
Abstract
The Dominican Republic (DR) has the second-highest prevalence of HIV infection in the Caribbean, but viral suppression and treatment adherence are not well understood. We conducted a cross-sectional study among people living with HIV/AIDS(PLWHA) to fill in the knowledge gap. Questionnaire was used to collect demographic data, antiretroviral therapy (ART) adherence, and barriers and facilitators to HIV care. Viral load and other clinical information were extracted through chart reviews. Descriptive analyzes and logistic regression were conducted to explore factors associated with non-viral suppression and imperfect ART adherence. Of 193 PLWHA 83.9% were virally suppressed. Those that were non-virally suppressed were more likely of being male (odds ratio [OR]: 2.55, 95% confidence interval [CI]: 1.17-5.58) and less likely of being unemployed (OR: 0.28, 95% CI: 0.08-0.96). However, being male (OR: 0.78, 95% CI:0.40-1.53) and unemployed (OR: 0.28, 95% CI:0. 08-1.21) were less likely to report imperfect adherence. Tailored interventions are needed to improve adherence and viral suppression in DR.
Introduction
The Human Immunodeficiency Virus (HIV) is a devastating infectious disease that continues to affect Low- to Middle-Income Countries (LMIC) disproportionately 1 The Caribbean region has the second-highest prevalence of HIV in the world. 2 The Dominican Republic (DR), shares the island of Hispaniola with Haiti, both countries accounted for 70% of AIDS related death in the region on 2017. 3 UNAIDS estimates the prevalence of HIV-infection to be 1% among adults aged 15 to 49 years, with about 67 000 adults and children living with HIV in the DR. 4 Efforts to increase access of antiretroviral therapy (ART) to HIV-infected individuals and improvement of social protection strategies has reduced the number of new infections by 29% in the Caribbean from 2010-2019. Key populations and their partners or sexual contacts account for 60% of those newly infected. 5
In 2004, the President's Council on AIDS, the DR Ministry of Health and international non-governmental organizations significantly scaled up the provision of antiretroviral therapy (ART) to people with HIV (PWH) in the DR. 6 Between 2004 and 2017, the incidence of HIV infections and the number of AIDS-related deaths decreased by 66% and 58%, respectively. Despite these achievements, significant progress must be made to achieve the 90-90-90 targets. Currently, only 53% of PWH have access to ART and only 43% are virally suppressed. 4
The Ministry of Public Health in the DR has established national guidelines for addressing the epidemic in the DR, which includes ending the AIDS epidemic by 2030, the provision of ART for all PWH, and reduction of new infections by 50% among key populations. 7 The HIV epidemic in the DR is characterized by several sociocultural challenges which hinder the ability of certain populations to access and adhere to HIV interventions and services. 8 Despite having the second-highest prevalence of HIV in the Caribbean, there is limited literature on the factors that impact the continuum of care among HIV-infected populations in the DR. 2
This is a cross-sectional evaluation of adherence to care and ART, and its association with HIV viral suppression on adult PWH engaged in care at an urban clinic within a public tertiary-care hospital in Santiago, DR. This study aims to understand how adherence interventions can be better targeted for patients in HIV care in the northern region of the DR.
Methods
Study Setting and Participants
A sample of adult PWH were enrolled from the Clínica de Enfermedades de Daños Inmunólogicos (CEDI; Clinic of Immunologic Diseases) between June and July 2018. CEDI is an HIV clinic located within the Hospital Regional Universitario José María Cabral y Báez (HRUJMCB), a major public tertiary-care hospital in Santiago, DR. All PWH being followed at the CEDI receive ART and medical consultations free of charge regardless of insurance status. Currently, the clinical staff at the CEDI provide several resources to promote engagement in care, including a peer navigator, a psychologist, and staff members who distribute medications.
Inclusion criteria for participants were: (1) HIV diagnosis, (2) age 18 years or older and (3) receiving antiretroviral therapy for more than 30 days. Informed consent and surveys were provided in Spanish and/or Haitian Creole by trained research staff.
Measures
The primary outcome was HIV viral suppression, defined as having an HIV viral load of less than 200 copies/mL within the last six months. Participants completed a demographics survey, a self-reported adherence assessment and a survey of barriers and facilitators. Clinical data were collected through chart review by the research staff.
Demographic information included age, sex, race/ethnicity, nationality, employment status, medical insurance, time from HIV diagnosis, as well as alcohol and drug use. The self-reported adherence assessment was based on a tool that has been validated for use both in the United States and in South Africa.9–11 Participants are asked to report the number of doses missed in the last 30 days, how well they adhered to their medications (on a scale of “Very poor, Poor, Fair, Good, Very good, Excellent”), how frequently they adhered to their medications (on a scale of “Never, Rarely, Sometimes, Usually, Almost always, Always”) and how many HIV medical appointments they had missed within the last year.
A survey of barriers and facilitators of participant's adherence to HIV care was conducted. Finally, clinical data were extracted from the paper medical records, including most recent viral load, ART regimen prescribed, previous ART prescribed, and presence of psychiatric or medical co-morbidities.
Statistical Analysis
Bivariate analyzes were performed to present the distribution of demographics between participants who were virally suppressed (<200 copies/mL) and those who were not virally suppressed (>200 copies/mL). Chi-square tests and Kruskal-Wallis rank tests were used for categorical and continuous variables, respectively. Multivariate logistic regressions were conducted to explore risk factors associated with being not virally suppressed or reporting imperfect adherence. Confounding variables were determined by a priori knowledge. This analysis was conducted using Stata 15.0 (StataCorp, Texas).
Ethical Approval and Informed Consent
The study protocol was approved the Miriam Hospital Institutional Review Board (IRB) in Providence, RI (Review #210218) and the Ethics Committee (EC) at HRUJMCB in Santiago, DR. Both the IRB and EC waived the need for a written informed consent since the only record linking the subject and the research would be the consent document and the principal risk would be potential harm resulting from a breach of confidentiality. Informed consent was obtained verbally before participation and confirmed by an independent witness.
Results
During June and July 2018, 202 PWH were surveyed. 193 (95.5%) had clinical chart data available to review and were included in the analysis. The characteristics of the study population are presented in Table 1. The majority of PWH were women (61.1%), of Dominican nationality (90.1%), uninsured (76.6%), and employed (73.6%). Most participants were in the age group of 35-54 years (59.6%). These characteristics compare to those of the overall CEDI clinic whose HIV patient population is 53% women, 95% of Dominican nationality and has a median age of 47 years. Nearly half (47.4%, n = 90) of participants reported having 0-6 years of education, while 42.1% (n = 80) had completed 7-9 years of education. About half considered they lived far away from the HIV clinic (49.2%, n = 95). More than half of PWH reported the cost of transportation was expensive for them (53.4%, n = 103). Most patients stated never (59.1%) or rarely (18.1%) using alcohol in the last month.
Demographic Characteristics of the Study Participants (N = 193).
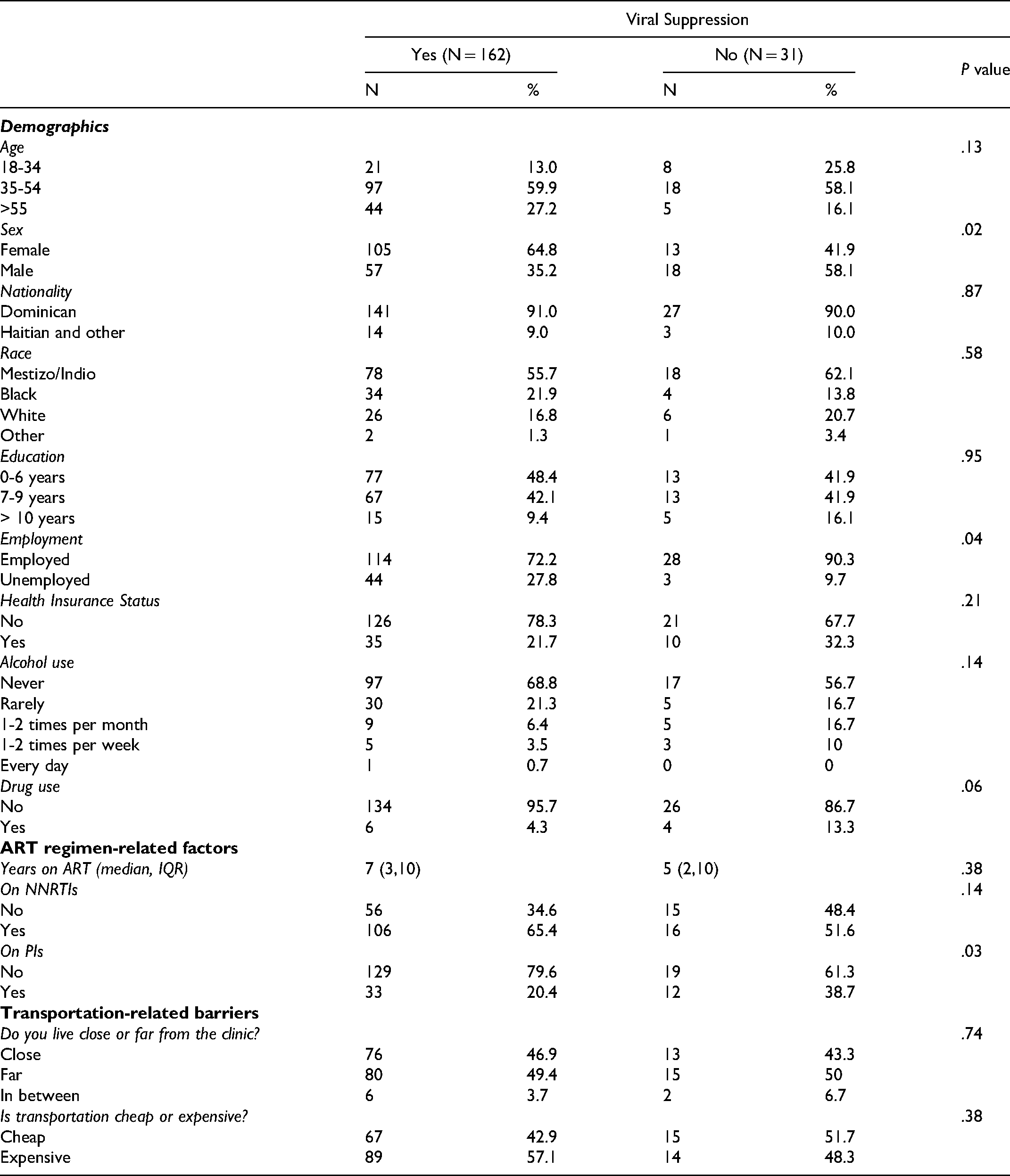
Of the 193 study participants, 83.9% (n = 162) had achieved HIV viral suppression (HIV RNA viral load < 200 copies /mL). Factors that had a negative impact on HIV viral suppression included being male (P = .02), employed (P = .04) or prescribed a protease-based inhibitor containing regimen (P = .03). Marginal statistically significance was observed for years of taking ART and a history of drug use. Patients who achieved viral suppression tended to have a longer time period of taking ART than those who were not viral suppressed. (Median: 7 years vs 5 years, interquartile range (IQR):3-11 years versus 2-10 years; P = .08). A history of drug use was associated with viral non-suppression (P = .06).
Logistic regression analysis of HIV viral suppression shows that males were 155% more likely (crude odds ratio (OR): 2.55, 95% confidence interval [CI]: 1.17-5.58) to be virally non-suppressed than females. Those who were virally non-suppressed were 72% less likely (crude OR: 0.28, 95% CI: 0.08-0.96) to be unemployed. When adjusting for male sex, employment had a marginally significant effect on viral suppression (adjusted OR: 0.32, 95% CI: 0.08-1.21. (Table 2a)
Multivariate Analysis of Viral Suppression (2a) and Imperfect Adherence (2b).

ORs adjusted for age, race, and sex.
Logistic regression analysis of imperfect adherence shows that males were 22% (crude OR: 0.78, 95% CI: 0.40-1.53) and unemployed participants were 72% less likely (crude OR: 0.28, CI: 0.08-0.96) to report missing at least 1 dose of their ART. When adjusting for male sex, employment did not have a significant effect (adjusted OR: 0.79, 95% CI: 0.31-2.01). Those in older age groups were also less likely (35-54 years, crude OR: 0.27, 95% CI: 0.12-0.61; 55 + years, crude OR: 0.16, 95%CI: 0.06, 0.45) to report imperfect adherence than younger patients in the 18-34 age group. (Table 2b)
Self-Reported Treatment Adherence
PWH who achieved viral suppression were statistically more likely to rank their adherence positively as compared to those who had not. Among those who reported never missing a single dose in the past 30 days, most were virally suppressed, but 14.7% were not. (Table 3)
Outcomes from Self-Reported Treatment Adherence Tool.

On average, participants who missed fewer HIV appointments were more likely to be virally suppressed (P = .001). After adjusting for employment, those with missed appointments were still less likely to have HIV viral suppression (adjusted OR: 2.28, 95% CI:1.40-3.72).
Perceived Barriers and Facilitators
The structured interview questionnaire also provided insight into the most common barriers and facilitators that participants reported were relevant to their ability to adhere to their HIV care and ART.
Table 4 shows the top 10 barriers and facilitators reported by the 202 participants that participated in this survey. The most common barriers were related to lack of confidentiality concerns, structural barriers and stigma. The most prevalent barrier reported was concern for privacy (n = 111), but feelings of shame and embarrassment (n = 77) and feeling afraid that their family would find out their HIV status (n = 74) were common stigma- and confidentiality-related barriers. Many patients also expressed feeling anxious or depressed (n = 74). Challenges associated with transportation to the clinic were also relatively common, such as lacking money for transportation (n = 85), not being able to get to the clinic due to strikes within the transportation system (n = 45) or that their appointments were inconvenient (n = 48).
Reported Barriers and Facilitators to HIV Care.

When asked which factors helped them remain engaged in care, participants most often reported that it was important for them to take care of their health so that they would not feel worse (n = 171), to be able to take care of their children (n = 119), or to maintain their CD4 count and viral load (n = 118). Acceptance of their diagnosis (n = 100) and less concern with issues relating to privacy (n = 100) were also reported to have a positive impact. Finally, a significant proportion of participants indicated the following facilitators: acknowledgement of the importance of seeing a health care provider (n = 106), ability to get money for transportation (n = 86) and more convenient appointment scheduling (n = 73). (Table 4)
Discussion
In this study, we conducted a self-reported adherence assessment, a survey of barriers and facilitators, and a chart review in order to evaluate factors associated with viral suppression among adults living with HIV engaged in care at CEDI in Santiago, DR. Of patients enrolled in this study, 83.9% had a viral load less than 200 copies/mL. Patients that were not virally suppressed were significantly more likely to be male, taking second-line regimens such as protease inhibitors, miss follow-up appointments or be currently employed. These findings may help to tailor interventions for PWH who may benefit from additional support to remain engaged in care.
The global standard of HIV care is universal access to ART, which has significantly increased life expectancy and decreased mortality and morbidity caused by HIV.12,13 The Treatment as Prevention (TasP) model, which now informs HIV prevention strategies worldwide, suggests that achieving high rates of viral suppression by scaling up access and adherence to ART among PWH may significantly reduce future transmission, since undetectable means untransmissible (U = U). 14 The potential success of the TasP framework relies on individual patients achieving and sustaining viral suppression through adequate adherence to ART and consistent engagement in HIV care. 15 However, achieving stable compliance to ART regimens within the cascade of HIV care remains a significant challenge, particularly in resource-limited settings. 16
We found that there are multifactorial barriers and facilitators that influence patient's engagement in care, even if they are virally suppressed and report excellent adherence. Social factors including stigma, lack of social support and confidentiality concerns as well as structural factors relating to transportation and more convenient appointments.
Our finding that male patients are less likely to be virally suppressed is consistent with other studies that have shown that male patients have decreased engagement in HIV care in the DR and the greater Caribbean region.17,18 In this study, male patients constitute only 38.8% of this study population, but they represent close to half of the total number of PWH in the DR and 47.2% of all patients at CEDI. Male patients might encounter additional barriers to accessing care, which may not be fully represented here given that our sample population consisted of patients who were in the clinic for an appointment or to pick up medications from the pharmacy and that were willing to participate.
This study showed that employed PWH were less likely to have an undetectable viral load. This may be related to fear of discrimination and/or stigma from their employer as well as having limited time off to attend appointments. In qualitative studies of PWH in the DR, many participants described experiences of stigma and discrimination in employment settings due to their HIV status, including job loss, illegal HIV testing by employers and other stigma-related barriers.19,20 Additionally, many patients in this study reported that transportation to the clinic was a major barrier due to cost and logistical complications. This effect may be even greater since we used a convenience sample of those patients who were already at the clinic, so we could not assess those patients for whom transportation was preventing them from accessing care in the first place. An evaluation of an adherence intervention in La Romana, DR revealed that transportation and work schedule conflicts are important factors in achieving persistent adherence, and future studies should explore the association between transportation barriers and loss to follow-up in order to capture those who are most at risk for poor adherence. 21 In contrast, some studies have shown employment to be a protective factor for viral suppression, suggesting a complex relationship between employment status, stigma and clinical outcomes. 17
We identified that PWH prescribed PI-based regimens were less likely to achieve HIV viral suppression which has not been previously reported in the literature from the DR. Patients who are on second-line regimens are more likely to be at risk for virologic failure due to existing difficulties with ART adherence and possibly undiagnosed drug resistance.22–24 Other contributing factors include the greater pill burden, more complicated dosing schedules, and higher rates of adverse effects known to be associated with PI-based regimens.25,26 Access to genotype testing is limited for PWH in the DR, and ART regimens are frequently changed based on HIV disease progression, lack of viral suppression and the availability of medications in the hospital pharmacy. The rate of virologic failure to certain ART regimens due to drug resistance is unknown, though one small study detected at least one antiretroviral class mutation in 54% of samples from the DR, with 24% of patients having multi-class resistance. 23
The DR Ministry of Health has updated the national HIV treatment guidelines, and in 2019 Dolutegravir was included and made available as a first-line agent in combination with a dual nucleoside reverse transcriptase inhibitor (NRTI) backbone. This once-daily combination regimen has been shown to have improved efficacy, tolerability and is particularly important given that some low- and middle-income countries report a pretreatment drug resistance to Efavirenz of over 10%. 27 Other treatment regimens that are being evaluated for low-income countries to improve adherence and tolerability, and limit pill burden include long-acting injectable cabotegravir-rilpivirine which has shown on modeling studies to be cost-effective in PWH with an HIV VL of more than 1000 copies/mL but there is concern for potentially inducing integrase inhibitor resistance.24,28
This paper complements the literature to help characterize common barriers to HIV care among people living with HIV in the DR and the greater Caribbean region. Risk factors for non-adherence to ART found in other urban regions of the DR (Santo Domingo and Puerto Plata) included heavy alcohol use, having children and perceptions of less social support. 29 Previous research has also found that stigma and fear are common barriers to people seeking HIV care in the DR, and that certain populations may be more affected as a product of the reinforcement of existing prejudices in the Dominican society, especially anti-Haitianism and gender inequality.18,30,31 In addition, ongoing socioeconomic challenges related to the high levels of poverty in the DR are significant barriers to access to HIV care.29,31
Individuals of Haitian descent who are living with HIV in the DR may be at risk for worse outcomes due to both HIV-related stigma and the generalized discrimination they face in Dominican society. 25 According to the 2020 PEPFAR report, the HIV prevalence in this group ranges between 3-5% which is even higher than the reported HIV prevalence of 2% in Haiti, per UNAIDS in 2018. 32 Haitian patients constituted about 10% of our study population and had a slightly higher (though not statistically significant) rate of having a detectable viral load. 24 Among those that reported being Dominican we did not assess if they were of Haitian descent. Additional research and interventions are needed to better address the structural racism that persons of Haitian descent face and its impact on their HIV care. Other ‘key populations’ within the DR include those living in rural Bateye communities, gender and sexual minorities (men who have sex with men and transgender individuals), and individuals involved in sex work.18,29,33–35
In this study, only HIV patients who were visiting for their clinic appointment or to pick up their medications were able to be assessed, so they may not be fully representative of the population of PWH in the DR. However, this “real world” sample provides a snapshot of those who are accessing care at a public hospital.
There is a need for alternative methods of assessing HIV viral suppression in settings with limited laboratory resources. We analyzed whether a validated tool could correlate with HIV viral suppression. While the results reported here show an association between levels of optimal self-reported adherence and viral suppression, the adherence tool missed some cases of an unsuppressed viral load when participants reported high levels of “Excellent” adherence or “Always” taking their medications as prescribed. However, patients who report anything except “Excellent/Very Good” or “Always/Almost Always” were much more likely to have a detectable viral load (VL > 200 copies/mL).
Of the questions asked in the adherence assessment, endorsing having missed appointments, had the strongest association with not being virally suppressed. Those who had missed appointments recently were less likely to be virally suppressed (P = .0001). This is consistent with other studies showing that keeping scheduled clinic appointments correlates with clinical indicators of HIV outcomes. 21
A short adherence assessment may be a helpful tool to prompt an adherence discussion with peer navigators, closer follow up with a clinician, or other relevant interventions. However, social desirability bias may play an important role in responses to the self-reported sections of this survey, and this tool likely overestimated patients’ actual adherence. While neither self-reported adherence nor viral load are perfect indicators of patient's true adherence, using both can provide insight into patient's response to their ART regimens.36,37
Conclusions
With the initiative to adopt Treatment as Prevention models to end the HIV epidemic around the world, identifying and addressing challenges related to adherence and viral suppression are crucial to both individual patient outcomes and the future of the HIV epidemic on a larger scale. Future studies in the DR ought to investigate how to better support those who may be at highest risk for HIV virologic failure due to difficulties with retention in care, ART adherence and acquired ART resistance to develop effective interventions.
Footnotes
Acknowledgement
This research was supported in part by NIH/NIAID R25AI140490. We would like to acknowledge Rachaell Diaz and Brittnie Miles for their contributions to conduct this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.