
Abstract
HIV prevention research among men who have sex with men (MSM) has traditionally focused on individual risk reduction strategies. Our study evaluated awareness, utilization, and preferences for 10 complementary HIV prevention strategies among 1,286 MSM recruited via Facebook and Instagram from June-August 2018. Ages ranged from 18-85 years, and the majority were non-Hispanic white (n = 1,019, 79.24%), college-educated (n = 819, 63.69%), gay-identifying (n = 1,074, 83.51%), and partnered (n = 808, 62.83%). Post-exposure prophylaxis was the least familiar option, and engaging in sexual activities other than anal sex was the most utilized option. Progressively older and bisexual-identifying MSM were less likely, but those with higher educational levels and easy access to local HIV resources were more likely to be aware of and to be utilizing a greater number of strategies. Additionally, Hispanic MSM were less likely to be aware of, and those in a “closed” relationship were less likely to be utilizing a greater number of strategies. In a subset of 775 multiple strategy users, pre-exposure prophylaxis, regularly testing for HIV, and limiting the number of sex partners emerged as the most preferred options. Combination intervention packages for MSM should be tailored to personal circumstances, including sexual orientation, relationship characteristics and access to local HIV resources.
Keywords
Introduction
Men who have sex with men (MSM) represent approximately 2% of the general United States (US) population 1,2 but remain disproportionately impacted by HIV. In 2018, more than 70% of the estimated 36,400 new HIV infections across the country were attributable to male-to-male sexual contact. 3 At year’s end in 2018, 576,787 MSM were living with diagnosed HIV infection. 4 Sexually transmitted infections (STIs) such as gonorrhea, chlamydia and syphilis are more prevalent among MSM living with HIV compared to those who are HIV-negative. 5 Coinfections are especially concerning because both ulcerative and non-ulcerative STIs can promote the sexual transmission of HIV through biological and behavioral mechanisms. 6,7 The Centers for Disease Control and Prevention (CDC) acknowledges that stopping the spread of HIV among MSM is a key national priority that could be achieved by identifying unrecognized infections, improving outcomes at each step of the HIV care continuum and harnessing all prevention strategies to help men protect themselves and their partners. 8
Over the past 4 decades, domestic and foreign investments in HIV-related research have fostered the development of a variety of behavioral and biomedical risk reduction strategies. 9,10 The HIV prevention toolkit includes multiple options such as regularly testing for HIV and other STIs, limiting the number of sex partners, always using condoms during anal sex, taking pre-exposure prophylaxis (PrEP) every day to prevent HIV, and taking post-exposure prophylaxis (PEP) for 28 days after possibly being exposed to HIV. 11 Consensus generally exists that behavioral and biomedical strategies at not at odds with one another and have complementary roles in HIV prevention efforts geared towards those at elevated risk. 12 Although scientific evidence for the efficacy of different HIV prevention tools is abundant, translating this evidence into real-world solutions to reduce transmissions among sexually active MSM has remained a challenge because of a variety of individual, interpersonal and structural barriers. 13,14 Characterizing subgroups of MSM who are not being reached by existing services and thoughtfully directing limited public health resources towards engaging them in the HIV prevention continuum 15 are essential to successfully curtail the epidemic.
Modeling suggests that combination intervention packages that include multiple HIV prevention strategies can reduce the incidence of HIV among MSM, 16,17 but achieving their full impact will require investments in broader reforms (e.g., routine opt-out HIV testing in clinical settings, reducing societal homophobia, expanding PrEP financial assistance programs). 18 The development of such packages is often guided by theoretical frameworks such as the AIDS risk reduction model, 19 social cognitive theory, 20 and the information-motivation-behavioral skills model. 21 Some common threads among these theories are that individuals should recognize their risk for HIV, know how to mitigate their risk, and perceive themselves as being capable of undertaking risk reduction activities. Being aware of the range of HIV prevention tools is pivotal to an individual’s decision-making process around the potential uptake and maintenance of one or more options. Not all MSM, however, have similar levels of exposure to HIV risk reduction information. A study evaluating the online and offline sexual health information-seeking patterns of HIV-negative MSM found that participants who were less open about their sexuality accessed significantly fewer sources of information, thereby reducing their likelihood of receiving HIV prevention messages. 22 Identifying MSM subgroups with limited awareness of HIV prevention strategies can help guide the development of customized communication campaigns to impart relevant information on both traditional and contemporary HIV prevention approaches.
Simply being familiar with various options in the HIV prevention toolkit is insufficient to prompt their adoption. Not all prevention tools are equal, and different individuals depending on their personal circumstances might use different strategies. For instance, partnered MSM have been documented to test less frequently for HIV and other STIs compared to those who are single, 23 as they tend to believe they are at lower risk. 24 A recent systematic review on relationship-based predictors of sexual risk for HIV among male couples has also reported that positive relationship dynamics such as greater levels of commitment, attachment, emotional intimacy, satisfaction, social support, equality, constructive communication and trust promote condomless anal sex (CAS) with primary partners, but protect against CAS with outside partners. 25 Data from the CDC’s 2017 National HIV Behavioral Surveillance (NHBS) show that Non-Hispanic black and Hispanic MSM are less likely to discuss PrEP with a healthcare provider or to use PrEP compared to non-Hispanic white MSM. 26 Mistrust of the medical community among racial and ethnic minorities has been identified as a possible deterrent to their PrEP uptake. 27,28 Such examples bolster the need for designing and evaluating tailored combination intervention packages for different MSM subgroups that take into account varying personal circumstances and recognize the facilitating or hampering roles of different service delivery settings.
To date, much of the HIV prevention research among HIV-negative MSM in the US has focused on the knowledge and use of individual risk reduction strategies rather than concurrently considering multiple options. 29 -31 Some studies have compared preferences for strategies such as always using condoms during anal sex versus taking PrEP every day, 32,33 but we are unable to find published research that has simultaneously evaluated a wider range of risk reduction tools. Disparities that exist in the comprehension of HIV epidemiology and transmission dynamics across age, race and ethnicity, educational level, sexual orientation and relationship characteristics of MSM 34 might extend to the awareness and utilization of HIV prevention strategies. To fill extant gaps in the literature, we sought to quantify awareness and utilization of 10 complementary HIV prevention tools among MSM, and to identify potential variations in awareness and utilization of an increasing number of strategies across demographic and behavioral characteristics. We also sought to elucidate the most preferred options among current users of multiple strategies. Given the heterogeneity of lived experiences of diverse MSM subgroups, a deeper understanding of these issues is important.
Methods
Study Design
Participants were recruited through selective placement of advertisements on 2 social media platforms (Facebook and Instagram) from June to August 2018. Our advertisements included images of men kissing, hugging or holding hands, the study title (“Project Flourish”) and the following call-to-action text: “Check out our brief survey on HIV prevention strategies and make your voice heard!” Individuals who clicked through the advertisements were directed to a survey landing page programmed in Qualtrics. This provided basic information about the purpose of our study, the anonymous and voluntary nature of our survey, a study email address to contact the research team, and a clickable button to document electronic informed consent. Individuals who consented were screened to determine eligibility (identify themselves as male, are ≥18 years of age, currently reside in the US, engaged in anal sex with at least one man in the past 6 months, have never been diagnosed with HIV), and those who met the eligibility criteria were administered a Web-based survey. No identifying information was collected from participants, and no incentives were provided for completing our survey.
Data Collection
Demographic information collected from participants included their age, race and ethnicity, educational level, state of residence, health insurance coverage, sexual orientation and relationship status. Partnered men could indicate whether they were in a “closed” relationship (defined as sex with outside partners was not allowed) or in an “open” relationship (defined as sex with outside partners was allowed with or without restrictions). Participants were asked about their injection and non-injection drug use (other than drugs prescribed by a healthcare professional), and binge drinking behavior (defined as consuming ≥5 alcoholic drinks at the same time or within a couple of hours of each other) in the past 6 months. The survey also included questions on their engagement in CAS with multiple male partners within the same period. Easy access to local HIV resources was assessed using the following question: “Next, we will ask you about some HIV prevention and treatment resources that might be available in some communities. For each option, please tell us whether it is easily accessible to you in your community: (i) free HIV testing and counseling, (ii) treatment for HIV, (iii) free testing for other STIs (e.g., gonorrhea, chlamydia, syphilis), (iv) treatment for other STIs, (v) free condoms, (vi) free water-based lubricants, (vii) syringe/needle exchange programs, (viii) free or low-cost health facilities for gay, bisexual and other men who have sex with men, (ix) pre-exposure prophylaxis (PrEP), (x) post-exposure prophylaxis (PEP).” Participants were also asked about their HIV and other STI testing history.
Awareness and utilization of different HIV prevention strategies were assessed by asking participants to select “I know about this” and “I currently do this” for each of the following 10 strategies: (i) regularly testing for HIV (e.g., every 6 months to 1 year), (ii) regularly testing and getting treated for other STIs (e.g., chlamydia, gonorrhea, syphilis), (iii) limiting the number of sex partners, (iv) encouraging partners to get tested and treated for HIV and other STIs, (v) discussing HIV and other STI status with partners, (vi) only having sex with known HIV-negative partners, (vii) engaging in sexual activities other than anal sex (e.g., oral sex, mutual masturbation), (viii) always using condoms during anal sex, (ix) taking PrEP every day to prevent HIV (e.g., Truvada®), (x) taking PEP for 28 days after possibly being exposed to HIV. These strategies were chosen because information on their attributes is readily available to the general public on official US Government websites. 35,36 Participants who selected “I currently do this” for multiple HIV prevention strategies were asked to indicate their single most preferred option from a personalized menu of strategies they were utilizing.
Statistical Analyses
SAS version 9.4 was used to conduct data analyses. Demographic and behavioral characteristics of the sample were summarized using descriptive statistics. Participants’ responses to the question on easy access to local HIV resources were combined into the following 5 domains: (i) easy access to HIV testing and treatment, (ii) easy access to other STI testing and treatment, (iii) easy access to condoms and water-based lubricants, (iv) easy access to syringe/needle exchange programs, and (v) easy access to health facilities offering PrEP or PEP. For example, those who specified that free condoms and/or free water-based lubricants were easily accessible to them in their community were classified under domain (iii). Proportions of participants who selected “I know about this” and “I currently do this” for each HIV prevention strategy were tabulated (overall and stratified by age, race and ethnicity, educational level, sexual orientation and relationship category). Differences in awareness and utilization of each strategy across participant characteristics were assessed using Chi-squared tests. Data on preferences for different HIV prevention strategies in the subset of participants who reported currently utilizing multiple options were also summarized using descriptive statistics.
For our Model 1 outcome (i.e., awareness of a greater number of HIV prevention strategies), we created a new variable for each participant by tallying the number of strategies for which they selected “I know about this”. This ordered categorical variable could range from 0 (none) to 10 (all). For our Model 2 outcome (i.e., utilization of a greater number of HIV prevention strategies), we created another new variable for each participant by tallying the number of strategies for which they selected “I currently do this”. This ordered categorical variable could also range from 0 (none) to 10 (all).
Initially, we formulated 2 separate cumulative logit models to identify factors independently associated with awareness (Model 1) and utilization (Model 2) of a greater number of HIV prevention strategies using outcome variables with 11 ordered categories. These models take into account the inherent ordering of categories in each of our outcome variables, thus making fuller use of the ordinal information compared to multinomial logit models. One assumption that should not be violated when fitting cumulative logit models is the assumption of proportional odds. In our models this assumption means that the odds ratio assessing the effect of a covariate (e.g., age) will be the same regardless of whether we are comparing awareness (Model 1) or utilization (Model 2) of ≥1 versus 0, ≥2 versus ≤1, ≥3 versus ≤2, ≥4 versus ≤3, ≥5 versus ≤4, ≥6 versus ≤5, ≥7 versus ≤6, ≥8 versus ≤7, ≥9 versus ≤8, or finally, 10 versus ≤9 strategies. The proportional odds assumption can be checked using a statistical test known as the Score test. If the P < 0.05 (or <0.10 to be more conservative when checking assumptions), then the proportional odds assumption is not satisfied. The P for the Score test for our original Model 1 was <0.0001, and for our original Model 2 was <0.0001. Therefore, we decided to reduce the number of categories for each of our outcome variables without disrupting the ordering as follows: none, 1-2 strategies, 3-4 strategies, 5-6 strategies, 7-8 strategies, and 9-10 strategies.
Next, we formulated 2 separate cumulative logit models to identify factors independently associated with awareness (Model 1) and utilization (Model 2) of a greater number of HIV prevention strategies using outcome variables with 6 categories. However, the proportional-odds assumption was still not satisfied for either model. The P for the Score test for our revised Model 1 was <0.0001, and for our revised Model 2 was 0.0071. Therefore, we decided to further reduce the number of categories for each of our outcome variables without disrupting the ordering as follows: none, 1-5 strategies, and 6-10 strategies.
Finally, we formulated 2 separate cumulative logit models to identify factors independently associated with awareness (Model 1) and utilization (Model 2) of a greater number of HIV prevention strategies using outcome variables with 3 categories. This time the proportional-odds assumption was satisfied for both models. The P for the Score test for our final Model 1 was 0.2106, and for our final Model 2 was 0.4989. Each model included the following covariates: age (continuous in 10-year increments), race and ethnicity, educational level, region of residence, health insurance coverage, sexual orientation, relationship category, injection or non-injection drug use in the past 6 months, binge drinking in the past 6 months, CAS with ≥2 men in the past 6 months, have easy access to HIV resources in their community. Results are presented as adjusted odds ratios (aORs) with 95% confidence intervals (CIs). Point estimates from each model represent the adjusted odds of being aware of and utilizing a greater number of prevention strategies (i.e., 6-10 versus 1-5 and none, or 6-10 and 1-5 versus none) respectively in a particular demographic or behavioral stratum compared to the referent.
Ethical Approval and Informed Consent
Before the study was initiated, ethical approval was obtained by the University of Michigan Institutional Review Board - Health Sciences and Behavioral Sciences (IRB-HSBS) in Ann Arbor (Reference#HUM00142480). All individuals who were interested in participating were asked to provide electronic informed consent. Only those individuals who consented were screened to determine eligibility, and those who met the eligibility criteria were enrolled as study participants.
Results
Details pertaining to the formulation of the analytic sample are presented in Figure 1. Briefly, 720,866 advertising impressions resulted in 12,858 click-throughs to the survey landing page over a 3-month period. Of these, 3,357 individuals provided consent, 2,820 completed the eligibility screener, and 1,508 met the eligibility criteria. Analyses for this manuscript are restricted to 1,286 of 1,362 (94.42%) survey completers who provided data on awareness and utilization of one or more HIV prevention strategies. No statistically significant differences were observed between participants who were included in the analytic sample and those who were excluded with respect to demographic and behavioral characteristics.
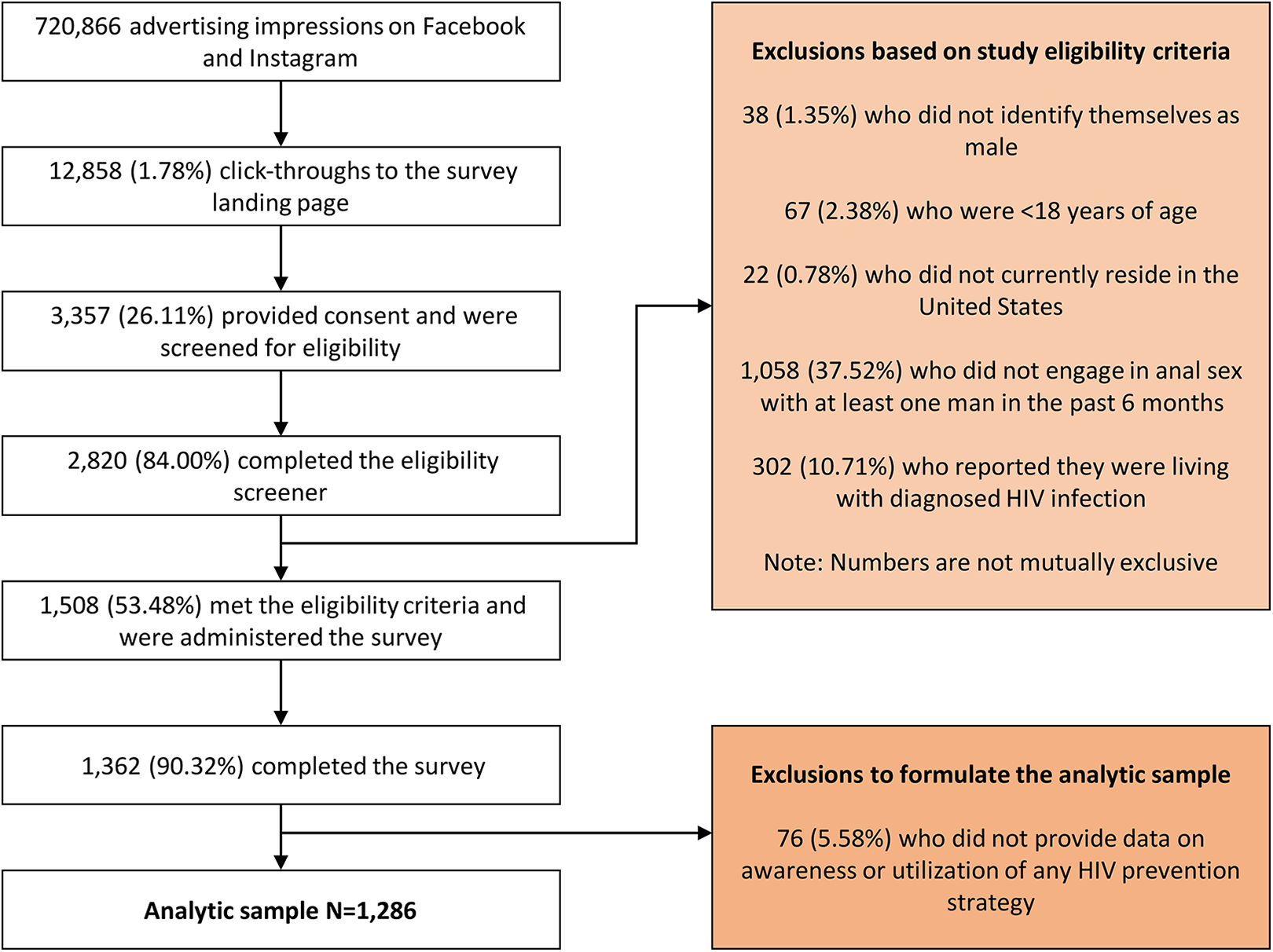
Formulation of the analytic sample of 1,286 HIV-negative or unknown status MSM recruited via Facebook and Instagram, United States, June-August 2018.
Table 1 summarizes the descriptive characteristics of 1,286 participants. Ages ranged from 18 to 85 years, with both the mean being 42 years. The majority of participants were non-Hispanic white (n = 1,019, 79.24%), had a Bachelor’s degree or higher educational level (n = 819, 63.69%), identified as gay (n = 1,074, 83.51%), and were partnered (n = 808, 62.83%). A higher proportion of partnered men were in a “closed” relationship (n = 441, 54.58%) versus an “open” relationship (n = 367, 45.42%). Regarding sexual behavior, more than two-thirds (n = 514, 39.97% reported engaging in CAS with ≥2 men in the past 6 months. Approximately one-fifth (n = 294, 22.86%) reported not having easy access to HIV resources in their community. Slightly less than two-thirds (n = 828, 64.39%) had been tested for HIV in the past year, and slightly more than half (n = 669, 52.02%) had been tested for other STIs in the past year.
Demographic and Behavioral Characteristics of 1,286 HIV-Negative Or Unknown Status MSM Recruited Via Facebook and Instagram, United States, June-August 2018.

a Mean = 42 years, Range = 18-85 years.
b Includes 33 black, 24 Asian, 12 Native American/Alaskan Native, 6 Middle Eastern/North African, 3 Native Hawaiian/Pacific Islander and 40 multiracial.
c Includes 127 with an Associate’s/Technical degree, 264 with some college education, 74 with a high school diploma or General Educational Development (GED) and 2 with some high school education.
d Includes 3 straight, 29 queer and 6 questioning.
e Defined as sex with outside partners was not allowed.
f Defined as sex with outside partners was allowed with or without restrictions.
g Includes 386 who reported using amyl nitrite (“poppers”), 95 who reported using cocaine, 78 who reported using MDMA (Ecstasy or Molly), 48 who reported using opioids (heroin, fentanyl or pain relievers) and 37 who reported using methamphetamine.
h Defined as consuming ≥5 alcoholic drinks at the same time or within a couple of hours of each other.
i Includes 766 who indicated that free HIV testing and counseling and 665 who indicated that treatment for HIV were easily accessible to them in their community.
j Includes 722 who indicated that free testing for other STIs and 715 who indicated that treatment for other STIs were easily accessible to them in their community.
k Includes 760 who indicated that free condoms and 556 who indicated that free water-based lubricants were easily accessible to them in their community.
l Includes 371 who indicated that free or low-cost health facilities, 437 who indicated that PrEP and 340 who indicated that PEP were easily accessible to them in their community.
Awareness of each of the 10 HIV prevention strategies reported by 1,286 participants is presented in Table 2. Overall, 1,211 participants (94.17%) were aware of 6-10 strategies, 66 (5.13%) were aware of 1-5 strategies and 9 (0.70%) were not aware of any strategy. Familiarity with almost all options was high except taking PEP for 28 days after possibly being exposed to HIV, for which less than three-fourths of participants (n = 935, 72.71%) selected “I know about this”. Differences in awareness of specific strategies were observed across some participant characteristics. For example, fewer Hispanic men selected “I know about this” for always using condoms during anal sex compared to non-Hispanic men. Fewer men who had an Associate’s/Technical degree or lower educational level selected “I know about this” for regularly testing for HIV versus those who had a Bachelor’s degree or a Master’s/Doctoral degree.
Awareness of HIV Prevention Strategies Among 1,286 HIV-Negative Or Unknown Status MSM Recruited Via Facebook and Instagram, United States, June-August 2018.

Note: Values in bold indicate statistically significant differences in awareness of a specific HIV prevention strategy across strata of a particular participant characteristic (Chi-squared P < 0.05).
a Mean = 42 years, Range = 18-85 years.
b Includes 33 black, 24 Asian, 12 Native American/Alaskan Native, 6 Middle Eastern/North African, 3 Native Hawaiian/Pacific Islander and 40 multiracial.
c Includes 127 with an Associate’s/Technical degree, 264 with some college education, 74 with a high school diploma or General Educational Development (GED) and 2 with some high school education.
d Includes 3 straight, 29 queer and 6 questioning.
e Defined as sex with outside partners was not allowed.
f Defined as sex with outside partners was allowed with or without restrictions.
Utilization of each of the 10 HIV prevention strategies reported by 1,286 participants is presented in Table 3. Overall, 390 participants (30.33%) were utilizing 6-10 strategies, 741 (57.62%) were utilizing 1-5 strategies and 155 (12.05%) were not utilizing any strategy. Engaging in sexual activities other than anal sex (e.g., oral sex, mutual masturbation) was the most commonly utilized option, for which more than 3 in 5 participants (n = 790, 61.43%) selected “I currently do this”. Differences in utilization of specific strategies were observed across some participant characteristics. For example, fewer men who identified as bisexual or some other sexual orientation selected “I currently do this” for taking PrEP compared to those who identified as gay. More men in an “open” relationship selected “I currently do this” for discussing HIV and other STI status with partners versus those who were single or in a “closed” relationship.
Utilization of HIV Prevention Strategies Among 1,286 HIV-Negative Or Unknown Status MSM Recruited Via Facebook and Instagram, United States, June-August 2018.

Note: Values in bold indicate statistically significant differences in utilization of a specific HIV prevention strategy across strata of a particular participant characteristic (Chi-squared P < 0.05).
a Mean = 42 years, Range = 18-85 years.
b Includes 33 black, 24 Asian, 12 Native American/Alaskan Native, 6 Middle Eastern/North African, 3 Native Hawaiian/Pacific Islander and 40 multiracial.
c Includes 127 with an Associate’s/Technical degree, 264 with some college education, 74 with a high school diploma or General Educational Development (GED) and 2 with some high school education.
d Includes 3 straight, 29 queer and 6 questioning.
e Defined as sex with outside partners was not allowed.
f Defined as sex with outside partners was allowed with or without restrictions.
Figure 2 presents data on the utilization of each HIV prevention strategy among participants who were aware of that option. The largest gaps between awareness and utilization were for taking PEP for 28 days after possibly being exposed to HIV, taking PrEP every day to prevent HIV, and always using condoms during anal sex. Of the 935 participants who were aware of PEP, 903 (96.58%) were not utilizing that option, of the 1,109 participants who were aware of PrEP, 864 (77.91%) were not utilizing that option, and of the 1,185 participants who were aware of always using condoms during anal sex, 899 (75.86%) were not utilizing that option. The smallest gaps between awareness and utilization were for engaging in sexual activities other than anal sex (e.g., oral sex, mutual masturbation), and discussing HIV and other STI status with partners. Of the 1,124 participants who were aware of engaging in sexual activities other than anal sex, 790 (65.07%) were utilizing that option, of the 1,203 participants who were aware of discussing HIV and other STI status with partners, 780 (64.84%) were utilizing that option.

Utilization of each HIV prevention strategy among participants who were aware of that option in a sample of 1,286 HIV-negative or unknown status MSM recruited via Facebook and Instagram, United States, June-August 2018.
Table 4 includes results from the 2 cumulative logit models evaluating factors independently associated with awareness and utilization of a greater number of HIV prevention strategies (i.e., 6-10 versus 1-5 and none, or 6-10 and 1-5 versus none) respectively. Regarding awareness, increasing age was associated with significantly lower odds of being aware of a greater number of strategies. Participants who were Hispanic and identified as bisexual were also less likely to be aware of more strategies (compared to those who were non-Hispanic white and identified as gay respectively). However, those who had a Master’s/Doctoral degree and had easy access to HIV resources in their community were more likely to be aware of more strategies (compared to those who had an Associate’s/Technical degree or lower educational level and did not have easy access to local HIV resources respectively). Regarding utilization, increasing age was associated with significantly lower odds of utilizing of a greater number of strategies. Participants who identified as bisexual and were in a “closed” relationship were also less likely to be utilizing more strategies (compared to those who identified as gay and were single respectively). However, those who had a Bachelor’s degree or higher educational level, were in an “open” relationship and had easy access to HIV resources in their community were more likely to be utilizing more strategies (compared to those who had an Associate’s/Technical degree or lower educational level, were single and did not have easy access to local HIV resources respectively). Both models adjusted for risk behaviors including injection and non-injection drug use, binge drinking, and engaging in CAS with multiple male partners in the past 6 months, none of which were independently associated with awareness or utilization of a greater number of HIV prevention strategies.
Factors Independently Associated With Awareness and Utilization of a Greater Number of HIV Prevention Strategies Among 1,286 HIV-Negative or Unknown Status MSM Recruited Via Facebook and Instagram, United States, June-August 2018.

Note: Values in bold indicate a statistically significant association (P < 0.05).
a Ordered categories include not being aware of any strategy (n = 9), being aware of 1-5 strategies (n = 66) and being aware of 6-10 strategies (n = 1,211). Point estimates from the cumulative logit model represent the adjusted odds of being aware of a greater number of strategies (i.e., 6-10 versus 1-5 and none, or 6-10 and 1-5 versus none) in a particular demographic or behavioral stratum compared to the referent.
b Ordered categories include not utilizing any strategy (n = 155), utilizing 1-5 strategies (n = 741) and utilizing 6-10 strategies (n = 390). Point estimates from the cumulative logit model represent the adjusted odds of utilizing a greater number of strategies (i.e., 6-10 versus 1-5 and none, or 6-10 and 1-5 versus none) in a particular demographic or behavioral stratum compared to the referent.
c Mean = 42 years, Range = 18-85 years.
d Includes 33 black, 24 Asian, 12 Native American/Alaskan Native, 6 Middle Eastern/North African, 3 Native Hawaiian/Pacific Islander and 40 multiracial.
e Includes 127 with an Associate’s/Technical degree, 264 with some college education, 74 with a high school diploma or General Educational Development (GED) and 2 with some high school education.
f Includes 3 straight, 29 queer and 6 questioning.
g Defined as sex with outside partners was not allowed.
h Defined as sex with outside partners was allowed with or without restrictions.
i Includes 15 who reported injection drug use and 467 who reported non-injection drug use (386 reported using amyl nitrite (“poppers”), 95 reported using cocaine, 78 reported using MDMA (Ecstasy or Molly), 48 reported using opioids (heroin, fentanyl or pain relievers) and 37 reported using methamphetamine).
j Defined as consuming ≥5 alcoholic drinks at the same time or within a couple of hours of each other.
k Derived by combining responses to the question asking which of the following HIV prevention and treatment resources are easily accessible to participants in their community: (i) free HIV testing and counseling, (ii) treatment for HIV, (iii) free testing for other STIs (e.g., gonorrhea, chlamydia, syphilis), (iv) treatment for other STIs, (v) free condoms, (vi) free water-based lubricants, (vii) syringe/needle exchange programs, (viii) free or low-cost health facilities for gay, bisexual and other men who have sex with men, (ix) pre-exposure prophylaxis (PrEP), (x) post-exposure prophylaxis (PEP).
Seven hundred and seventy-five of 1,023 (75.76%) multiple strategy users indicated their single most preferred option from a personalized menu of strategies they were currently utilizing. Non-responders were more likely to be partnered men in a “closed” relationship, but were similar with respect to other characteristics. Taking PrEP every day to prevent HIV (n = 153, 19.74%), regularly testing for HIV (n = 140, 18.06%), and limiting the number of sex partners (n = 135, 17.42%) were the most preferred options. These were followed by always using condoms during anal sex (n = 100, 12.90%), engaging in sexual activities other than anal sex (n = 79, 10.19%), only having sex with known HIV-negative partners (n = 68, 8.77%), and discussing HIV and other STI status with partners (n = 65, 8.39%). Regularly testing and getting treated for other STIs (n = 21, 2.71%), encouraging partners to get tested and treated for HIV and other STIs (n = 12, 1.55%), and taking PEP for 28 days after possibly being exposed to HIV (n = 2, 0.26%) were the least preferred options.
Discussion
Developing tailored combination intervention packages that seek to reduce HIV transmissions among MSM requires an understanding of their awareness and utilization of existing prevention strategies, as well as their preferences for different options. Our study found generally high levels of awareness and variable levels of utilization of 10 complementary HIV prevention tools in a Web-based sample of sexually active MSM from across the US. Progressively older participants and those who identified as bisexual were less likely, but those with higher educational levels and easy access to local HIV resources were more likely to be aware of and to be utilizing a greater number of prevention strategies. Significant variations were also observed across strata of race and ethnicity (for awareness) and relationship category (for utilization). In the subset of multiple strategy users, taking PrEP every day to prevent HIV, regularly testing for HIV, and limiting the number of sex partners emerged as the most preferred options. For context, it is important to note that approximately 19% of the sample reported taking PrEP, approximately 50% reported regularly testing for HIV, and approximately 49% reported limiting the number of sex partners. Our results delineate how intrapersonal characteristics (e.g., age, sexual orientation) influence both knowledge and use of HIV risk reduction tools, and reinforce the importance of focusing prevention efforts on subgroups of MSM who are not being reached by existing services.
Regarding awareness of specific HIV prevention strategies among our study participants, it is encouraging that most knew about almost every option presented in our survey. The only strategy that less than three-fourths (73%) of the sample reported being aware of was taking PEP for 28 days after possibly being exposed to HIV. This is consistent with estimates from samples of MSM in large US cities such as Boston and Pittsburgh. 31,37 Although PEP has been recommended by the CDC for non-occupational exposures since 2005, 38 limited awareness of this option suggests there is a need to educate MSM, especially those engaging in CAS with multiple male partners, about this HIV prevention strategy. Public health departments, community-based organizations, and healthcare providers can all play a role in this endeavor. In recent qualitative work conducted with MSM and transgender women in New York City, many participants mentioned they had seen advertisements for PrEP on subways and buses, but only few knew about the existence or availability of PEP. 39 Those who were aware of PEP had learned about it from their healthcare providers and stated that, unlike PrEP, PEP was not a common topic of discussion in their social circles. It is not surprising that the vast majority of our participants (97%) who reported being aware of PEP were not utilizing this emergency use measure. PEP is certainly not a substitute for other HIV prevention strategies, but disseminating basic information on its attributes (e.g., initiation within 72 hours of a possible exposure, follow-up HIV testing at 1 month and 3 months) would allow MSM to consider using this back-up option if the need arises. Contact with a healthcare provider during the treatment period also offers an opportunity to discuss the appropriateness of other prevention options like PrEP.
Regarding utilization of specific HIV prevention strategies by our study participants, engaging in sexual activities other than anal sex was the most frequently reported option, overall (61%) and among participants who were aware of this strategy (65%). Educating MSM about the risk associated with anal sex, in the absence of using condoms or PrEP, has always been a key focus of HIV communication campaigns. 40,41 An analysis of pooled data from 6 US studies with MSM revealed that more than 90% of 3,565 participants responded correctly to the true-false survey question “A person can get HIV from having anal sex”. 42 Prior research has documented that some MSM abstain from anal sex entirely in order to reduce their HIV risk, 43,44 and instead participate in activities they perceive to be less risky such as oral sex, mutual masturbation, frottage, rimming and digital penetration. 45,46 In a large Web-based survey of 24,787 MSM, engaging in oral sex (73%) and mutual masturbation (68%) were more commonly reported than engaging in anal sex (37%) during the most recent sexual encounter. 47 For MSM who still perceive anal sex to be the “gold standard” of what constitutes sex, 48 a notion hypothesized by some researchers to stem from the pervasive influence of societal heterosexism, 49 a discussion around the range of sexual activities beyond anal sex during HIV prevention counseling could help alter their perception, and reinvigorate HIV prevention efforts.
Focusing next on the factors associated with awareness and utilization of multiple HIV prevention strategies, our study found some noteworthy results. Progressively older participants were less likely to be aware of and to be utilizing a greater number of strategies. One explanation for this finding could be the differential use of digital technologies commonly used to access health information and resources across age groups. According to the Pew Research Center, younger Americans are more avid users of the Internet and are more smartphone dependent compared to older Americans. 50 Despite an increase in the adoption of digital technologies by middle-aged and older adults in recent years, they often lack the confidence to assess the quality of online health information and tend to rely on healthcare providers as their primary source of medical counsel. 51,52 Unless MSM disclose their same-sex behavior, healthcare providers might not have conversations about risk reduction strategies which could lead to lower engagement in HIV prevention, including testing. 53 Another explanation for our result could be that many middle-aged and older MSM underestimate their risk of infection or believe that HIV is no longer a serious health threat. 54,55 Lower risk perceptions have in turn been associated with reduced HIV testing 56,57 and a greater engagement in CAS. 29,58 In light of our results, we echo calls to remedy the lack of attention to older MSM in prevention messages and programs aiming to curb the HIV epidemic. 59,60
Our study found that Hispanic participants were less likely to be aware of a greater number of HIV prevention tools compared to non-Hispanic white participants. Lower proportions of Hispanic participants selected “I know about this” for always using condoms during anal sex and encouraging partners to get tested and treated for HIV and other STIs compared to non-Hispanic participants. These observations are concerning given recent national trends that indicate a progressive increase in the number of HIV diagnoses among Hispanic MSM. Latest surveillance data from the CDC reveal that new diagnoses increased by 18% from 2010 to 2016 among Hispanic MSM while remaining stable for non-Hispanic black and non-Hispanic white MSM. 61 Qualitative research suggests that homophobia experienced by racial and ethnic minority MSM prevents them from being open about their sexual orientation and sexual behaviors, 62 and has been shown to negatively impact HIV prevention efforts. 63 Analogous to intergenerational variations in the use of digital technologies to access health information discussed above, racial and ethnic differences exist. By the end of 2018, 61% of Hispanics had broadband service at home compared to 66% of non-Hispanic blacks and 79% of non-Hispanic whites. 64 Hispanics are more likely to obtain health information through broadcast media (television and radio) compared to the Internet. 65 HIV communication campaigns should be cognizant of variations in digital technology utilization across racial and ethnic subgroups, be inclusive of cultural norms, and cater to language preferences of the intended audiences.
Participants who had a Master’s/Doctoral degree were more likely to be aware of and to be utilizing a greater number of HIV prevention strategies compared to those who had an Associate’s/Technical degree or lower educational level. This finding demonstrates how inequalities in educational attainment might influence the level of exposure to HIV risk-reduction information, as well as engagement in preventive services. Individuals with higher educational attainment can gain access to better social and economic opportunities, leading to better health outcomes in general. 66 In one of our recent studies, MSM with higher educational levels were more knowledgeable about specific details of HIV transmission dynamics, and incremental increases in their knowledge were positively associated with HIV testing. 34 Although not surprising, it is disconcerting that lower proportions of participants in our sample who had an Associate’s/Technical degree or lower educational level selected “I know about this” and “I currently do this” for regularly testing for HIV. The importance of testing in advancing HIV prevention efforts cannot be overstated as it is the first step in considering the use of prophylactic options like PrEP for MSM who are HIV-negative and initiating antiretroviral therapy for MSM who newly test positive for HIV. Imparting prevention education in high schools has been shown to improve testing behaviors among sexual minority males, 67,68 and might be one way to set the stage for lifelong protection among MSM who do not attend college or university.
In our sample, participants who identified as bisexual were less likely to be aware of and to be utilizing a greater number of HIV prevention tools compared to those who identified as gay. Although the prevalence of HIV has been reported to be lower among bisexual men than among gay men, 69,70 this subgroup is not immune to the risk of HIV. Some studies have found that bisexual men engage in more sexual risk behaviors compared to gay men including younger age at sexual debut, greater number of sex partners, substance use immediately before sex and CAS. 71,72 Bisexual men experience unique stressors such as internalized biphobia, challenges related to the concealment and disclosure of their identity, as well as negative attitudes towards bisexuality, 73,74 which presents barriers to accessing a variety of preventive health services. 75 -77 Their lack of integration into the gay community, potentially as a result of anticipated and experienced stigma from gay men, 78 has long been suggested as a reason why they might have limited exposure to HIV prevention information. 79 Our findings that lower proportions of bisexual men selected “I know about this” and “I currently do this” for PrEP compared to gay men suggest that HIV communication campaigns seeking to promote the uptake of this biomedical strategy might not be reaching an important subgroup of MSM. Additional research is needed to better understand the sexual health concerns and HIV prevention needs of bisexual men. 80
Compared to participants who were single, those in “closed” relationships were less likely, but those in “open” relationships were more likely to be utilizing a greater number of HIV prevention strategies. Lower proportions of men in “closed” relationships selected “I currently do this” for regularly testing for HIV and always using condoms during anal sex, whereas higher proportions of men in “open” relationships selected “I currently do this” for discussing HIV and other STI status with partners and taking PrEP. These results might reflect varying HIV risk perceptions across different types of relationships. Prior research has found that partnered men in “closed” relationships believe they are at low risk for acquiring HIV through CAS because they trust their partners do not engage in outside sexual activities, 24 and consequently do not get tested annually as recommended by the CDC. 81 In contrast, partnered men in “open” relationships have been shown to lack confidence in their ability to remain HIV-negative, 82 and believe that taking PrEP helps reduce their sexual anxiety. 83 Reports that one-third to two-thirds of HIV transmissions among MSM could been attributed to sex within primary partnerships 84,85 have prompted an increased focus on dyadic interventions for male couples including couples HIV testing and counseling that includes skills building around negotiating sexual agreements and condom use. 86 -88 Our results support the notion that a one-size fits-all approach cannot be employed for all partnered MSM, and underscore the importance of addressing HIV prevention needs across a broad range of relationship configurations.
Our study also found that participants who had easy access to HIV resources in their community were more likely to be aware of and to be utilizing a greater number of prevention strategies. This highlights the possible role of structural factors in shaping HIV prevention among individuals at elevated risk. Structural factors have been described as physical, social, economic, cultural, organizational, community, legal or policy aspects of one’s environment that can facilitate or hamper efforts to avoid HIV infection. 89 Barriers to engaging in prevention activities cited by MSM include lack of proximity to health facilities, anticipated and experienced stigma from healthcare providers, as well as perceived and actual financial constraints. 90 -92 MSM who are unable to access local HIV resources in person might not be able to get tested, learn their serostatus, receive counseling, and subsequently alter their behaviors to lower their risk. Telehealth applications such as Web-based videos, text messages and emails, chat rooms and social networking websites have been successfully used to disseminate HIV prevention information to MSM, 93 and have the potential to encourage health-promoting behaviors. Given the broad scope and complex nature of structural factors, approaches to address them are generally viewed as long-term initiatives. 94 Nonetheless, it is imperative to invest in increasing awareness and utilization of different HIV prevention tools by MSM with limited access to resources in their community.
Turning to focus on the most preferred options in the subset of multiple strategy users, the top 3 choices were taking PrEP every day to prevent HIV, regularly testing for HIV, and limiting the number of sex partners. However, it is important to bear in mind that a small proportion of men in our sample reported taking PrEP, overall (19%) and among participants who were aware of this strategy (22%). Our results are consistent with data from the CDC’s 2017 NHBS-MSM cycle, 95 and are a clear indication that although contemporary strategies such as PrEP are being embraced by some MSM, traditional risk reduction strategies retain an important place in the HIV prevention toolkit. PrEP-related stigma (anticipated and experienced), side effects, and psychosocial factors have been associated with suboptimal uptake and adherence of PrEP among MSM in high-income settings. 90 Because not all MSM are aware of PrEP, desire to use PrEP, or have the support to initiate and sustain PrEP, presenting them with information on multiple prevention options has ethical and practical benefits. We agree with proponents that argue for the promotion of less resource-intensive and more widely available HIV prevention tools in addition to scaling up PrEP for individuals at high risk for HIV acquisition. 96
Limitations of our study include the use of a convenience sample of MSM recruited via Facebook and Instagram. Ideally, all MSM in the general US population should have an equal chance of participating, but our Web-based survey’s availability was restricted to MSM who have accounts on these social media platforms, subjecting our results to sampling bias. MSM in underserved and disenfranchised communities may not have access to technology, such as such as a computer, tablet or smartphone, precluding their participation. Caution must be exercised in generalizing our results to MSM users of other social media platforms, users of geospatial dating apps (e.g., Grindr, Scruff), and those in the general population. Participants voluntarily self-selected into our study, resulting in a sample that was predominantly non-Hispanic white. Our sample only included 136 Hispanic and 131 non-Hispanic non-white MSM (of whom 33 were black, 24 were Asian, 12 were Native American/Alaskan Native, 6 were Middle Eastern/North African, 3 were Native Hawaiian/Pacific Islander and were 40 multiracial). Unfortunately, this underrepresentation of racial and ethnic minority MSM is analogous to previous Web-based research conducted with sexual and gender minorities in the US. 97,98 Only 74 participants had a high school diploma or General Educational Development (GED) and 2 had some high school education. Further, 992 participants reported having easy access to HIV prevention resources in their community. Therefore, our results are not generalizable to MSM of other races and ethnicities, those with lower educational attainment, or those who reside in communities with limited access to prevention resources. Our survey did not include questions on sex assigned at birth or gender identity, so we are unable to comment on what proportion of our sample identified as transgender. Although an attempt was made to formulate an exhaustive list of commonly used HIV prevention tools by MSM who are not known to be living with HIV, we acknowledge that this set might not be complete. The cross-sectional nature of our data precludes us from commenting on the temporality of observed associations with awareness and utilization of a greater number of HIV prevention strategies. Finally, almost a quarter of multiple strategy users did not indicate their single most preferred option. Non-responders were more likely to be partnered men in a “closed” relationship, which might reflect their lack of interest in HIV-related issues compared to men who are single or in an “open” relationship. 24
Conclusions
Findings from our study have important implications for furthering HIV prevention efforts among MSM in the US. New information on the awareness and utilization of 10 complementary HIV prevention strategies has been presented in this manuscript. Subgroups of MSM that could potentially benefit from tailored HIV communication campaigns seeking to impart information and promote the uptake of both traditional and contemporary HIV prevention approaches have also been identified. Researchers developing combination intervention packages for MSM should bear in mind that preferences for different options are likely to vary depending upon an individual’s personal circumstances, including their sexual orientation, relationship characteristics and access to local HIV resources.
What Do We Already Know About This Topic?
Investments in HIV-related research have fostered the development of a variety of behavioral and biomedical risk reduction tools, and harnessing all prevention strategies can help stop the spread of HIV among men who have sex with men (MSM).
How Does Your Research Contribute to the Field?
Unlike previous research that has focused on individual risk reduction strategies, our study presents new information on the awareness, utilization, and preferences for 10 complementary HIV prevention options in a large sample of sexually active, highly educated, non-Hispanic white MSM, and describes variations in awareness and utilization of an increasing number of strategies across demographic and behavioral characteristics.
What Are Your Research’s Implications Toward Theory, Practice, or Policy?
Our study identifies subgroups of MSM that could potentially benefit from tailored HIV communication campaigns seeking to impart information and promote the uptake of both traditional and contemporary HIV prevention approaches.
Footnotes
Authors’ Note
Before the study was initiated, ethical approval was obtained by the University of Michigan Institutional Review Board - Health Sciences and Behavioral Sciences (IRB-HSBS) in Ann Arbor (Reference#HUM00142480). All individuals who were interested in participating were asked to provide electronic informed consent. Only those individuals who consented were screened to determine eligibility, and those who met the eligibility criteria were enrolled as study participants.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.