
Abstract
Studies investigating same-day antiretroviral therapy (ART) initiation demonstrate different clinical outcomes depending on settings. We retrospectively reviewed adults with newly positive human immunodeficiency virus (HIV) antibody testing. The proportion of individuals who were retained in care at 12 months was compared between early (≤2 weeks) and late (>2 weeks) ART initiation groups. Of all, the median (IQR) time from HIV diagnosis to ART initiation was 18 (9-30) days. This duration was 7 (7-13) days in the early ART initiation group (n = 116) and 28 (21-46) days in the late ART initiation group (n = 154). In the multivariate logistic regression, having pneumocystis pneumonia [odds ratio (OR) 9.30, 95% CI 2.56-33.75], tuberculosis (OR 2.21, 95% CI 1.03-4.73), and weight loss (OR 12.98, 95% CI 1.00-167.68) were associated with late ART initiation. The early ART initiation group had a slightly higher proportion of individuals retained in care at 12 months than those in the late ART initiation group (88.8% vs 80.5%, P = .066) and had a higher significant proportion of HIV viral load suppression (81.0% vs 70.1%, P = .041). No significant differences were observed in the proportion of individuals who died at 12 months (2.6% vs 3.2%, P = 1.000) between the two groups. Early ART initiation trends to retain individuals in care and higher HIV viral load suppression was determined. Nevertheless, ART initiation timing might not be a solely important factor in improving HIV care and minimizing mortality among HIV-infected individuals in a university hospital setting.
Introduction
The infection of human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) are among the most significant global health issues. In 2018, 37.9 million people were living with HIV (PLHIV), 1.7 million were newly infected with HIV, and 770 000 people died from AIDS-related illnesses. 1 Nevertheless, 13.4 million PLHIV are still unable to access life-changing antiretroviral medicines, and only 62% receive antiretroviral therapy (ART). The Joint United Nations Programme on HIV/AIDS (UNAIDS) responses for ending the AIDS epidemic by 2030. The 90-90-90 campaign, HIV test–treat–retain continuum of care, has been proposed. 2 The achievable target by 2020, 90% of all PLHIV will be aware of their HIV status, 90% of all people diagnosed with HIV infection will receive sustained ART, and 90% of all people receiving ART will have viral load suppression. Globally, in 2018, 79% of all PLHIV were aware of their HIV status, 78% of all people diagnosed with HIV infection received sustained ART, and 86% of all people receiving ART had viral load suppression. 1 In 2018, the UNAIDS reported an estimated 480 000 PLHIV in Thailand and that 6400 people were newly infected with HIV, and 18 000 people died from AIDS-related illnesses. In the same year, 94% of all PLHIV in Thailand were aware of their HIV status, only 75% of all people diagnosed with HIV infection received sustained ART, and 73% of all people receiving ART had viral load suppression. 1
Same-day ART initiation is a strategy to reduce waiting time before initiating ART to minimize mortality and loss to follow-up. 3 Some randomized trials conducted in resource-limited settings demonstrated a higher proportion of retention in care in PLHIV for whom ART was initiated on the same day of HIV diagnosis.4,5 The study in Haiti reported retention in care rates at 12 months of 79.8% in the same-day ART initiation group and 71.9% in the standard ART initiation group regardless of viral load results. 4 Furthermore, the study conducted in South Africa determined the retention in care rates at ten months of 81% in the same-day ART initiation group and 64% in the standard ART initiation group. 5 Nevertheless, there was only a shortened time of HIV viral load suppression (median 1.8 months) among individuals in the same-day ART initiation group compared to individuals in the general care group in San Francisco. The results did not disclose the difference in the retention rate in care. 3 There was no statistical difference in the mortality rate between the same-day ART initiation group and the standard ART initiation group.3–5
In a continuum-of-care analysis of the Thai National AIDS Program (NAP) from 2011 to 2014, 70% of all people diagnosed with HIV infection were retained in care. 6 Meanwhile, another study conducted in a university hospital in Thailand demonstrated that approximately 70.2% of newly diagnosed HIV-infected individuals were retained in care and the mortality rate was 1.8%. 7 To the best of our knowledge, a limited study has mentioned the effect of the timing of ART initiation and the clinical outcomes such as retention in care, HIV viral load suppression, and mortality in Thailand, where the prevalence of HIV infection is high. From the benefit of same-day ART initiation, the situation at each step of the continuum of care may be different for different population groups and countries. 8 We hypothesized that a routine HIV care system in this university hospital setting, the timing of ART initiation of approximately 14 days, does not compromise the clinical outcomes compared with late ART initiation.
Methods
A retrospective cohort study was conducted among adults (aged ≥18 years) who had the first diagnosis of HIV infection based on positive HIV antibody testing at Ramathibodi Hospital (a 1200-bed university hospital in Bangkok, Thailand) between 1 January 2015 and 31 December 2017. The data were collected during September 2018 and August 2019. Individuals were excluded if they were pregnant or previously diagnosed with HIV infection or had known positive HIV antibody testing. Anti-HIV with ARCHITECT HIV Ag/Ab Combo (Abbott GmbH & Co. KG) was used for screening. If the first test result was positive, at least two additional tests were performed, eg Determine™ HIV-1/2 Ag/Ab Combo (Orgenics Ltd), Wondfo Diagnostic Kit for HIV 1/2 Antibody (Guangzhou Wondfo Biotech Co., Ltd), and VIDAS® HIV panel (bioMérieux Co., Ltd).
Clinical and demographic data, including age at positive HIV antibody testing, gender, marital status, hometown, health insurance scheme, route of HIV acquisition, co-morbidity, reason, and timing of HIV antibody testing (date of blood collection), the timing of HIV diagnosis (date of the first physician informing the result of testing to PLHIV), the timing of HIV clinic visit, the timing of ART initiation, clinical presentations, location of HIV infection diagnosis, and antiretroviral regimen, were obtained by reviewing the medical records. AIDS-defining illnesses, immune reconstitution inflammatory syndrome (IRIS), and cause of death were also collected. Five major healthcare systems had a universal coverage program, social security, state enterprise, government office, and self-pay. The health insurance scheme might be a confounder of the timing of ART initiation. An individual who had universal coverage health insurance was feasible for ART initiation after registry to the NAP without additional costs, regardless of the primary register site. For an individual with government officials and state enterprise health insurance, ART could be initiated as early as possible at the exact location of HIV diagnosis without any registration or transfer out. In contrast, free-of-charge ART initiation was allowed only for those registered at the particular affiliate hospital for individuals with social security health insurance. Laboratory investigation results, including CD4 count, HIV viral load, and co-infection with hepatitis B virus (HBV), hepatitis C virus (HCV), or syphilis, were also retrieved and reviewed.
Continuum of HIV care was determined. Retention in care was defined as having medical records on the day of HIV viral load or CD4 count testing at 12 months after undergoing HIV antibody testing (known outcome). 9 Details regarding lost to follow-up at every step of care, such as HIV antibody testing to the diagnosis, from HIV diagnosis to visiting the HIV clinic, and from seeing the HIV clinic to ART initiation, were collected. All individuals received pre-test counseling before performing HIV antibody testing by primary physicians at every clinic in the hospital. The same physician usually performs post-test counseling when individuals return to get the testing results. If the test was positive, individuals discussed with the primary physician where to start ART depending on the health insurance scheme and their convenience. If individuals did not return to the clinic, the nurse did a phone call for rescheduling the visit as soon as possible (from Monday to Friday). If they deny returning, we did not inform the test results via phone. Lost to follow-up was defined as an individual who did not visit the HIV clinic within three months after an appointment date and did not have a documented transfer to other care facilities (unknown outcome). HIV viral load suppression was defined as a viral load less than 40 copies/mL. In the case of absent HIV viral load results, they were defined as viral load non-suppression.
The sample size for the chi-square test was calculated using 95% power to detect an effect size (W) of 0.3, where the degree of freedom was three and the significance level (alpha) was 0.05; as a result of this estimation, the sample size was 191. 10 Mean values (with standard deviation, SD) or median values (with interquartile range, IQR) and frequency were used to describe the patients’ characteristics for continuous and categorical data, respectively. Chi-square test or Fisher's exact test and Student's t-test were used to compare categorical variables and continuous variables between the two groups, respectively. Baseline characteristics of individuals were compared between the early ART initiation group (≤2 weeks) and the late ART initiation group (>2 weeks). The proportions of individuals who were retained in care who had HIV viral load suppression and died at 12 months were also compared. Factors associated with late ART initiation were determined. Univariate and multivariate logistic regression analyzes were performed to determine the factors associated with late ART initiation. Variables with a P-value <.05 were considered in a multivariate logistic regression model after assessing the multi-collinearity of variance inflation factors. Variables were selected into a multiple logistic regression model with stepwise forward selection, and those that attained a level of significance (P < .05) were retained in the model. The odds ratio (OR) and its 95% confidence interval (CI) were estimated. A P-value <.05 was considered statistically significant. All statistical analyzes were performed using the Stata statistical software version 12.0 (StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP).
Ethical Approval and Informed Consent
Ethical approval of this study was obtained from the Human Research Ethics Committee, Faculty of Medicine Ramathibodi Hospital, Mahidol University (approval number: COA. MURA2020/339). Individual consent was not required due to a retrospective study.
Results
During the 3-year study period, 195 585 HIV antibody test was performed and a total of 1078 (0.55%) individuals with positive HIV antibody results were identified. Of these individuals, 566 were already known cases of HIV infection, 22 were pregnant women, and two had missing data. The reasons for HIV antibody re-testing mostly were routine preoperative laboratory investigations and regular screening before hemodialysis individuals who were already known as PLHIV. Finally, 488 individuals were identified with newly positive HIV antibody testing at the study site. During the transfer process by the first physician contact to the HIV clinic, 98 individuals were transferred out to other healthcare facilities and 20 individuals were lost to follow-up. Of these, 83 of 98 (84.6%) individuals who were transferred out and 16 of 20 (80%) individuals who lost to follow up had self-pay health insurance schemes. Twenty-four individuals did not return after performing HIV antibody testing and were not aware of their HIV status. They were counted as undiagnosed of HIV infection. Of these, median (range) age was 44 (31-60) years, 66.7% were male, 87.5% were asymptomatic, 66.7%, and 29.2% were performing HIV antibody testing due to preoperative evaluation and clinical suspicion by a physician, respectively, and 66.7% had self-pay health insurance scheme. At the HIV clinic, 47 individuals were additionally transferred out to other healthcare facilities and 299 individuals were enrolled in the HIV clinic. Of 29 individuals for whom ART was not initiated, one individual was an elite controller, five died, and 23 individuals were lost to follow-up. The causes of death among individuals who died before ART initiation were disseminated cryptococcosis, disseminated cryptococcosis with Kaposi's sarcoma, cerebral toxoplasmosis, pneumocystis pneumonia with disseminated tuberculosis, and severe bacterial pneumonia (one each). Continuum of HIV care of individuals with newly positive HIV antibody testing during 2015 to 2017 is shown in Figure 1

Continuum of HIV care of 488 individuals with newly positive HIV antibody testing, 2015–2017.
The median (range) age of the 488 individuals with newly positive HIV antibody testing was 37 (18.3-79.8) years, 371 individuals (76%) were males, 325 individuals (66.6%) were married/couple, and 244 individuals (50%) lived in the central part of Thailand. The most common health insurance scheme was self-pay (43.4%), followed by universal coverage program (25.2%), government officer (22.5%), state enterprise (5.5%), and social security (3.2%). The two most common routes of HIV acquisition were heterosexual (42%) and homosexual (29.5%). Sixty-five individuals (13.3%) had underlying diseases diabetes mellitus, hypertension, and dyslipidemia. Based on clinical HIV diagnosis, 281 individuals (57.6%) were asymptomatic, 207 individuals (42.4%) were symptomatic, and 157 individuals (32.2%) were AIDS. Approximately one-third of individuals had AIDS-defining illnesses such as pulmonary tuberculosis (73.3%), pneumocystis pneumonia (55.8%), extrapulmonary tuberculosis (45.3%), and cryptococcosis (16.3%). The common reasons for performing HIV antibody testing were clinical suspicion by a physician (57.4%) and preoperative evaluation (31.1%). HBV, HCV, and syphilis co-infections constituted 6.1%, 2.4%, and 9.2%, respectively. Median (IQR) CD4 count at the time of HIV diagnosis was 159 (53-308) cells/mm3 (n = 324). Table 1 shows the characteristics of the individuals with newly positive HIV antibody testing.
Demographic and Baseline Characteristics of 488 Individuals with Newly Positive HIV Antibody Testing During 2015–2017.

Others: obstetrics and gynecology (n = 17), orthopedics (n = 7), psychiatry (n = 3), dentistry (n = 2), pediatric (n = 2).
Others: obstetrics and gynecology (n = 7), orthopedics (n = 1), psychiatry (n = 1), dentistry (n = 2), pediatric (n = 2).
Others: obstetrics and gynecology (n = 4), orthopedics (n = 1), psychiatry (n = 2).
Some patients might have more than one underlying disease.
The continuum of care was depicted in Figure 2. Overall, 95.1% of 488 PLHIV were aware of their HIV status, 299 (61.3%) individuals were enrolled in care, 228 (46.7%) individuals retained in care, 227 (46.5%) individuals received sustained ART, and 203 (41.6%) individuals had HIV viral load suppression. Among 299 individuals who were enrolled in care, 270 (90.3%) individuals initiated ART at the study site, 228 (76.3%) individuals retained in care at 12 months, and 203 (67.9%) individuals had HIV viral load suppression, including one elite controller.

HIV test–treat–retain continuum of care.
Of 270 who initiated ART, 227 (84.1%) individuals retained in care at 12 months and 202 (74.8%) individuals had HIV viral load suppression. Of 256 individuals who initiated ART at the study site and did not transfer out, 227 (88.7%) individuals retained in care at 12 months and 202 (78.9%) individuals had HIV viral load suppression (Table 2). Of 270 individuals for whom ART was initiated at the study site, the median (IQR) time from HIV diagnosis to ART initiation was 18 (9-30) days. Clinical characteristics and laboratory investigations between individuals in the early ART initiation group (n = 116) and those in the late ART initiation group (n = 154) are shown in Table 1. The median (IQR) time from HIV diagnosis to ART initiation was 7 (7-13) days for individuals in the early ART initiation group and 28 (21-46) days for those in the late ART initiation group. In the early ART initiation group, the proportion of HIV diagnoses at the outpatient department was higher (84.5% vs 72.7%, P = .021). In contrast, the proportion of HIV diagnoses at the emergency department was higher (16.2% vs 6.0%, P = .010) in the late ART initiation group. Individuals in the early ART initiation group had a higher proportion of having HIV antibody testing by self-testing (19.8% vs 12.3%, P = .093), lower proportions of AIDS diagnosis (19.8% vs 45.5%, P < .001), and having syphilis (7.8% vs 16.9%, P = .027) than those in the late ART initiation group. The median (IQR) CD4 count at the time of ART initiation was 179 (68-310) cells/mm3 and 162 (45-320) cells/mm3 in the early ART initiation group and the late ART initiation group (P = .329), respectively. Tenofovir disoproxil fumarate/emtricitabine/efavirenz was the most common initiation regimen in both groups.
Comparisons of Clinical Outcomes among Individuals in the Early ART Initiation Group and Those in the Late ART Initiation Group.
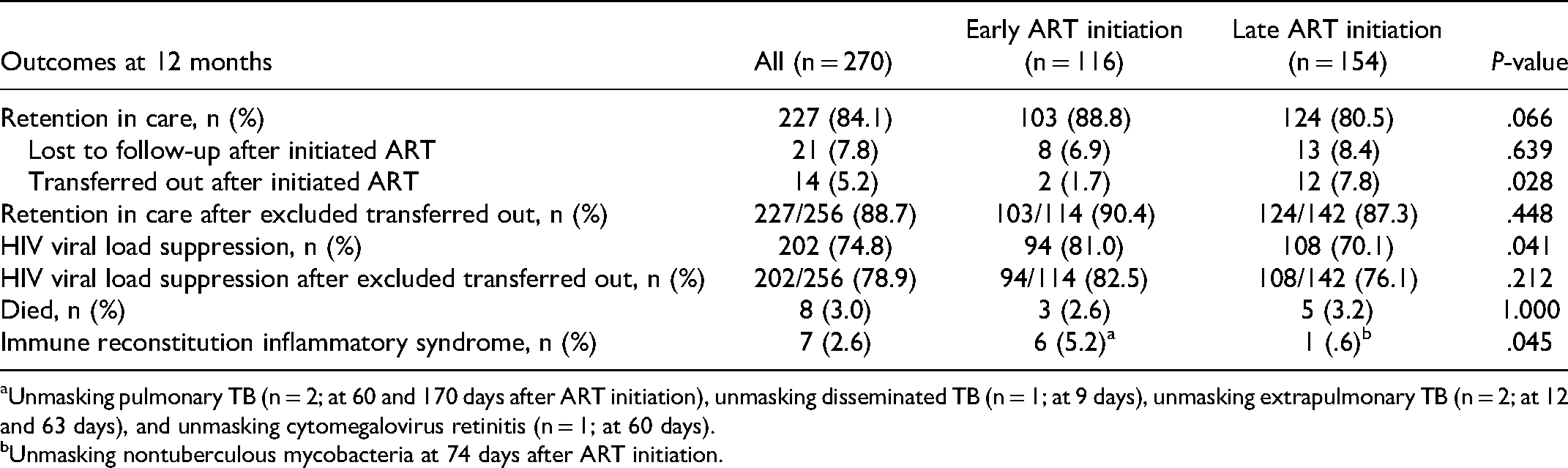
Unmasking pulmonary TB (n = 2; at 60 and 170 days after ART initiation), unmasking disseminated TB (n = 1; at 9 days), unmasking extrapulmonary TB (n = 2; at 12 and 63 days), and unmasking cytomegalovirus retinitis (n = 1; at 60 days).
Unmasking nontuberculous mycobacteria at 74 days after ART initiation.
Individuals in the early ART initiation group had a slightly higher proportion of retention in care at 12 months (88.8% vs 80.5%, P = .066) and a significant higher proportion of individuals who had HIV viral load suppression (81.0% vs 70.1%, P = .041) than those in the late ART initiation group. A higher proportion of IRIS was significant higher in the early ART initiation group (5.2% vs 0.6%, P = .045). However, there were no significant differences between the two groups in the proportion of death at 12 months (2.6% vs 3.2%, P = 1.000) (Table 2). The causes of death of individuals in the early ART initiation group were Burkitt's lymphoma (n = 2) and bacterial pneumonia (n = 1). The causes of death in late ART initiation group were NK/T-cell lymphoma (n = 1), haemophagocytic lymphohistiocytosis (n = 1), Kaposi sarcoma (n = 1), pneumocystis pneumonia (n = 1), and bacterial pneumonia (n = 1). All causes of death were not related to IRIS.
In the univariate logistic regression analysis, having pneumocystis pneumonia (OR 6.95, 95% CI 2.04-23.07, P = .002), tuberculosis (OR 3.10, 95% CI 1.61-5.98, P = .001), syphilis (OR 2.41, 95% CI 1.08-5.38, P = .031), and weight loss (OR 1.95, 95% CI 1.12-3.42, P = .019) were associated with late ART initiation. In the multivariate logistic regression analysis, having pneumocystis pneumonia (OR 9.30, 95% CI 2.56-33.75, P = .001), tuberculosis (OR 2.21, 95% CI 1.03-4.73, P = .041), and weight loss (OR 12.98, 95% CI 1.00-167.68, P = .050) were associated with late ART initiation (Table 3).
Factors Associated with Late ART Initiation Using Multivariate Logistic Regression Analysis.
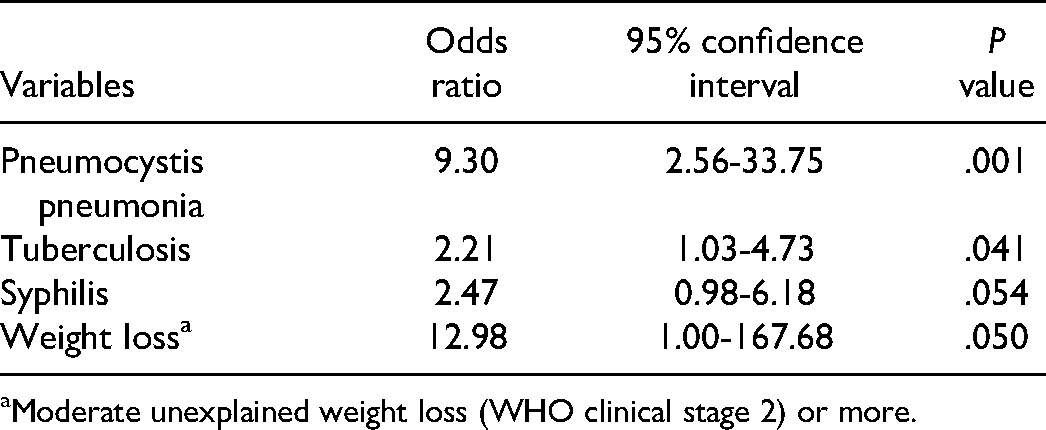
Moderate unexplained weight loss (WHO clinical stage 2) or more.
Discussion
This study observed that the median time from HIV diagnosis to ART initiation was 18 days in the university hospital setting in Thailand, where one-third of newly diagnosed PLHIV were AIDS and had low CD4 counts. We determined a difference in some characteristics and laboratory investigations between individuals with early ART initiation and those with late ART initiation. Pneumocystis pneumonia and tuberculosis were factors associated with late ART initiation, and it might be the main reasons for a physician waiting until opportunistic infections improve before initiating ART. There was no statistically significant difference in the proportion of retention in care and mortality at 12 months between the groups. The proportion of individuals with HIV viral load undetectable is approximate 10% higher in the early ART initiation group. However, this effect was attenuated after excluding transferred out individuals, and there was no statistically significant difference.
Early ART initiation is one of the several solutions to improve retention in care. The proportion of PLHIV who were retained in care was 88.8% among those for whom ART was initiated within 14 days after HIV diagnosis in this study. It is comparable with the proportion of PLHIV who retained in care in the same-day ART initiation group in randomized controlled trials, and it is higher than those of the same-day ART initiation model in Thailand.3–5,11 Additionally, in particular, clinical settings such as antenatal care, HIV testing, counseling, and ART service in the same site were more critical than same-day ART initiation. 12 Therefore, same-day ART initiation may not improve retention in every HIV care setting.
Durable HIV viral load suppression is the primary goal of HIV care. This is because ART prevents morbidity and mortality in PLHIV and prevents HIV transmission to partners and others, the so-called “treatment as prevention”.13,14 A systematic review reported a viral load suppression (thresholds set at or below 200 copies/mL) of 76.1% after 12 months of ART in low- and middle-income countries. 15 Nevertheless, the proportions of PLHIV with HIV viral load suppression in the same-day ART initiation group in clinical trials were only 53% at 12 months and 64% at ten months.4,5 In our a university hospital setting, the timing of ART initiation with a median time from HIV diagnosis to ART initiation of 18 days resulted in a high proportion of HIV viral load undetectable of approximately 80% and higher than those in the same-day clinical trial in Thailand. 11 As mentioned, the proportion of individuals with HIV viral load suppression varies across the studies. In the setting with a high percentage of PLHIV with HIV viral load suppression, the effect of timing of ART initiation (eg, same-day or early) trends not to increase the proportion of individuals with HIV viral load suppression after same-day ART initiation.
Furthermore, the mortality rate in PLHIV was low and around 3% in our study regardless of ART initiation timing. The mortality rate within one year after late initiation of ART in the TREAT Asia HIV observational database (TAHOD) of the International epidemiologic Databases to Evaluate AIDS (IeDEA) Asia-Pacific was 4.27 per 100 person-years. 16 The study conducted in Africa also reported mortality rates of 2% in the intervention group (ART initiation by two weeks after eligibility) and 3% in the control group (usual care). 17 In a recent systematic review, ART initiation on the same day demonstrated a non-significant trend towards reduced mortality (three trials: relative risk 0.53, 95% CI 0.24-1.08). 18 Overall, the mortality in PLHIV after ART initiation was relatively low irrespective of ART initiation timing. Thus, the timing of ART initiation might not reduce the mortality among PLHIV. Furthermore, we found a significantly higher proportion of individuals with IRIS in the early ART initiation group than in the late ART initiation group.
There are some limitations in this retrospective study. First, there were missing data regarding the clinical characteristics and laboratory investigations, and this was not unexpected because of the nature of a retrospective study. Some patients were transferred out after ART initiation, and we were unaware of their outcome. Second, the sample size was small, and the study was conducted in a single center. Besides, our study did not directly compare early and same-day ART initiation. Finally, the study was conducted in a university hospital setting, which might not reflect the entire picture of Thailand and other resource-limited settings where differences exist in the system and policy of HIV/AIDS care.
In contrast, this study demonstrates the real-world practice without intervention bias that may occur in the counseling process of an unblinded study. Moreover, we presume that in almost every HIV care setting in Thailand, ART initiation within two weeks is feasible and practical. We believe that there are the first few studies in Thailand and Southeast Asia concerning the effect of ART initiation timing and clinical outcomes in HIV care.
Conclusions
The median time to ART initiation was approximately two weeks in Thailand's real-world university hospital setting. Early ART initiation trends to retain PLHIV in care and a higher proportion of individuals with HIV viral load suppression were determined. However there were no differences in the mortality rate. The timing of ART initiation might not be the solution for all levels of HIV care, and widespread implementation should be concerned. ART initiation as early as possible should be implemented to reduce early loss to follow-up and HIV transmission; however, the improvement in the proportion of HIV viral load suppression and the decrease in mortality is questionable. Further research and strategies are required to improve the early detection of HIV-infected individuals and monitor long-term clinical outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.