
Abstract
Even though there are advancements in the treatment of patients with HIV, many deaths are related to undernutrition. Despite this fact, the burden of undernutrition and associated factors among adults receiving ART is a significant shortcoming in the study area. A cross-sectional study was done in public hospitals of the Bench-Sheko zone. Face-to-face interviews were used to gather information. Odds ratio with a 95% confidence level was used to identify determinants of undernutrition. The proportion of undernutrition, normal, and overweight were 29.2%, 61.2%, and 9.6% respectively. Food insecurity, poor ART adherence, low CD4 count, and substance use were factors associated with under nutrition among HIV patients. Undernutrition was so high in comparison to other studies in Ethiopia; the local concerned bodies should focus on identified risk factors for improving HIV/AIDS treatment via health education, nutritional assistance and counseling.
Introduction
Human Immunodeficiency Virus (HIV) continues to be a major global public health issue. According to the Joint United Nations Programme on HIV/AIDS (UNAIDS) report in 2021, an estimated 37.7 million people were living with HIV with a global prevalence of 0.7% among adults. The vast majority of HIV cases are located in low- and middle- income countries. 1 The most affected Africa region was East and Southern Africa with 20.6 million people living with HIV and 670 000 new HIV infections in 2020. 2 The World Health Organization (WHO) African region remains most severely affected, with nearly 1 in every 25 adults (3.6%) living with HIV and accounting for more than two-thirds of the people living with HIV worldwide. 3 Ethiopia is among sub-Saharan Africa which profoundly affected by the Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) and related conditions with the adult HIV prevalence ranges 1.5 in 2011 to 1.1% in 2016.4,5
Human nutrition and HIV/AIDS are closely linked to each other, both of which can independently cause progressive immune system damage. Malnutrition worsens the situation by hastening the progression of HIV infection to AIDS. HIV/AIDS is frequently linked to biological and social variables that impair people's ability to eat and use food. 6 Despite significant progress in boosting HIV/AIDS treatment coverage in recent decades, the high burden of HIV/AIDS and undernutrition have remained key health-care system challenges in SSA. 7
Undernutrition is commonly associated with HIV/AIDS than the general population.8,9 There are multi-factorial causes of undernutrition in patients with HIV/AIDS. These includes food consumption disorder, medications that cause loss of appetite, nausea and vomiting, anorexia, opportunistic infections, diarrhea, nutrient mal absorption of nutrients and wasting syndrome. 10 In addition, HIV has a particular impact on nutritional status by increasing energy requirements through metabolic and oxidative changes. Adult patients with HIV/AIDS require 10% more energy consumption when asymptomatic, 20–30% more when symptomatic and increased energy intake by 30% during the recovery period compared to healthy people. 11
It is revealed that death is higher among adult HIV positive and undernourished patents. 12 Undernutrition among HIV infected clients is often preventable, but recovering is difficult particularly those who are wasted, need more protein, and micronutrient intake to increase a weak-ended immune system. 13 Despite significant progress in the reduction of adult malnutrition, it remains a widespread public health problem of Ethiopian adults, with 33% of Ethiopians aged 15 to 49 exhibiting undernourishment. 14
The prevalence of undernutrition among HIV-infected individuals was 19% in Tanzania, 15 10% in Zimbabwe, 16 19.34% Cameron. 17 In Ethiopia, the prevalence of undernutrition among HIV/AIDS patients receiving Anti-retroviral Therapy (ART) ranges from 12.3% to 46.8%.13,18–24 Moreover a meta-analysis study revealed that the pooled prevalence of undernutrion among adult HIV positive individuals was 26%. 25 Different studies in different parts of the world revealed the factors associated with undernutrition were age, sex, marital status, unemployment, poor medication adherence, anemia, difficulty of accessing food, advanced WHO HIV stage, Cluster of differentiation 4 (CD4) count, tuberculosis, household food insecurity, ART duration, diarrhea, chat chewing, smoking tobacco bedridden or ambulatory.13,17–19,21,22,25–27
Despite many studies have been conducted in Ethiopia to investigate malnutrition among adult HIV positive individuals,13,18–19,21–23,28–31 no large-scale investigation involving a number of health facilities encompassing wide population areas and socio-cultural diversity has been done. Moreover the previous study does not assess the food insecurity level of the patients. Additionally the findings of this study will help as an input for the local governmental and non-governmental organizations who are working in the area of malnutrition and HIV/AIDS. So the present study aimed to assess undernutrion and associated risk Factors among Adult HIV/AIDS patients attending ART at public hospitals of Bench-Sheko zone, Southwest Ethiopia”.
Methods
Study Design, and Setting
From November 2020 to November 2021, a facility-based cross-sectional study was done in public hospitals of the Bench-Sheko zone of south-western Ethiopia. The administrative town of Bench-Sheko zone, Mizan Aman, is located 585 kilometers southwest of Addis Ababa. The zone has three public hospitals, namely Chena, Sheybench and Mizan Tepi university teaching hospitals, 26 health centers and 128 health posts. The main food crops of the Bench-Sheko zone include maize, coffee, godere (taro root), and enset, while sorghum, teff, wheat and barley are cultivated to a significant extent. An average of 3540 HIV positive individuals were attending ART among the three public hospitals, of which 1965 males and 1575 were females. Counseling, tracing, ART treatment, nutritional, and medical treatment are all available at the clinic.
Populations
All adults living with HIV/ADIS who are attending ART at public hospitals of Bench-Sheko zone were the source population. All adults living with HIV/ADIS who are attending ART and fulfill the eligibility criteria during the study period at public hospitals of the Bench-Sheko zone were the study population.
Eligibility Criteria
All HIV positive aged 18 years and older, who are attending ART at public hospitals of the Bench-Sheko zone, were included in to the study. An individual who was critically ill, having hearing impairment and severe mental illness at the time of the study were excluded.
Sample Size Determination and Sampling Technique
The sample size was calculated using a single population proportion calculation with a 95% level of confidence, a 5% margin of error, and a 5% non-response rate. The estimated prevalence of undernutrition among patients on ART (46.8%) was utilized to reach the maximum sample size in a study conducted in Jimma University Teaching Hospital in south west Ethiopia, 16 As a result, the total sample size was increased to 402 people.
The Bench-Sheko zone has three public hospitals namely; Mizan-Tepi university teaching hospital, Chena and Sheybench hospitals providing ART service were included in this study. An average of 3540 HIV positive individuals (1650 from Mizan-Tepi university teaching hospital, 754 from Chena hospital and 1136 from Sheybench hospital) were attending ART. A proportionate number of samples were assigned to each hospital ART clinic based on the overall number of ART customers in each public hospital. After proportional allocation the study participants were chosen using a systematic sampling procedure from three hospitals. The skip interval (k = 3540/402 = 9) was determined. The first research subject was chosen by a lottery method, then the other study participants were selected every nine intervals.
Variables
Undernutrition was the dependent variable, while the independent variables were socio-demographic variables (sex, residence, age, educational status, occupation religion, ethnicity, and income), Clinical factors (HIV related) factors (diarrhea, duration of antiretroviral therapy, CD4 count, viral load, WHO staging, TB treatment, ART adherence, hemoglobin level), Behavioral factor (alcohol use, substance use, and extra sexual partner) and vulnerability characteristics(household food consumption, food aid) were the independent variables.
Measurements and Operational Definitions
Data Collection Tools and Procedures
A pretested and organized interviewer-administered questionnaire, checklist, and measurements were used to gather data. Three nurses and one public health professional were recruited as data collectors and supervisors respectively. The questionnaires included socio-demographics, clinical factors, household and behavioral characteristics.
The nutritional status of the study participants were determined by anthropometric measurements by using Body Mass Index (BMI). The weight of the study participants was determined using a beam balance with a measurement range of up to 120 kg and a precision of 0.1 kg. Weight was taken while wearing only light clothing and no shoes. Before weighing each participant, the calibration was done by setting the scale to zero. The respondents' heights were measured using a vertical height scale in the middle of the board, standing upright, and recorded to the nearest 0.5 cm. The participants were instructed to remove their shoes, stand tall, and look straight down in the horizontal plane. BMI was then calculated by multiplying the weight in kilograms by the square of the height in meters (kg/m2). As a result, if the study participants' BMI was less than 18.5 kg/m2, they were classed as undernourished (underweight). 32
The Household Food Insecurity Access Scale (HFIAS) was used to assess household food security, 34 which was validated by Food and Nutrition Technical Assistance (FANTA). The Morisky Medication Adherence Scale (MMAS-8) was used to assess the patient's drug adherence. 33 ASSIST which is a brief screening questionnaire developed by the WHO to find out about people's use of psychoactive substances was used to assess current and ever substance use history of the participants. 35
Data Quality Assurance
Data collection tool was initially prepared in English translated to local language Amharic and back-translated into English to check its consistency. A pretest was done among 5% of study sample size and training was provided to the data collectors and supervisors on the objective of the study, maintenance of ethical standards, and methods of data collection. A supervisor checked the completeness of the collected data daily and overall data collection was monitored by investigators. Also data completeness were checked before enter into Epi-data 3.1. Cross-checking printout data for probable inaccuracies served as the basis for data coding and cleaning. Furthermore, descriptive analysis was used to check for missing values and outliers.
Data Processing and Analysis
Data were cleaned and entered into Epi data 3.1 and then exported to SPSS version 24 for statically analysis. The descriptive statistics were presented in frequency, tables and graphs. Normality assumption was checked for continuous variables. The BMI was computed by multiplying the weight in kilograms by the square of the height in meters. Undernutrition was defined as a BMI of less than 18.5 kg/m2.
To choose a candidate variable for multivariate logistic regression, bivariate logistic regression was used to investigate the relationship between undernutrition and each covariate. Multiple logistic regression analysis was used to find independent predictors of undernutrition using variables with a P value of less than 0.25.
The model was built using a backward likelihood ratio with a 0.1 probability of removal. The Hosmer Lemshow goodness of fit test, which considers good fit at P-value > 0.05, was used to verify the final model's goodness of fit. Finally, independent predictors of undernutrition were identified using a P-value 0.05 cut-off point, and the strength of the link was evaluated using AORs with their respective 95% confidence levels.
Ethical Approval and Informed Consent
The study was approved by Mizan-Tepi University research Institutional review board (IRB) (Ref No: MTU/20/45/8/35/11), Then, relevant offices were communicated for their cooperation with formal letter issued by the review board. Written informed consent was obtained from the study participants for data collection, but the consent for publication was not applicable. Privacy during interview and confidentiality of collected data has been securely maintained.
Results
Socio-Demographic Characteristics
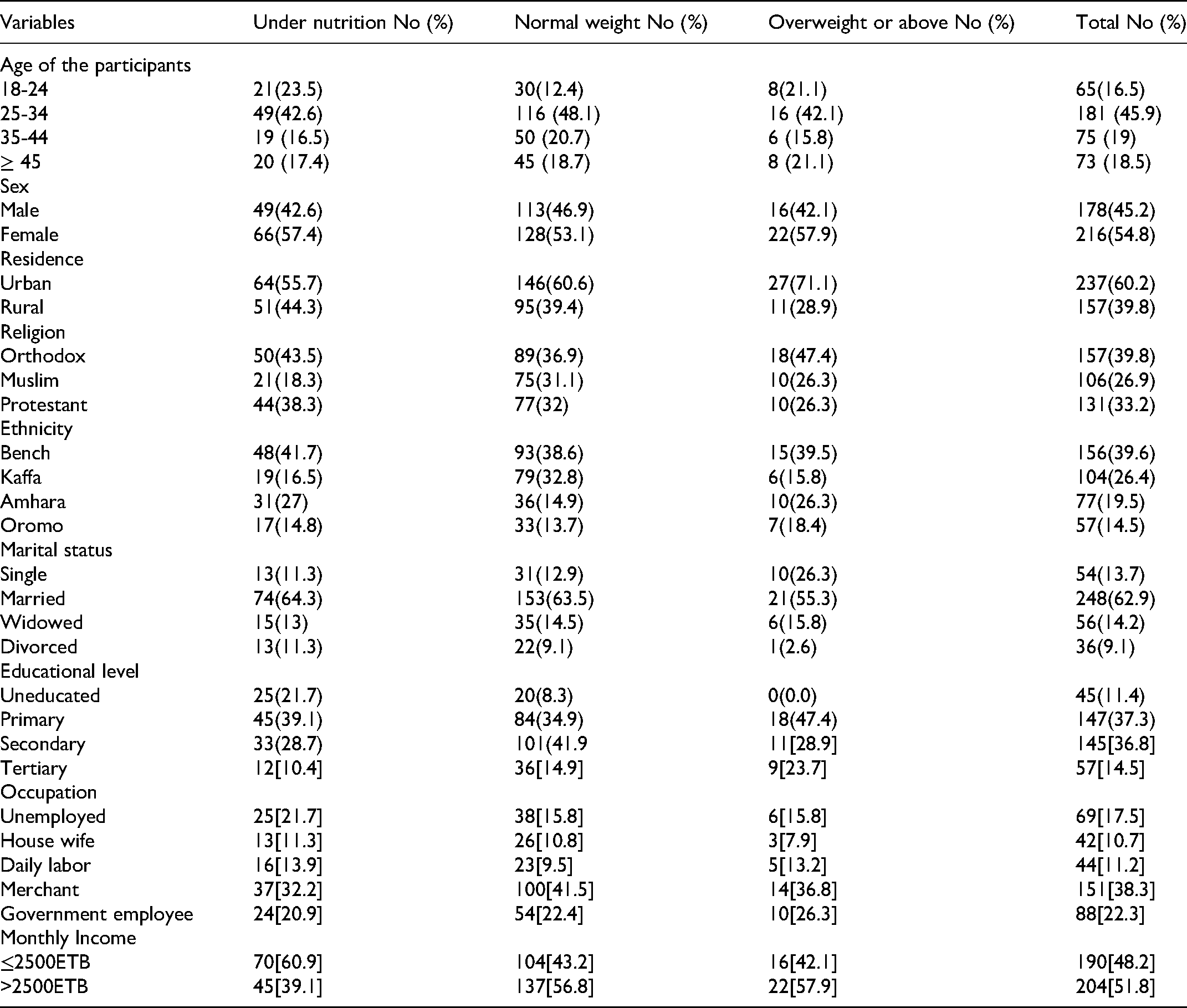
A total of 314 adult HIV-positive patients who were enrolled in ART clinics took part in the study, with a 100% response rate. The mean BMI (SD) and age of the participants were 19.9 (2.9), 34 11 respectively. The majority of the participants, 181 (45.9%), were between the ages of 25 and 34. More than half of 216 (54.8%) and about 237 (60.2%) were female in sex and urban in residence. Nearly Similar proportion 157 (39.8%) and 156 (39.6%) were Orthodox in religion and Bench in ethnicity. Concerning to marital status about 248 (62.9%) were married and about 145(36.8%) of the participants were completed their secondary education (see Table 1).
Socio-Demographic Characteristics of Patients with Their Nutritional status (BMI) in Bench-Sheko Zone Public Hospitals, Southwest Ethiopia, 2020.
Clinical and Behavioral Related Characteristics
Most of the participants 231(58.6%) were diagnosed for HIV ≥ 2 years and about 165(41.9%) had more than one year ART duration. Lightly above three-fourth 303(76.9%) had good ART adherence. The mean (SD) level of hemoglobin and CD4 count of the participants were 12.2(1.3) mg/dl and 243(18.4) cells/mm3 respectively. About 274(69.5%) of the participants had got food aid. Concerning to the behavioral characteristics nearly one-fourth 106(26.9%) were currently substance user and about 167(42.4%) had history of extramarital sex (Table 2).
Clinical and Lifestyle-Related Characteristics and Nutritional status [BMI] of Adults Receiving ART at Bench-Sheko Zone Public Hospitals, Southwest Ethiopia, 2020.

Prevalence of Malnutrition
The proportion of under nutrition (BMI<18.5 kg/m2), normal nutrition (BMI 18.5-24.9 kg/m2) and overweight or obese (BMI≥25 kg/m2) patients were 29.2% [95% CI :(24.6-33.5)], 61.2% [95% CI: (56.5-66.3)], and 9.6% [95% CI: (6.6-12.9)] respectively. Out of under nutrition patients, severe malnutrition (BMI<16 kg/m2) accounted of 5.6% (Figure 1).

Nutritional status of HIV/AIDS patients on follow-up care in bench-sheko zone public hospitals, southwest Ethiopia, 2020.
Predictors of Undernutrion
Four variables were shown to be independently linked with under nutrition among Adult HIV positive persons attending ART, out of a total of 12 candidate variables incorporated into multivariable analysis. Undernutrition was about three times [AOR: 3.26, 95% CI: (1.79-5.92)] more likely among patients who had food insecurity than who had not.
The odds of under nutrition were four times [AOR: 4.22, 95% CI: (1.47-12.14)], higher among HIV patients who had poor ART adherence. HIV/AIDS patients with CD4 cell count ≤ 200 cells/mm3 were nearly six times [AOR: 5.73, 95% CI: (2.45-13.13)], more likely under nourished than patients with CD4 cell count ≥ 500 cells/mm3. Moreover individuals who were substance user is about four times [AOR: 4.11, 95% CI: (2.31-7.30)], higher risks of developing under nutrition as compared to who did not use (see Table 3).
Multivariate Associations of Different Variables with Under Nutrition among HIV/AIDS Patients on Follow-up Care in Bench-Sheko Zone Public Hospitals, Southwest Ethiopia, 2020.

Key
Discussion
Undernutrition (BMI <18 kg/m2) was prevalent in 29.2% of the population, severe undernutrition (BMI <16 kg/m2) accounted for 9%. Furthermore, food insecurity, CD4 count, ART adherence, and current substance use were identified as independent predictors of undernutrition.
The prevalence of undernutrion was consistent with 30% in the east Harerge zone hospitals, 19 25.2% in Butajira hospital, 29 and 27% in Nekemte referral hospital 31 studies in Ethiopia, however the prevalence was lower than 60.2% in west Gojam zone public hospitals, 23 46.8% in Jimma University specialized hospital, 21 and 43% in southwest Oromia region 20 studies in Ethiopia. It was higher than 12.3% in Dilla university hospital, 30 and 18.2% in Arba Minch area public health facilities 21 studies in Ethiopia, 19.5% in Tanzania, 36 10% in Zimbabwe, 25 and 19.2% in Senegal. 26 The variation observed between this and other studies could be due to discrepancy in health care awareness of the community, healthcare services utilization and the sample size difference. Besides, it might be due to the difference in socio-economic and lifestyle factors across the study participants.
In this study, food insecurity was statistically significantly associated with undernutrition. HIV patients with food insecurity had 3.3 times increased odds of developing undernourished as compared to their counterparts. This finding was consistent with studies done in East Hararge Zone hospitals of Ethiopia and Senegal19,26 found that patients with household food deficiency had higher risks of undernourishment. This may be due to the shortage of food to satisfy nutritional requirements for productive and healthy living, contributing to macro and micronutrient deficiencies.
The strong association was found between CD4 count and undernutrion. Patients with a CD4 count of < 200 cells/mm3 were approximately six times more likely to develop undernutrition than those with a CD4 count of > 500 cells/mm3. This finding was supported by studies done in Jimma of Ethiopia, Senegal, and Tanzania,22,26,36 in which undernutrition was significantly associated with lower CD4 counts. On the contrary, the study done at Dilla University Hospital, Ethiopia indicate that CD4 has no major impact on nutrition. 30 The discrepancy could be due the cultural variation of the study populations and the time in which the studies were conducted. 19
ART adherence was statistically associated with undernutrition. HIV patients who had poor ART adherence had 4 times increased odds of developing undernutrition compared to those who had good ART adherence. This finding was supported by studies done in Senegal and Ethiopia26,31,37 revealed patients who had good ART adherence had less likely to develop undernutrition. This may be due to poor ART adherence leads to viral replication, destruction of CD4 cells, compromised immunity, and advanced disease progression; finally leads to reducing the dietary intake and nutrient absorption. 28
Current substance used was significantly associated with undernutrition. Patients who use any substance in the last three months for non-medical purpose were 4 times more likely to develop undernutrition as compared to those who had not used. This finding was supported by studies done in Arbamnch, Ethiopia and Canada showed that current tobacco-smoking adults enrolled in ART programs were at higher risk of being undernourished.17,21 On the contrary, a study in Nepal showed behavioral factors like alcohol and smoking were found to have no association with under nutrition. 27 The possible differences may be due to difference in study population, behavioral characteristics and educational background.
Conclusion and Recommendation
The prevalence of malnutrition was found to be high in this study as compared to other Ethiopian environments. Food insecurity, poor ART adherence, CD4 cell counts ≤ 200 200 cells/mm3, and substance use have all been linked to under nutrition among adults HIV/AIDS patients attending ART.
Based on our findings, we suggest that all HIV-positive adults be tested for nutritional status during antiretroviral therapy, and counseling, supplementation, and nutritional treatments be tailored to HIV-positive adults with food insecurity, poor ART adherence, CD4 cell counts below 200 cells/mm3, and drug use. Further interventional trials will be conducted to determine the impact of these factors on the treatment outcomes of HIV-positive adults who are malnourished.
Limitation of the Study
The data is cross-sectional, making it impossible to draw judgments regarding the direction of relationships between research variables.
Footnotes
List of abbreviations
Acknowledgments
Our heartfelt thank goes to Mizan Tepi University for financial support. Our thanks also goes to Bench-Sheko Zone hospitals staffs for the provision of necessary information to the study area.
Moreover, we would like to thank study participants who voluntarily participated in this study.
Authors’ Contribution
All the authors wrote the protocol, participated in data collection, analyzed the data and wrote the manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials
The datasets created and analyzed during the study will be made available to organizations and individuals by the first author based on fair request.
Consent for Publication
Not applicable
Declarations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was not funded by any organizations.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.