
Abstract
As antiretroviral therapy (ART) becomes more available to the HIV-infected population, it is important to determine the prevalence of its long-term complications. In this cross-sectional study, 145 HIV-positive patients on ART, 146 HIV-positive patients not on ART, and 72 HIV-negative individuals visiting the Namakkal District Head Quarters Hospital, Tamil Nadu, India, were recruited from February 2007 to April 2009. Among the patients on ART, the prevalence of lipodystrophy was 60.7%; 22.7% with lipohypertrophy, 51.1% with lipoatrophy, and 22.7% with mixed pattern. The proportion of patients with dyslipidemia was significantly higher in the treatment group when compared to ART-naive and HIV-negative controls (P = .00). Total duration of ART was significantly associated with lipodystrophy (P = .04) and dyslipidemia (P = .01). Also, by logistic regression, abnormal metabolic levels were a risk factor in lipodystrophy (P = .02). This study highlights the need for development of inexpensive and accessible treatments for the reduction of lipodystrophy.
Introduction
The introduction of highly active antiretroviral therapy (HAART) has led to a significant reduction in AIDS-related morbidity and mortality. 1 Abnormalities in fat distribution (lipodystrophy), insulin resistance and diabetes, dyslipidemia, hyperlactatemia, osteopinea, and osteonecrosis are some of the morphologic and metabolic complications of long-term HAART use. 2,3 Lipodystrophy is characterized by fat loss (lipoatrophy) in the face, arms, buttocks, and legs; or/and fat gain (lipohypertrophy) in the abdomen and breasts, as well as over the back of the neck (”buffalo hump"). 4 The morphological changes are potentially stigmatizing, resulting in poor adherence to antiretroviral therapy (ART) and hence treatment failure. 5
Lipodystrophy associated with long-term HAART use has been widely described in the developed world. 4,6 Such data are limited in India and is confined to tertiary HIV care centers in urban areas. 7–10 As ART becomes more available to the HIV-infected population in rural areas, it is important to determine the prevalence of its complications in these areas. Therefore, it was proposed to find out the prevalence of lipodystrophy among patients receiving ART in rural South India. The prevalence of dyslipidemia in patients receiving ART compared to HIV-positive ART-naive and HIV-negative adults in this population was also studied.
Material and Methods
Study Population
In this cross-sectional study, HIV-infected patients on ART, visiting the ART center at Namakkal District Head Quarters Hospital, Tamil Nadu, India, were recruited from February 2007 to April 2009. They were on generic first-line fixed-dose combinations of ART, provided for free by the Indian Government under its national ART program. HIV-positive individuals visiting the ART center for ART screening, and follow-up clinics at the Prevention of Mother to Child Transmission (PMTCT) centers in Namakkal District served as the first comparison group. There was a second comparison group of healthy HIV-negative adults who had accompanied the HIV-positive patients. All the participants were aged 18 years or above. Written informed consent was obtained from all the participants. The exclusion criteria for all the participants were active substance or alcohol abuse, current usage of anabolic steroids, glucocorticoids, lipid-lowering or hypoglycemic drugs, recent opportunistic infection, or malignancy.
Assessments and Measurements
Sociodemographic information, anthropometric measurements, and details of type and duration of ART regimen were recorded. Patients' self-perception of lipodystrophy (lipohypertrophy and lipoatrophy) was obtained using standardized questionnaires and clinically confirmed by the physician at the ART center. Lipoatrophy was defined as facial fat loss, peripheral fat loss on arms, legs, or buttocks. Lipohypertrophy was defined as central fat gain on upper back, chest, or abdomen. The questionnaire was administered in the local language (Tamil), which was spoken by all patients. The questionnaire was explained in detail to the patients to ensure all participants understood the requirements.
Anthropometric measurements included body weight (kg), height (cm), waist circumference (cm), and hip circumference (cm). Participants were weighed wearing light clothing and without shoes to the nearest 0.1 kg. Height was measured to the nearest millimeter using a stadiometer, the participant not wearing shoes. Body mass index (BMI, weight in kg divided by the square of the height in m) was calculated. Waist circumference to the nearest millimeter was measured using a cloth tape measure halfway between the lowest rib and the iliac crest. Hip circumference to the nearest millimeter was measured at the level of the anterior superior iliac spine when this could be palpated; otherwise, it was measured at the broadest circumference below the waist. The waist-to-hip ratio (WHR) was calculated from these measures.
The CD4 counts before initiation of therapy was recorded for patients on therapy. Current CD4 counts were recorded for all the HIV-infected patients. An overnight fasting blood was drawn to determine serum lipids levels. Aliquots of serum were stored at −80°C. Total cholesterol, high-density lipoprotein (HDL) cholesterol, and triglycerides were analyzed by colorimetric enzymatic methods with reagents purchased from Identii (Spain) using Stat Fax 3300 chemistry analyzer (Awareness Technology, USA). Low-density lipoprotein (LDL) cholesterol and very low density lipoprotein (VLDL) cholesterol was calculated using the Friedewald formula. 11 Dyslipidemia was defined as total cholesterol ≥200 mg/dL, HDL-cholesterol ≤40mg/dL, LDL-cholesterol ≥130 mg/dL, and triglycerides ≥150 mg/dL by the US National Cholesterol Education Program (NCEP) III guidelines. 12
Statistical Analysis
Data entry and Database management was completed using Microsoft Office Excel 2003. Statistical analyses were done using Statistical Package for Social Sciences (SPSS) Version 11.0.1. Descriptive statistics were presented for all variables. Association between characteristics (age, gender, literacy, habit, and BMI classification) and prevalence of abnormal metabolic levels of the study groups was compared by chi-square test. ANOVA test was used to compare the mean anthropometric measurements, biochemical, and immunological values between the study groups, if the data was normally distributed. Multiple comparisons were made by post hoc test Bonferroni pair-wise comparison. For nonnormal data comparisons, Kruskal-Wallis Nonparametric test was used. For normally distributed data, linear association between any 2 variables was determined by Pearson correlation. In the case of nonnormal data, nonparametric measure of correlation, Spearman correlation coefficient was used. Both univariate and multivariate logistic regression analysis was done to see the risk factor for ART regimen, abnormal metabolic levels, lipodystrophy and lipoatrophy. A P value of <.05 was considered statistically significant.
Results
Total number of participants enrolled in the study was 363, with 196 (54%) females and 167 (46%) males. Three groups were studied: (1) 145 HIV-infected participants (46.9% males, 53.1% females) currently receiving ART for a mean 29.4 months (range, 2 to 60 months) with number of patients on zidovudine (ZDV)/lamivudine (3TC)/nevirapine (NVP), and AZT/3TC/efavirenz (EFV) regimens being 54 (37.8%) and 4 (2.8%), respectively, while those on stavudine (d4T)/3TC/NVP and d4T/3TC/EFV regimens were 83 (58%) and 2 (1.4%), respectively; (2) 146 ART-naive patients; and (3) 72 HIV-negative controls. Because of fat distribution concerns, 17 patients previously on d4T regimen had been switched to ZDV regimen.
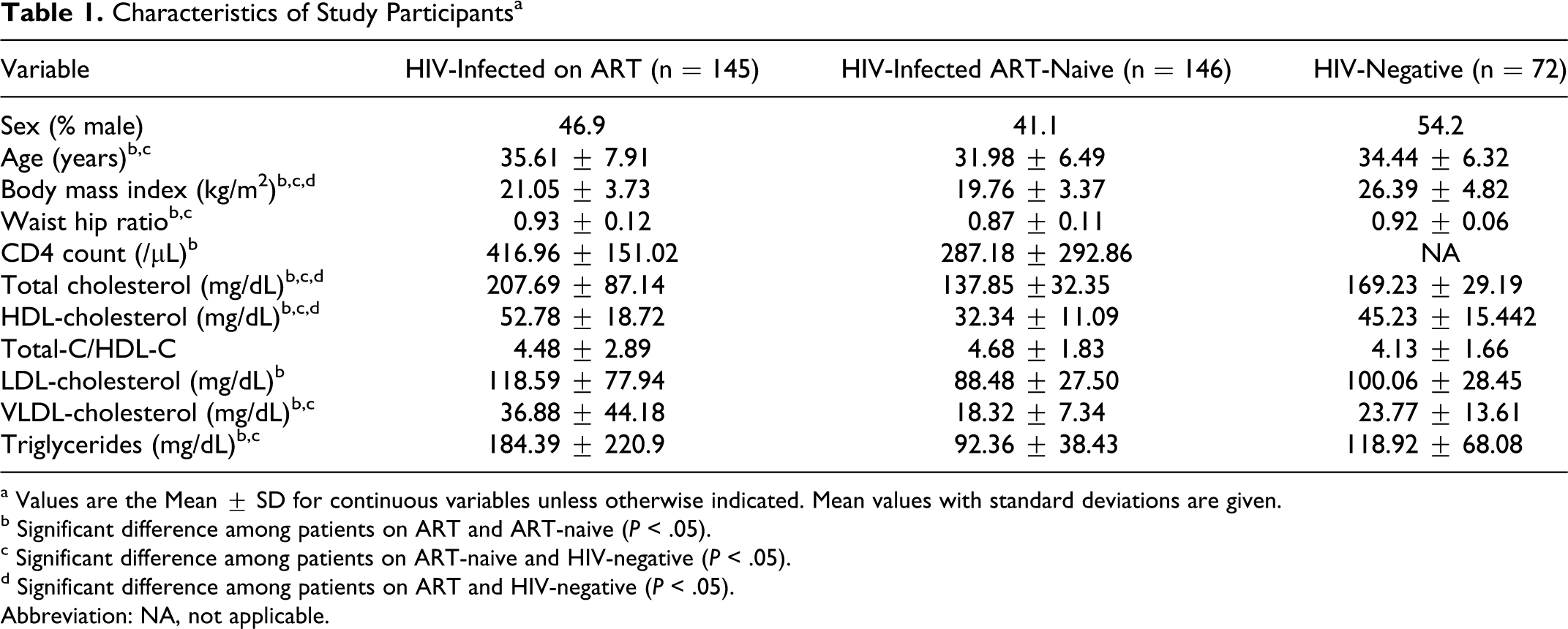
Mean age was 33.92 ± 7.23 years and mean BMI was 22.26 ± 4.46 kg/m2. The mean CD4 count was 143.23 ± 79.2/μL at the initiation of therapy in patients on ART. ART-naive patients had lower mean CD4 counts (most recent) as compared to patients on ART (287.18 ± 292.86 vs 416.96 ± 151.02; P = .00). There was no difference in gender distribution among the 3 groups and no difference in mean age among patients on ART and HIV-negative controls. However, HIV-infected patients who were ART-naive were younger than those on ART (P = .00) and HIV-negative controls (P = .048; Table 1 ).
Characteristics of Study Participantsa

a Values are the Mean ± SD for continuous variables unless otherwise indicated. Mean values with standard deviations are given.
b Significant difference among patients on ART and ART-naive (P < .05).
c Significant difference among patients on ART-naive and HIV-negative (P < .05).
d Significant difference among patients on ART and HIV-negative (P < .05). Abbreviation: NA, not applicable.
Anthropometric Characteristics
Patients on ART had higher mean BMI (P = .00) as compared to ART-naive patients but lower mean BMI (P = .00) as compared to HIV-negative controls (Table 1). Moreover, a higher percentage of patients on ART (18.1%) were significantly underweight (BMI <18.5 kg/m2) when compared to HIV-negative controls (5.5%), with ART-naive patients being the most underweight (38.8%; P = .00).Severely underweight patients (BMI <16.5 kg/m2) were also of a significantly higher percentage among HIV-infected patients (ART = 3.5%, ART-naive = 11.5%, HIV-negative = 1.4%; P = .00).
Lipodystrophy
Among the patients on ART, the prevalence of lipodystrophy was 60.7%; 22.7% with lipohypertrophy, 51.1% with lipoatrophy, and 22.7% with mixed pattern. There was a significant difference in lipodystrophy pattern between females and males, with females having a higher prevalence (62.5% vs 37.5%; P = .004). Prevalence of lipoatrophy was also higher in females (68.9% vs 31.1%; P = .015). Moreover, there was a higher prevalence of facial atrophy among women compared to men (68.8% vs 31.2%; P = .029).
There was no significant difference in the prevalence of lipodystrophy and type of ART in this study population. Lipodystrophy was reported in 62.1% of patients currently on ZDV regimens and 58.8% of patients currently on d4T regimens. Lipoatrophy was documented in 34.5% of patients currently on ZDV and 29.4% of patients currently on d4T regimens. Because of fat distribution concerns, 17 patients previously on d4T regimen had been switched to ZDV regimen. There was a higher prevalence of lipoatrophy among all patients currently or previously receiving d4T regimens as compared to those receiving ZDV regimens only, but it was not significant (33.7% vs 26.85%; P = .85). Among all the patients with lipodystrophy, 70.9% received or had received d4T. Also, 75.6% of all participants with lipoatrophy, 63.2% with mixed pattern, and 65% with lipohypertrophy, received or had received d4T. Moreover, 55.4% of patients who had ever received d4T had facial atrophy.
Total duration of ART was significantly associated with lipodystrophy, with 7.1%, 37.6%, and 55.3% of patients having developed lipodystrophy within 1 year, 1 to 2 years, and more than 2 years, respectively, of initiating ART (P = .04). However, even though participants with lipodystrophy had higher mean duration (months) of therapy compared to those without lipodystrophy (30.35 ± 12.41 vs 27.61 ± 13.86, P = .219), there was no significance.
Dyslipidemia
Patients on ART had significantly higher mean total cholesterol (P = .00), HDL-cholesterol (P = .00), LDL-cholesterol (P = .00), VLDL-cholesterol (P = .00), and triglycerides (P = .00), when compared to ART-naive patients and higher total cholesterol (P = .00), HDL-cholesterol (P = .003), VLDL-cholesterol (P = .012), and triglycerides (P = .007), when compared to HIV-negative controls (Table 1).
As seen in Table 2 , the proportion of patients with dyslipidemia according to NCEP III guidelines was significantly higher in the treatment group when compared to ART-naive and HIV-negative controls except for the proportion of abnormal HDL-cholesterol (≤40 mg/dL), which was significantly higher in the ART-naive group.
Prevalence of Dyslipidemia

a Pearson chi-square.
There was a significantly higher proportion of patients on d4T regimen with abnormal NCEP III total cholesterol elevation (≥200 mg/dL; 47.7%) than those on ZDV regimens (24.1%) (P = .006). Both groups showed no other significant differences in dyslipidemic patterns. Total duration of ART was positively correlated with total cholesterol (r = .197, P = .019).
Therapy duration also had significant association with dyslipidemia with 47.4% (P = 0.003), 34.2% (P = .057), and 48.7% (P = .045) of patients developing abnormal elevations of total cholesterol, LDL-cholesterol, and triglycerides more than 2 years after initiating ART. A higher percentage of abnormal reduction in HDL-cholesterol was seen in 39.6% (P = .007) of patients within 1 to 2 years of treatment initiation. Type of therapy was not a risk factor for abnormal metabolic parameters by logistic regression analysis but age and duration of ART were risk factors for abnormal metabolic levels (Table 3 ). Also, abnormal levels of total cholesterol (odds ratio 1.039, 95% CI 1.01-1.07, P = .008) and triglycerides (odds ratio 1.032, 95% CI 1.0-1.06, P = .024) were independent risk factors with duration of therapy.
Associations of Variables with Abnormal Metabolic Parameters by Logistic Regression

a P < .05.
Abbreviations: OR, odds ratio; R, reference category.
There was no difference among lipodystrophic and nonlipodystrophic patients with regard to mean BMI and waist-hip ratio (Table 4 ). However, compared to nonlipodystrophic patients, a higher proportion of lipodystrophic patients were overweight (18.6% vs 13.2 %, P = .065). Also, compared to nonlipodystrophic patients, lipoatrophic patients were significantly underweight (25% vs 10.3%; P = .022).)
Anthropometry and Lipid Profile Values in Lipodystrophy

a t-test.
b P < .05.
Lipodystrophic patients had significantly higher VLDL-cholesterol (P = .043) and triglycerides (P = .043) than nonlipodystrophic patients and also had higher total cholesterol but not significantly (Table 4). Also, lipoatrophic patients had significantly lower waist (78.73 ± 8.85 cm vs 86.69 ± 14.55 cm; P = .033) and hip circumference (84.87 ± 8.51 cm vs 92.52 ± 10.08 cm; P = .013) compared to lipohypertrophic patients. Moreover, by logistic regression, only abnormal metabolic levels were a risk factor in lipodystrophy (Table 5 ).
Associations of Variables with Lipodystrophy by Logistic Regression
a P < .05.
Discussion
This is one of the very few studies reporting on the prevalence of lipodystrophy in India. We have demonstrated a high prevalence of lipodystrophy and dyslipidemia among patients taking first-line WHO-recommended regimen in rural South India, as against HIV-infected ART-naive individuals and HIV-negative control group. Majority of the patients were on d4T-based regimen. This regimen is popular because of the fear of development of anemia with AZT-based regimen in a population already having low hemoglobin levels. 7 As per the National ART program, maximum percentage of adults are on the regimen d4T3 + 3TC + NVP (42.4%) followed by AZT + 3TC + NVP (39.8%). 13 For diagnosing lipodystrophy, we used patient self-reporting and confirmation by a clinician. This is the most widely used method and has been suggested as the best method to use in the absence of objective measures of lipodystrophy. 14,15
This study on the prevalence of lipodystrophy in a rural setting among HIV-infected participants receiving free generic ART from the Indian Government is to our knowledge the first of its kind in India. We documented a higher prevalence of lipodystrophy in our study (60.69%). Higher prevalence of lipodystrophy (46.1%) was documented from a study from Maharashtra, 7 whereas only 14.5% of lipodystrophy was reported in a study from Gujarat, 8 both from western India. Studies have been documented from developed countries with high prevalence of lipodystrophy; similar to the finding of our study. 16,17
We observed that gender may play a role in the prevalence of lipodystrophy in this rural population, with the female gender reporting a higher prevalence. Similar observations were reported from South Africa and Senegal. 18,19 This observation is particularly important when considering the care of HIV-infected women in terms of decisions regarding ART. With respect to the type of regimen, we did not document any significant differences in the prevalence of lipodystrophy between patients currently or previously receiving d4T regimens as opposed to ZDV regimens. This data is contrary to the study in India where d4T use was significantly associated with lipoatrophy. 7 A recent study from the United States reported lipoatrophy to be more frequent with NRTI regimen. 20 However, we did observe a higher but insignificant prevalence of lipoatrophy among all patients receiving d4T regimens as compared to those receiving ZDV regimens only. That we did not observe significant results may be due to the reason that we did not have the past history of d4T usage for 45.5% of our patients. The increased apoptosis of adipocytes may be the possible mechanism for the lipoatrophy associated with d4T. 8 Although we did not note significant results with type of ART regimen, we observed that duration of ART regimen may influence the prevalence of lipodystrophy. This is in concurrence with the studies from Australia and South Africa, which concluded that prevalence and severity of lipodystrophy reflected both length and type of treatment with ART. 21,22 This high prevalence of lipodystrophy is stigmatizing and may lead to poor adherence or discontinuation of ART, 16 and may eventually result in treatment failure. Further studies in this population determining the history of ART usage and its relation to lipodystrophy are warranted.
With regard to dyslipidemia, according to NCEP III guidelines, we observed that the proportion of patients with abnormal levels of total cholesterol, LDL-cholesterol, and triglycerides were significantly higher in the treatment group when compared to treatment-naive and HIV-negative controls. But we also observed that the prevalence of abnormal HDL-cholesterol was lower in the treatment group. The results obtained are similar to that arrived at by Pujari SN et al. 7 Drugs of the NNRTI class, and particularly NVP, although associated with high total cholesterol and LDL-cholesterol levels, may also induce an increase in HDL-cholesterol. 23,24 A predominant percentage (94.4%) of our study population had NVP in their treatment regimen, and the usage of NVP may explain the favorable HDL-C levels in the treatment group compared to the ART-naive group.
Although there was a significantly higher proportion of patients on d4T regimen with abnormal NCEP III cholesterol elevation than those on ZDV regimens, type of ART regimen was not a risk factor for dylipidemia by logistic regression. However, duration of ART regimen not only influenced lipodystrophy but also dyslipidemia, even after adjusting for type of therapy, age, sex, and BMI, and was independently associated with NCEP III cholesterol and triglyceride elevation. While a study from India reported no association between dyslipidemia and type and duration of therapy, 7 other studies have documented the effect of NRTI, particularly d4T, in the development of dyslipidemia.25,26 Moreover, in this study, lipodystrophy was associated with dyslipidemia after adjusting for BMI, age, and sex. Lipodystrophic patients had elevated triglyceride levels compared to nonlipodystrophic patients similar to a study from Senegal. 19 These findings are important as lipid anomalies increase the risk of coronary heart disease.
When considering anthropometry, a higher percentage of patients on ART had significantly lower BMI when compared to HIV-negative controls with ART-naive patients being the most underweight. A higher percentage of severely underweight patients of BMI <16.5 kg/m 2 were also seen among HIV-infected patients suggesting that nutritional support is needed in the ART centers despite access to HAART. Similar results were seen in the study from Senegal. 19
Limitations of our study include the cross-sectional design and nonrandomized treatment allocations. In addition, morphologic changes were assessed subjectively and did not use Dual Energy Xray Absorptiometry (DEXA) and computed tomography (CT) as they were expensive.
In summary, our study demonstrates a high prevalence of morphologic and metabolic complications among patients taking WHO-recommended first-line generic HAART. Female patients presented more with lipodystrophy, particularly with lipoatrophy than males. The type of treatment regimens was not associated with lipodystrophy although d4T usage seemed to affect total cholesterol levels. Total duration of ART was significantly associated with lipodystrophy and dyslipidemia. Presence of lipodystrophy had association with abnormal lipid levels. Also, patients on ART as well as ART-naive patients had lower BMI than HIV-negative patients. This study not only highlights the need for development of inexpensive and accessible treatments for the reduction of lipodystrophy but also the need for adequate nutritional support.
Footnotes
Acknowledgments
We thank the participants for their valuable time and commitment. We acknowledge the support of Dr E. Ramesh Kumar and the staff of the ART center at Namakkal Head Quarter Hospital. We also thank D. Anitha and A. Ganesh of the Department of Experimental Medicine, The Tamil Nadu Dr MGR Medical University, Chennai, for technical assistance. Our gratitude to the Vice-Chancellor of The Tamil Nadu Dr MGR Medical University for his kind support.
Declaration of Conflicting Interests
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.