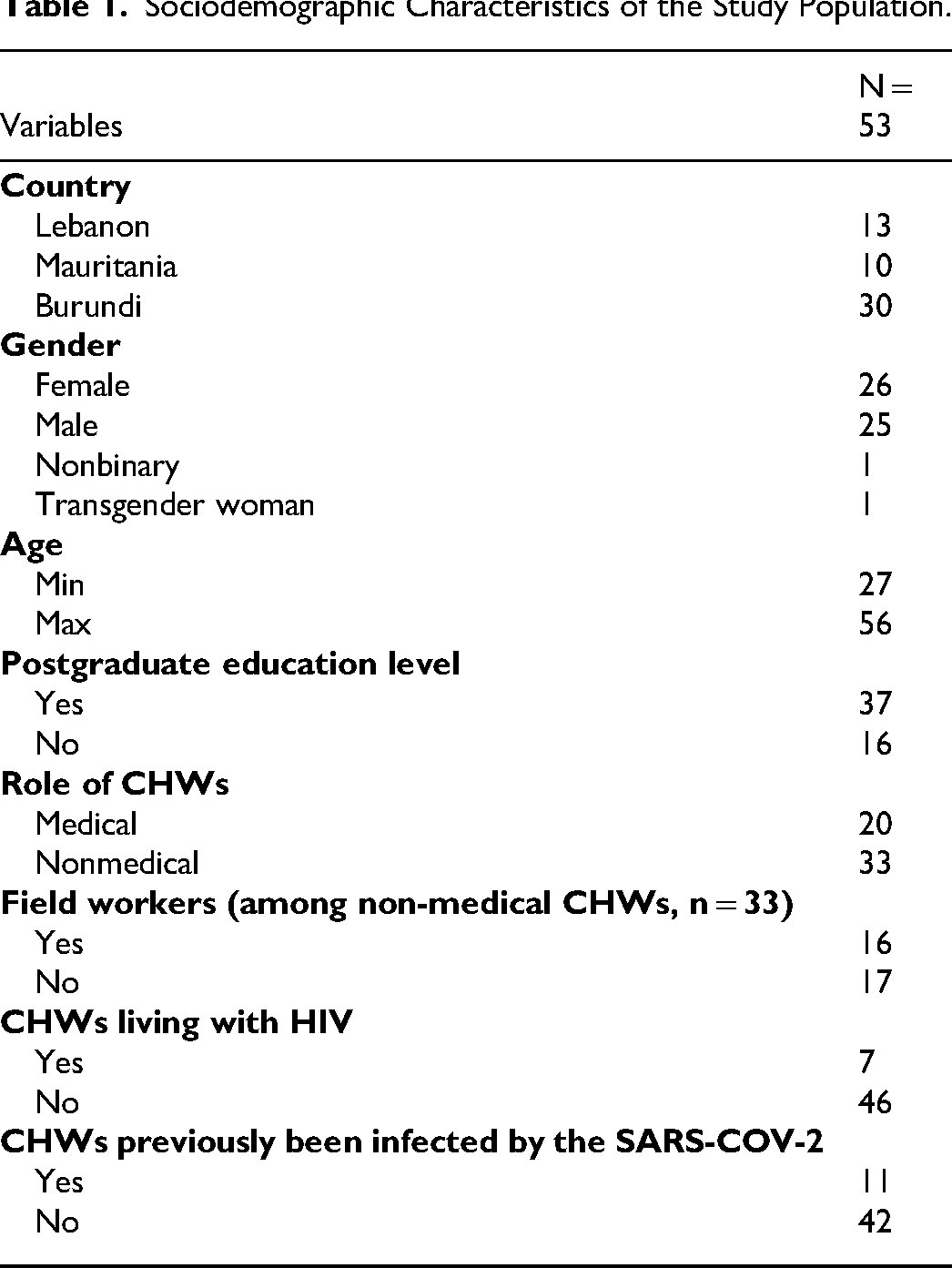
A total of 53 interviews were conducted with CHWs, including 13 from Lebanon, 30 from Burundi, and 10 from Mauritania. Among the participants, 25 self-identified as men, 26 women, 1 as non-binary, and 1 as a trans woman (Table 1). Age of the participants ranged from 27 to 56 years, and 37 reported completing a postgraduate education level. Among the 53 CHWs, 20 had a medical role in their CBO (e.g doctor, nurse, specialist) and 33 were non-medical CHWs (e.g., peer educator, project coordinator, facilitator, administrative support, management), including 16 field workers. Medical and non-medical CHWs included people who identify as PLHIV or key populations; this is mainly the case among field workers (such as peer educators). Seven participants were HIV positive and 11 had previously been infected by the SARS-COV-2 virus.
Sociodemographic Characteristics of the Study Population.
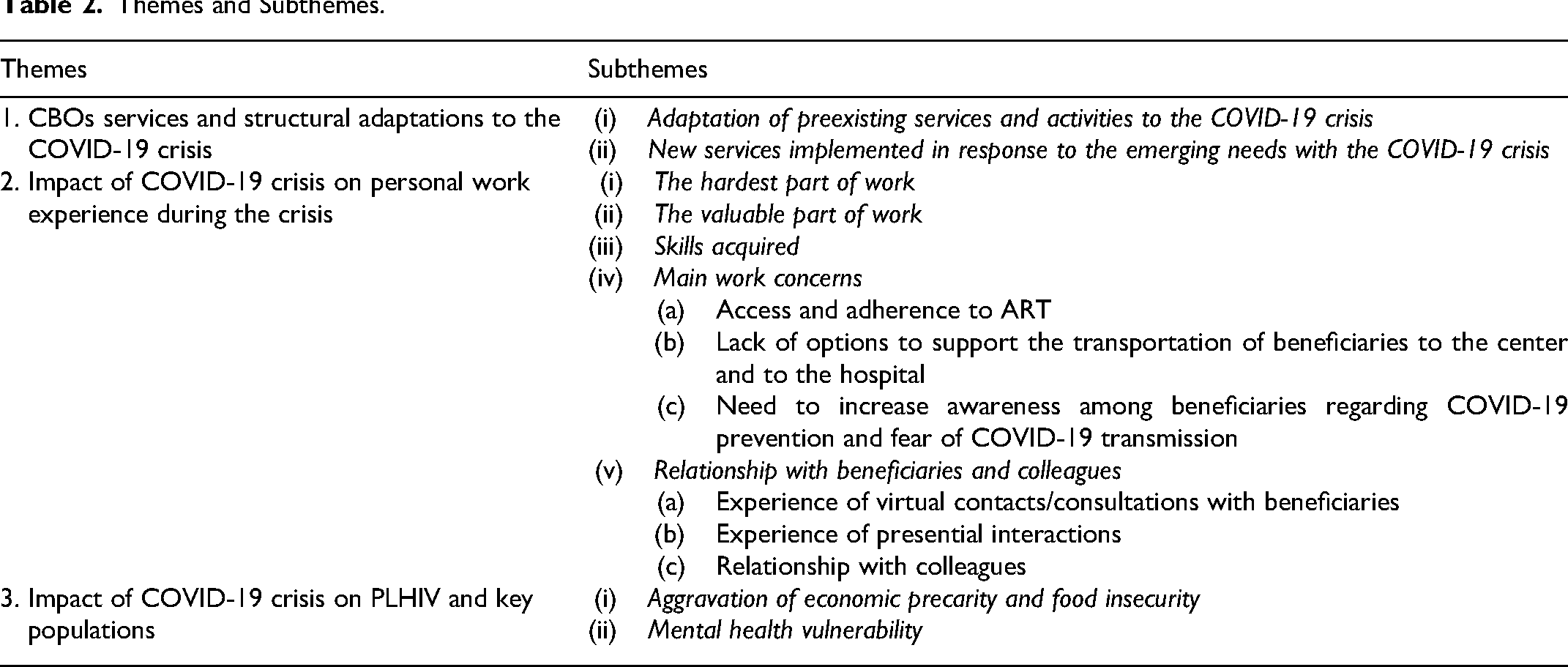
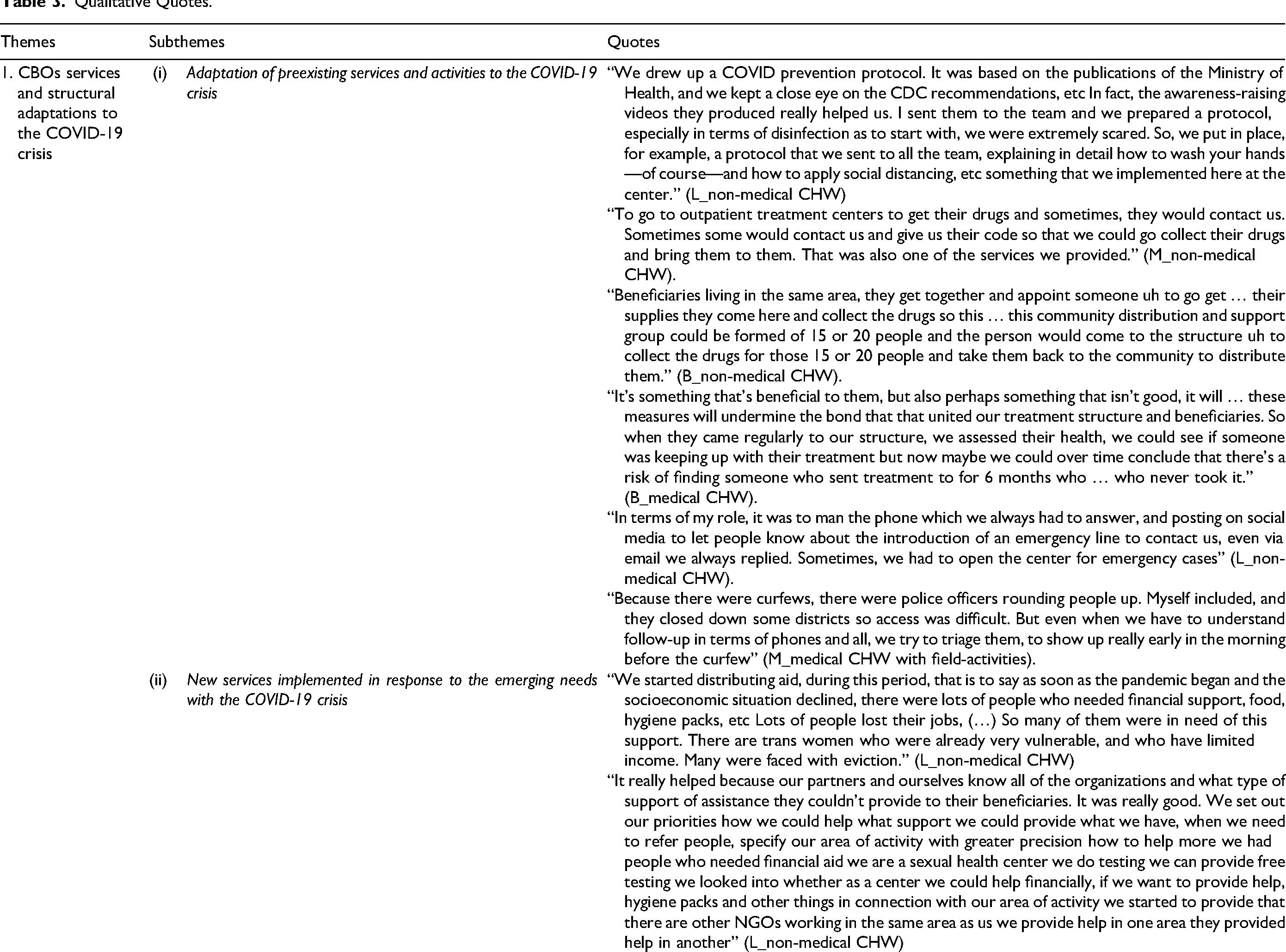
In relation to our objectives, 3 meta themes emerged from the interviews among CHWs (Table 2): (1) CBOs services and structural adaptations to the COVID-19 crisis which includes the following sub-themes: (1) adaptation of preexisting services and activities to the COVID-19 crisis and new services implemented in response to the emerging needs with the COVID-19 crisis; (2) impact of COVID-19 crisis on personal work experience during the crisis which includes the following sub-themes: (1) the hardest part of work; (2) the valuable part of work; (3) skills acquired; (4) main work concerns (access and adherence to ART; lack of options to support the transportation of beneficiaries to the center and to the hospital; and need to increase awareness among beneficiaries regarding COVID-19 prevention and fear of COVID-19 transmission), and (5) relationship with beneficiaries and colleagues during the crisis (experience of virtual contacts/consultations with beneficiaries; experience of presential interactions; and relationship with colleagues); and (3) impact of COVID-19 crisis on PLHIV and key populations which includes the following sub-themes: (1) aggravation of economic precarity and food insecurity and (2) mental health vulnerability. Some of the quotes related to the themes and sub-themes of this analysis are presented throughout the results section. All related quotes are provided in Table 3.
Themes and Subthemes.
Qualitative Quotes.
Meta-Theme 1: CBOs Services and Structural Adaptations to the COVID-19 Crisis
This meta-theme was focused on the structural reorganization of the CBOs in terms of service dispensation and included 2 main themes: (1) adaptation of preexisting services and activities, including health measures and processes to prevent COVID-19 transmission at the CBOs (to protect CHWs and beneficiaries) and (2) new services implemented in response to the emerging needs.
Adaptation of preexisting services and activities to the COVID-19 crisis (n = 53)
Only medical services and emergencies were maintained face-to-face at the CBOs. A COVID-19 protocol was implemented to prevent COVID-19 transmission between CHWs and beneficiaries. The protocol included several measures concerning the reception of beneficiaries, such as spacing out the appointments and increased hygiene measures during the visit, limiting entrances and exits, checking temperature and other COVID-19 symptoms before entry, providing protection equipment against COVID-19 for beneficiaries and suspending group activities. Furthermore, CHWs were trained on COVID-19 transmission and were provided with protective equipment by CBOs or medical partners. A rotation of CHWs was sometimes put into place to protect CHWs and assure the continuity of the services. Finally, CHWs integrated COVID-19 prevention in their daily activities and services toward beneficiaries. All these measures were often linked with the local sanitary measures of the country and were positively evaluated by the CHWs, who consequently felt safe at work. “We drew up a COVID prevention protocol. It was based on the publications of the Ministry of Health, and we kept a close eye on the CDC recommendations, etc In fact, the awareness-raising videos they produced really helped us. I sent them to the team and we prepared a protocol, especially in terms of disinfection, as to start with, we were extremely scared. So, we put in place, for example, a protocol that we sent to all the team, explaining in detail how to wash your hands—of course—and how to apply social distancing, etc something that we implemented here at the center.” (L_non-medical CHW)
Within the context of service adaptation to limit transmission and respect of governmental mobility restrictions, new modalities of ART dispensation were proposed during the crisis by CBOs. Indeed, we noted that innovations such as multimonth ART dispensing, at home-delivery of ART, community-relay ART dispensation (i.e., PLHIV living in the same locality chose a representative to collect ART for all of them) allowed a continuity of ART dispensation and supported ART adherence. “Beneficiaries living in the same area, they get together and appoint someone uh to go get … their supplies. They come here and collect the drugs, so this … this community distribution and support group could be formed of 15 or 20 people and the person would come to the structure uh to collect the drugs for those 15 or 20 people and take them back to the community to distribute them.” (B_non-medical CHW).
However, these innovative ART-dispensation services raised concerns in terms of beneficiaries’ follow-up. Although these innovations were implemented during the COVID-19 crisis to maintain beneficiaries on treatment, the CHWs expressed concern about the lapse of time between each CBO appointment, as it could lead to missing opportunities in health support (e.g., treatment adherence, clinical exams, psychological support). Before the health crisis, ART dispensation appointments were also an opportunity to check medical and psychosocial needs of the beneficiaries and their ART adherence. CHWs therefore expressed concern of an increase in lost to follow-up among PLHIV over the long term. “It's something that's beneficial to them, but also perhaps something that isn’t good, it will … these measures will undermine the bond that that united our treatment structure and beneficiaries. So when they came regularly to our structure, we assessed their health, we could see if someone was keeping up with their treatment but now maybe we could over time conclude that there's a risk of finding someone who sent treatment to for 6 months who … who never took it.” (B_medical CHW).
Services such as psychosocial support, peer education, and prevention transitioned, in most cases, online or to text messaging or phone contacts. Groups activities were delayed. Sometimes one-to-one face-to-face counseling was able to be conducted while respecting masking requirements and physical distancing. These activities targeting key populations were mainly led by non-medical CHWs. Therefore, these CHWs were the most affected in their work by the COVID-19 crisis. In addition, health and political restrictions also led to an in-depth reorganization of their activities. Field workers had fewer field-based activities (e.g., HIV prevention and screening in specific public venues) and had to conduct their prevention activities online or during the day to adapt to the curfews.
According to field workers’ discourses, flexibility in their professional practices was necessary during the crisis to maintain contact with beneficiaries and services. When online prevention was not sufficient (e.g., to distribute condoms), field workers continued to meet key populations at private/public spaces but left sooner than usual. In some cases, field workers had to contend with police presence by informing and raising awareness of their work to explain their presence despite restrictions. “Because there were curfews, there were police officers rounding people up; myself included. And they closed down some districts so access was difficult. But even when we have to understand follow-up in terms of phones and all, we try to triage them, to show up really early in the morning before the curfew” (M_non-medical CHW).
New services implemented in response to the emerging needs with the COVID-19 crisis (n = 12)
The COVID-19 crisis and associated restrictions affected the economic situation of people in an already precarious situation, resulting in an increased need to provide economic and food support. Food kits and COVID-19 protection kits were distributed, and financial support was provided for those in the most precarious situation. These services were for a large part ensured by field workers. “We started distributing aid during this period, that is to say as soon as the pandemic began and the socio-economic situation deteriorated, there were lots of people who needed financial support, food, hygiene packs, etc Lots of people lost their jobs, (…) So many of them were in need of this support. There are trans women who were already very vulnerable, and who had limited income. Many were faced with eviction.” (L_non-medical CHW)
The creation of new partnerships with other organizations, which had complementary skills or field actions/activities, was another way to respond to emergent needs and provide a more global response. For example, humanitarian issues (e.g., food insecurity, precarity) were a particular concern and other organizations were better placed to respond to these needs. HIV CBOs, however, could provide services such as HIV screening, for a broader subgroup of populations experiencing precarity which could lead to higher HIV exposure.
Meta-Theme 2: Impact of COVID-19 Crisis on Personal Work Experience
Meta-theme 2 described the personal work experience of CHWs during the COVID-19 crisis and how they experienced the structural reorganization of the CBO.
All CHWs reported a work overload since the beginning of the COVID-19 crisis mainly due to the frequent absence of coworkers infected by the COVID-19, the new tasks linked to COVID-19 prevention, and the lack of supplementary human resources.
Field workers encountered specific difficulties during the crisis due to local restrictions which interrupted outreach and group activities. Social distancing and movement restrictions were significant barriers to the field work, specifically for activities at night. Despite these challenges, field workers reorganized their activities to respond to beneficiaries’ essential needs and expressed a feeling of non-accomplishment, as their work was based on the frequent interactions and in-depth relationships with beneficiaries outside the CBO. The lack of these in-depth exchanges during the COVID-19 crisis weakened the link between field workers and beneficiaries and made it difficult to propose their regular (pre-COVID) activities such as HIV screening, linkage to care, and in-depth HIV awareness-raising.
This meta-theme also pooled 5 subthemes: (1) the hardest part of work during the crisis; (2) the valuable part of work during the crisis; (3) skills acquired during the crisis; (4) main work concerns during the COVID-19 crisis, and (5) relationship with beneficiaries and colleagues during the COVID-19 crisis.
The hardest part of work during the crisis (n = 39)
Three elements were most often considered as the most difficult part of work since the beginning of the COVID-19 crisis. The first element was the concern of COVID-19 transmission and respect of the COVID-19 prevention measures during the interaction with the beneficiaries, such as outreach activities and home-visits. Community health workers were worried about COVID-19 transmission even if they were protected, specifically when they had to be close to the beneficiaries (e.g., clinical exam, testing). “The difficult part was, at the start I was scared; people said that when someone was infected with COVID, if you got close to them you caught it too. To be honest, that was hard, making visits to the homes of people who were … the people close to the infected person. During the visit we’d go see why they weren’t coming anymore to collect their drugs and you’d think to yourself you’d be visiting a person with COVID. That was hard.” (B_non-medical CHW)
The second element concerned COVID-19 risk awareness among the beneficiaries. According to CHWs discourses, a proportion of the beneficiaries reported misinformation about COVID-19 risk and the importance to respect prevention measures. COVID-19 awareness represented a significant issue for CHWs, on one hand to assure their own protection and, on other hand, to assure the protection of beneficiaries, who often had comorbidities, and the protection of the greater community.
Third element concerned CHWs’ perception of social distancing as a barrier for their activities and for their relationship with the beneficiaries. Indeed, social distancing not only impeded several group and social activities but also complicated the social support (e.g., physical proximity; caring gestures) normally provided in certain situations such as HIV seroconversion. “The hardest part of this work is the human contact. For example, when someone tests positive for HIV, an important way of reassuring them that they are not sick is by shaking their hand, or a hug. Which is not possible now. So that's really hard. Sometimes a hug or simple contact is the human interaction that that person needs at that time.” (L_non-medical CHW)
The valuable part of work during the crisis (n = 42)
The most valuable part of the work was to be present for the beneficiaries during the crisis, to adapt their services to their needs and to ensure a continuity of preexisting services. During this time, social and medical support in the public health system were rare and CHWs were proud to take part in the continuity and availability of these services for the beneficiaries. “I think that what was valuable … despite the crisis it was being able to adapt, I think that it's adapting so that the service can continue as needed. That's valuable I think. I don’t know if … to adapt to the situation and continue to protect ourselves to avoid being infected and continuing to offer services to patients I think that that's what gives value to our activities or what demonstrates our value I think.” (B_non-medical CHW)
Skills acquired during the crisis (n = 19)
Community health workers reported to have acquired some skills to face the COVID-19 crisis. The 3 skills most frequently reported were: (1) the ability to use information and communication technologies to stay connected with the beneficiaries and co-workers and to pursue HIV and COVID-19 awareness and prevention online (n = 6); (2) the capacity to adapt to the context (n = 7); and (3) the integration of COVID-19 measures in their professional practices (n = 6).
Main work concerns during the COVID-19 crisis (n = 53)
Community health workers reported 3 main professional concerns during the COVID-19 crisis with regard to the beneficiaries: (1) access and adherence to ART; (2) the lack of options to facilitate transportation of beneficiaries to the community-based health center and to the hospital; and (3) the need to increase COVID-19 prevention awareness among beneficiaries and the fear of COVID-19 transmission.
Access and adherence to ART (n = 15)
Community health workers highlighted an increase of lost to follow-up among the PLHIV. Indeed, fear of COVID-19 led PLHIV to avoid public transportation or avoid leaving their home and fear of being exposed to a COVID-19 positive person at the center. Lockdowns and quarantines for COVID-19 positive people were also barriers to ART access.
For these reasons, CHWs reported a decrease in ART adherence among PLHIV. Community health workers were focused on maintaining access and adherence to ART to reduce the number of PLHIV who interrupted their treatment. “Patients weren’t coming in anymore, we lost contact with lots of them, many stopped taking their treatment. This was exacerbated by the fact that at the HIV center itself, the first COVID center was there (…) it wasn’t more than 100 meters from the outpatient treatment center. I think that that was one of the reasons for this drop-out, the fact that patients weren’t coming to the center anymore it's because of that, they were scared of being infected.” (M_medical CHW)
Lack of options to facilitate the transportation of beneficiaries to the center and to the hospital (n = 10)
The lack of individual means of transportation was highlighted by CHWs for several reasons. First, CHWs would have preferred individual transportation to avoid contact in public transportation and reduce potential COVID-19 exposure. Second, public transportation services were reduced and more expensive during this time. This created difficulties for field workers to conduct their outreach activities, mainly after the curfew. Third, additional transportation provided by CBOs could have facilitated transportation of beneficiaries to the center and linkage to care by the CHWs when it was necessary.
Need to increase awareness among beneficiaries regarding COVID-19 prevention and fear of COVID-19 transmission (n = 48)
COVID-19 prevention was an important concern of CHWs for several reasons. Firstly, CHWs were worried for the beneficiaries if they got COVID-19 because most of them were vulnerable in terms of health access and social support, and a large proportion lived with comorbidities such as HIV, diabetes, or hypertension. COVID-19 quarantine and treatment could increase their precarity and social stigma. Moreover, CHWs were aware of the cultural and economic barriers to COVID-19 prevention among the beneficiaries. Secondly, CHWs were concerned about the availability of COVID-19 protection equipment over the long term for themselves and for the beneficiaries. Thirdly, CHWs were afraid to contract COVID-19 at work or on transportation to work. COVID-19 infection also represented a concern for the continuity of services and for their own family's protection. “Yeah, at the beginning, when we started going back to the office, we were naturally worried about it: will I catch COVID-19? Am I washing my hands enough? Are all of the staff following the protocol correctly? The beneficiaries who come to the center, does one of them have COVID? All that caused us a lot of anxiety, because we have a responsibility to our parents. It's not just about you, it's also about the people you pass the virus onto. So that was a source of anxiety.” (L_non-medical CHW)
Relationship with beneficiaries and colleagues during the COVID-19 crisis
Communication with beneficiaries and colleagues was modified due to social distancing, fear of COVID-19 transmission, and local restrictions. This section describes how CHWs managed their relationships with beneficiaries and with their colleagues during the crisis.
Experience of virtual contacts/consultations with beneficiaries (n = 44)
Community health workers had mixed feelings regarding their experiences of virtual interactions during the crisis. Several positive elements were raised but were linked with the context when face-to-face interactions were impeded or discouraged.
Among positive elements, virtual contacts/consultations allowed to maintain a link and allowed beneficiaries to ask questions and to express their feelings and needs. Information and awareness on COVID-19 and HIV were also done online. Online relationships were also a way to ensure psychosocial support.
Virtual contacts/consultations also saved time (less time spent in transport and ability to provide quick responses) and helped to reduce the risk of COVID-19 transmission by limiting in-person contact.
Although virtual contacts/consultations had several positive points, CHWs highlighted that it was necessary to be aware of its limits and that virtual contacts could not fully replace face-to-face interactions. For example, virtual contacts could be used in conjunction with face-to-face interactions or in specific crisis situations.
Indeed, several barriers were identified, such as technical difficulties related to the devices (phone, computer, tablet) and the internet connection. The primary barriers were that virtual interactions could not meet all the beneficiaries needs and that there was lack of intimacy associated with the virtual contacts/consultations.
Virtual contacts/consultations were also incompatible with clinical examens and diagnosis of certain pathologies. “It's a good thing. It's always good to keep in contact with the person, but nothing beats physical contact, because as I say in that case there's that perception, and there's everything everything can be read, on, on the person's face. But by phone it's uh, social networks, it's good, it's a good means of communication, it allows us to keep in contact. But uh, there are some things that aren’t conveyed. There's not that perception.” (M_non-medical CHW)
Experience of face-to-face interactions during the crisis (n = 12)
When they could be maintained, CHWs reported a high satisfaction with face-to-face contacts/consultations. By respecting COVID-19 prevention measures, CHWs felt that COVID-19 transmission would be sufficiently limited for themselves and for the beneficiaries, to conduce face-to-face meetings. Community health workers highlighted that face-to-face contacts were the best way to be present for the beneficiaries. “Yes we stay with our beneficiaries because we can’t leave them. We can’t leave them; they need us at all times. So we’re there to help them. That's why we can’t leave them. So on top of that we do visits; we need to accompany them to the shelter where they’re staying, with taking their medication, we need to accompany them; that's why … that's why we can’t leave them. So we need to find ways, we need to protect ourselves effectively to stay in contact so that we, if they need us they can see us easily.” (B_medical CHW)
Relationship with colleagues during the COVID-19 crisis (n = 53)
Concerning professional relationships within the CBOs, CHWs reported that positive collaboration practices were maintained. Interactions and professional life were adapted to the COVID-19 prevention measures. CHWs reported good relationships and support within CBOs despite the social distancing and mask-wearing. The necessity to respect COVID-19 prevention measures between them was frequently reported.
The support provided by work colleagues was also adapted to the context, for example, in case of COVID-19 infection, support provided by the colleagues was provided by phone and not by home visits as it is usually done.
Although participants expressed a lack of social interaction at work, CHWs were aware of the necessity to continue with COVID-19 prevention measures. “Yes that's right. If there's a case of COVID among us, well we feel like we shouldn’t go to their home in case of COVID, well if our colleagues are in isolation. We changed our behavior; I can’t think about going to see them at home but I can phone or …. send a message, but I can’t go straight to the house for a visit.” (B_medical CHW)
Meta-Theme 3: Impact of the COVID-19 Crisis on PLHIV and Key Populations
This meta-theme showed the impact of COVID-19 on PLHIV and key populations from the perspective, and through the work, of CHWs. Two major consequences were observed by CHWs: (1) aggravation of economic precarity and food insecurity and (2) mental health vulnerability.
Aggravation of economic precarity and food insecurity (n = 39)
During the COVID-19 crisis, a large part of PLHIV and key populations lost their jobs or had less income, leading to increased economic precarity and difficulty accessing essential needs (food and care).
This increase in precarity also led to a reduction in the attention paid to sexual health and ART adherence. For example, an increase in behaviors which may increase exposure to HIV (e.g., sexual encounters without condoms or other prevention tools such as PrEP) was observed among sex workers to make more money.
Furthermore, ART access was more difficult (in terms of transportation costs as described in meta-theme 2) as well as access to food (shortages and cost). This caused a global deterioration of the quality of life of PLHIV. Several PLHIV preferred not to take their ART treatment if they did not have access to food.
In the specific case of Lebanon, shortages of condoms, STI testing, and medications represented a bigger issue compared to the other countries. “The border closure exacerbated the lack of economic power, and these key populations are the ones that suffer more, and a person can do everything and they can agree to unprotected intercourse for money, and a man or a woman is willing to do anything to feed their children” (M_non-medical CHW)
Mental health vulnerability (n = 6)
People living with HIV and key populations were a part of marginalized populations before the COVID-19 crisis and, from the point of view of CHWs, the crisis further led to less social support for these populations.
Mental health disorders emerged among PLHIV and key populations during the COVID-19 crisis. Curfews, lockdowns, and social distancing led to greater isolation and with the fear caused by COVID-19, a large part of these groups reported depressive symptoms. “I have some patients (nervous laughter) who suffered during COVID; they were afraid because they felt very vulnerable. They felt vulnerable, some of them, you could see the fear in their eyes, (…) but mostly fear, a phobia even, you could tell, because they knew that they were already HIV positive. Especially for those who suffer from other infections or pathologies like high blood pressure and uh, heart conditions. Those people were afraid because on top of COVID, it's, it's difficult for them.” (M_non-medical CHW)
Discussion
Results of this community-based qualitative research study showed that CBOs succeeded in maintaining HIV services despite the crisis and integrated COVID-19 prevention and awareness in their activities. This contributes to previous evidence suggesting that community engagement can effectively support health systems, serving as a bridge between communities and public health issues.8,9 This study also documents that COVID-19 crisis led to innovation in terms of HIV services, including a shift toward telemedicine and online psychosocial support, as well as new modalities of ART dispensation. Field workers, who constitute a specific group among CHWs, were especially negatively impacted by COVID-19 prevention and control measures (curfews, lockdowns, restrictions to travel) in our study and demonstrated resilience in adapting their practices to ensure their activities. Another study from West Africa also showed resilience among peer educators through the adaptation of their practices by relocating prevention activities from public to private areas, reducing group sizes, moving night activities to the daytime, increasing the use of social networks, integrating hygiene measures, and promoting assisted HIV self-testing as an alternative to conventional rapid testing. 17 Our results showed that all CHWs (not only field workers) developed the necessary skills to adapt their practices within the pandemic context.
The capacity of CBOs to assure the continuity of HIV services and of psychosocial support among their beneficiaries, while considering COVID-19 prevention and awareness-raising in their daily work, illustrated the resilience of the HIV CBOs involved in this study. Indeed, resiliency was recently defined in the field of health systems as the capacity of health organizations and health workers to absorb shocks while maintaining their services and responding to the beneficiaries needs, including the emergent needs.18,19 For this, CHWs developed new skills, not only in terms of COVID-19 prevention but also in terms of the use of technological communication tools. Although CHWs felt face-to-face interactions were a better way to support beneficiaries, CHWs have nonetheless taken advantage of these virtual solutions to maintain a link with beneficiaries. Other studies in the community-based context showed the issues associated with virtual contact among vulnerable populations and the variety of tools used.20,21CHWs in this study demonstrated a high work engagement during this crisis to adapt their work to constraints, absorb the workload linked to the limited human resources (e.g., absences due to COVID-19 infection). They also increased awareness of COVID-19 transmission among the beneficiaries and accepted contact with beneficiaries under secure conditions (with personal protective equipment). These results echo the 3 preconditions of resilience in health systems which were learned from the Ebola outbreak: the recognition of the severe nature of the health crisis, a legal and policy foundation to guide the response and the implementation, and a need for a strong and committed health workforce. 18 Based on their previous expertise regarding mobilization for HIV, CHWs quickly implemented COVID-19 prevention protocols in their CBOs and reoriented a large part of their work toward COVID-19 prevention and associated emergent needs. The regular COVID-19 updates from the international health authorities, such as the WHO, also favored this mobilization.
The resilience of HIV CBOs during the COVID-19 crisis observed in this study should encourage the collaboration between the community-based health system and the traditional public and/or private health systems in the event of future outbreaks, particularly among vulnerable populations. This collaboration could help maximize the response during epidemics and respond to the specific needs of these populations who are often not reached by prevention measures that are tailored to the general population.
Resilience should also be considered at the structural level. Local and individual adaptations within stressful environments are not sustainable, and individual coping strategies will be minimized in such a context. 22 The focus on resilience at the local level should not downplay structural issues. 22 Lack of PPR and the missed opportunity to fully integrate preexisting health systems (including the community-based system) were some of the structural weaknesses of the COVID-19 response. 6 The role and impact of CBOs and CHWs on the COVID-19 response could have been more effective if they were integrated with health systems and aligned with health authority guidelines. 23 Community-based systems can complement more traditional health systems by providing adapted, people-centered services for key populations. This people-centered care (PCC) is strongly present throughout the CHWs interviews in the present study through, for example, at home-delivery of ART for PLHIV which could not move to the HIV center, community-relay ART dispensation, food kits, and COVID-19 protection kit distribution, and financial support for those in the most precarious situations. PCC is a key to quality healthcare 24 and is promoted to achieve the 90-90-90 targets of the World Health Organization. 25 Moreover, PCC is also a means to implement DSD. 26 According to the WHO recommendations, DSD aims to adapt how HIV services (frequency, places, type of healthcare workers, type of services needed) are provided and to consider the specific needs of subpopulations, such as key populations, and their contextual settings. This definition of DSD fits with CBOs tasks and work organizations found in this study.
A review of lessons learned from 28 countries on health system resilience during the COVID-19 crisis recommended that countries worldwide should be open to exchanges with Asia and Africa regions about their knowledge and expertise on mobilization of CBOs and CHWs to optimize the reach, the capacity, and the quality of their health systems. 27
From the perspective of CHWs in the present analysis, an aggravation of socioeconomic vulnerabilities was observed among populations living or exposed to HIV, as reported in other studies.28-31 Food and job insecurity and mental health issues may have resulted in a deprioritization of health for populations living or exposed to HIV. With this reality, it was important for CHWs to address the emergent needs of the beneficiaries through the implementation of new services such as additional modalities of ART dispensation (at-home, by a community relay, multimonth dispensation), and support for food and hygiene. Therefore, CHWs developed services consistent with humanitarian support in addition to regular HIV services.
The results of our study highlight the essential role of non-medical CHWs, particularly field workers, in the implementation of new services to face the COVID-19 crisis. Our results suggest that the long-term availability of protective equipment was an anticipated concern for some CHWs, supporting results from other studies.8,10 Additionally, the lack of legitimacy of their work 32 put into question their safety and exposed them to confrontations with the police. Concerns and issues with police confrontations were not addressed in the interview guide but were spontaneously brought up by the participants from Mauritania. Therefore, we cannot say whether this was a specific concern associated with their country/political context. However, according to published articles, police confrontations were already a concern outside the context of the COVID-19 pandemic. 33
Field workers and peer educators were often in a precarious situations in relation to their unrecognized status 34 which was aggravated during the crisis by the discontinuity of income. Overall, the COVID-19 crisis has provided additional evidence of the strength and commitment of CHWs and specifically field workers, and the need of supporting their efforts and advocating for their recognition and rights. 35 Moreover, and outside the context of a health crisis, the results of this study can be used to inform and advocate for a better recognition and integration of HIV community-based services in the health systems.
This study had a few limitations. Firstly, CHWs included in this qualitative study belong to an international union of HIV CBOs which provided support during the crisis. This support could have influenced the resilience of their systems; therefore, these results cannot be generalized to all HIV CBOs. However, a survey conducted by UNAIDS among CBOs (n = 225 among 72 countries) also reported that CHWs have ensured continuity of HIV services and at the same time they also undertook new interventions to respond to the COVID-19 pandemic itself. 36 Secondly, although the study was proposed by an external consultant, the initiative of this study came from the upper management of the participating CBOs. Although the upper management did not have access to the transcriptions or audios of the interviews collected, this could have increased the chance of social desirability bias in the discourse of CHWs. Thirdly, study participation was voluntary. It is possible that CHWs who had a very negative experience of the COVID-19 crisis at work did not participate.
Finally, all CHWs interviewed were in Burundi, Mauritania, and Lebanon but represented various cultural, political, and socioeconomical contexts. For example, in Lebanon, data were collected after the Beyrouth explosion. Therefore, some elements in the discourse of CHWs from Lebanon were linked with the COVID-19 crisis and with the post-explosion context.
Conclusions
Results of this qualitative multicountry community-based research study conducted among CHWs in Burundi, Mauritania, and Lebanon showed that HIV CBOs had the capacity to adapt their services during the COVID-19 pandemic and to consider the emergent needs among people living or exposed to HIV. HIV CBOs showed resilience during the COVID-19 crisis and should be part of public health responses in the future to better reach and support vulnerable populations. Considering the essential role of field workers during the crisis, their status and the sustainability of their activities should be taken into consideration by health policies.
Supplemental Material
sj-docx-1-jia-10.1177_23259582241263686 - Supplemental material for How Community-Based Organizations Responded to the Covid-19 Crisis to Maintain HIV Services Among Vulnerable Populations in Burundi, Mauritania, and Lebanon: Qualitative Results From the Multicountry EPIC Program
Supplemental material, sj-docx-1-jia-10.1177_23259582241263686 for How Community-Based Organizations Responded to the Covid-19 Crisis to Maintain HIV Services Among Vulnerable Populations in Burundi, Mauritania, and Lebanon: Qualitative Results From the Multicountry EPIC Program by Marion Di Ciaccio, Othmane Bourhaba, Cécile Khoury, Ayman Assi, Sara Abu Zaki, Nicolas Lorente, Juliana Castro Avila, Annabelle Niyongabo, Dévote Gakima, Aminata Diouh, Lucas Riegel, Amal Ben Moussa, Gabriel Girard, Mehdi Karkouri, Rosemary M. Delabre, Daniela Rojas Castro and in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582241263686 - Supplemental material for How Community-Based Organizations Responded to the Covid-19 Crisis to Maintain HIV Services Among Vulnerable Populations in Burundi, Mauritania, and Lebanon: Qualitative Results From the Multicountry EPIC Program
Supplemental material, sj-docx-2-jia-10.1177_23259582241263686 for How Community-Based Organizations Responded to the Covid-19 Crisis to Maintain HIV Services Among Vulnerable Populations in Burundi, Mauritania, and Lebanon: Qualitative Results From the Multicountry EPIC Program by Marion Di Ciaccio, Othmane Bourhaba, Cécile Khoury, Ayman Assi, Sara Abu Zaki, Nicolas Lorente, Juliana Castro Avila, Annabelle Niyongabo, Dévote Gakima, Aminata Diouh, Lucas Riegel, Amal Ben Moussa, Gabriel Girard, Mehdi Karkouri, Rosemary M. Delabre, Daniela Rojas Castro and in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The authors thank all CHWs who gave their time to participate to this qualitative survey. The authors would also like to thank the EPIC study group, partnering CBOs, and other individuals who gave their time and support and who were essential to the success of the EPIC program.
Author Contributions
Contribution of all authors: MDC conducted the analysis and wrote the manuscript; OB coordinated the global study; CK participated to data collection and transcription; AA, DG, SAZ, and AD coordinated the local studies; NL and RL coordinated EPIC program; JCA, AN, ABM, and GG participated in the development of study survey, data collection, and manuscript revision; MK, RD, and DRC supervised the study and manuscript revision. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agence Nationale de Recherches sur le Sida et les Hépatites Virales ainsi que les Maladies infectieuses Emergentes (L’ANRS | MIE) and the Agence Française de Développement.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.