
Abstract
In 2012, the US Food and Drug Administration approved Truvada as a pre-exposure prophylaxis (PrEP) for adults at risk of HIV. PrEP is highly effective at preventing HIV when taken daily, but no gold standard exists for consistently administering PrEP to populations at highest risk. The “I Am Men’s Health” program used an innovative methodology to generate adherence to PrEP in 23 mostly young men who have sex with men of color (yMSMc), during a 28-week period from February to September 2013. Adherence was measured using weekly medication pickup rates. The average age of the participants was 21 years, and the majority were black and lived below the poverty line. Time on PrEP ranged from 1 to 28 weeks (2723 person-days), and the weighted average adherence was 73%. The methodology used in this study was preliminarily effective at generating adherence to PrEP among high-risk yMSMc in a community setting and may help inform large-scale future HIV prevention interventions.
Introduction
In the United States, young men of color who have sex with men (yMSMc) have the highest incidence of HIV infection compared with all other age groups and races. The HIV prevalence in men who have sex with men (MSM) is estimated to be 12.3%, and MSM represented 63% of new infections in 2010. 1,2 African Americans accounted for 46% of those new infections, despite only representing 12.6% of the population. 2 Additionally, HIV incidence in individuals aged between 13 and 29 increased 21% from 2006 to 2009, representing the only age range in which the incidence increased. 2 In light of these statistics, an intervention to reduce the risk of HIV infection in yMSMc should be a public health priority.
Pre-exposure prophylaxis (PrEP), or Truvada, consists of tenofovir (TDF) and emtricitabine taken as a combination pill once a day to prevent HIV infection. Pre-exposure prophylaxis was recently shown to be 43.8% effective in reducing HIV infection. 3 This number increased to 92% in people with detectable drug levels, indicating the importance of strict adherence. The Food and Drug Administration recently recommended oral Truvada for preventive use among people at higher risk of HIV exposure, including MSM and partners of HIV-infected people. 4 Young MSM of color, however, often have limited access to health care—including PrEP—due to factors such as high rates of poverty, lack of insurance, complexity of the health care system, and high out-of-pocket costs of medications. 5,6 Furthermore, this group may have difficulty taking chronic medications consistently; several studies published in the last decade have shown that adherence among HIV-infected youth on antiretroviral therapy (ART) is low, ranging from 27% to 41%. 7 –10
Currently, no gold standard exists for treating specific subpopulations with PrEP, much less than one that is as high risk and difficult to reach as yMSMc. The primary aim of the “I Am Men’s Health” program is to produce a scalable methodology for comprehensive HIV risk reduction that includes the use of daily PrEP. This article describes that methodology and reports the characteristics of the program’s participants and their adherence to the medication through the first 28 weeks. The Philadelphia FIGHT institutional review board granted exempt status to this retrospective review of data.
Program Methods
The PrEP program began enrolling participants in January 2013 in Philadelphia, Pennsylvania. Philadelphia’s poverty rate is 25.6%, African Americans comprise 44.3% of the population, and the HIV prevalence is 1.9%, making this city ideal for a PrEP program targeted at high-risk yMSMc. 11,12 The PrEP program is conducted at the Youth Health Empowerment Project (Y-HEP) in downtown Philadelphia. Y-HEP was established in 1994 as a citywide project to reduce the spread of HIV and sexually transmitted diseases (STDs) among adolescents and young adults. Today, Y-HEP serves more than 3,000 high-risk and hard-to-reach youth. Although Y-HEP operates with an open-door policy, recruiting efforts and program offerings have attracted a population that predominantly consists of low socioeconomic status yMSMc.
The PrEP program operates a weekly clinic from 7 to 9
When a new participant is recruited, a PrEP team member provides him with a description of the program and participant responsibilities. If interested, he signs an informed consent document and fills out a contact information sheet. If uninsured, he completes the Gilead Truvada for PrEP Medication Assistance Program application and provides evidence of his income (or lack thereof), usually with pay stubs or a tax return form. The Patient Assistance Program, whose aim, according to Gilead’s Web site, is to “assist eligible HIV-negative adults in the United States, who do not have insurance obtain access to Truvada,” sends medications directly to Y-HEP for dispensation. Patients with health insurance do not use the Patient Assistance Program, as most insurance companies (including Medicaid insurance plans) cover Truvada.
Once the PrEP staff receives Truvada, the new participant is tested for HIV viral load; hepatitis panel (A, B, and C); basic metabolic panel; rapid plasma reagin; urine trichomonas test; and urine, pharyngeal, and rectal gonorrhea and chlamydia. If the participant’s HIV status is verified as negative by viral load, the PrEP program staff provides him with the first 7 pills of Truvada; describes possible initial side effects; and offers adherence strategies, such as putting the pill box next to a toothbrush or setting a phone alarm. If the participant tests positive for any STD, he is treated by the PrEP team at Y-HEP. Likewise, if he is found to lack immunity to hepatitis A or B, the appropriate vaccines are administered.
After initiating PrEP, the participant reports to Y-HEP once a week for medication pickup. Participants are required to get monthly rapid HIV tests as well as quarterly STD and kidney function testing. They are encouraged to pick up their medications and receive any necessary tests when the PrEP program is open on Monday nights. The majority of participants do so, come at any point during the week, since one of the PrEP program members is also a full-time employee at Y-HEP.
Results
In the first 28 weeks, 23 participants enrolled and took PrEP according to medication pickup data. Time on PrEP ranged from 1 to 28 weeks (2,723 person-days) on therapy. Three participants withdrew due to personal obligations. The average participant age was 21 years, and the majority were black males, had received some form of public assistance, and lived in a household with an income less than the Federal Poverty Line for a family of 4 (Table 1). 13 In total, 39% had been kicked out of their home due to their sexual orientation, and 43% had spent at least 1 night on the street or in a shelter; 22% had exchanged sex for money, housing, or some other benefit in their life. Health care access was also an issue, and 39% were uninsured. Seventy-four percent reported inconsistent condom use, and 43% had at least 3 sexual partners in the last year. Seven STDs were diagnosed, 3 during baseline testing (1 chlamydia, 1 gonorrhea, and 1 trichomonas), and 4 during the course of the program (3 chlamydia and 1 gonorrhea). None of the participants were found to have chronic hepatitis B or C upon baseline screening, but over half were found to be nonimmune to hepatitis A, B, or both, and each of these participants was given the appropriate vaccination series. One prospective participant tested positive for HIV during his initial baseline testing and, as a result, was linked immediately to care for HIV but was not able to participate in the PrEP program. No participant seroconverted to HIV while in the program.
Participant Characteristics.a
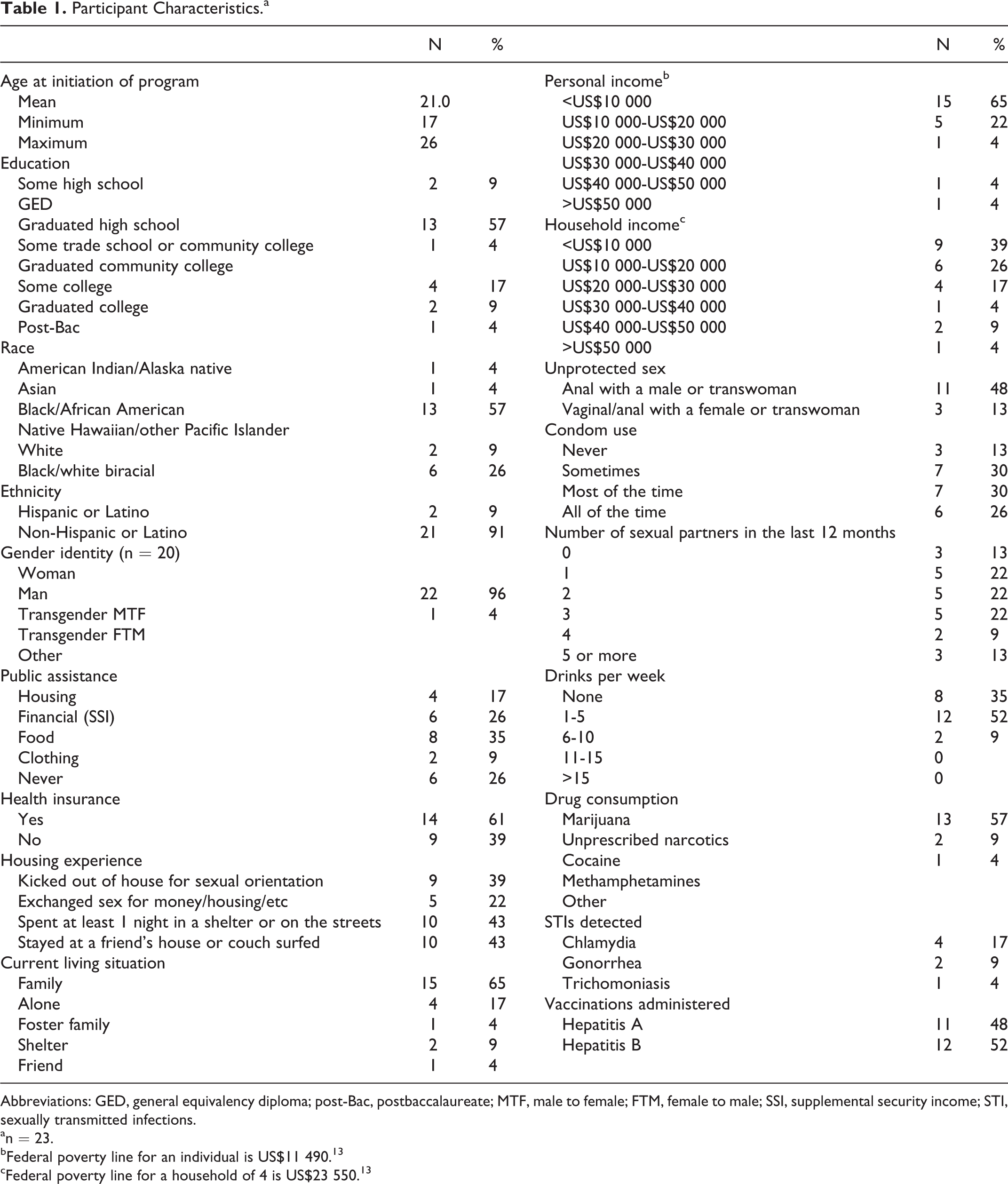
Abbreviations: GED, general equivalency diploma; post-Bac, postbaccalaureate; MTF, male to female; FTM, female to male; SSI, supplemental security income; STI, sexually transmitted infections.
an = 23.
bFederal poverty line for an individual is US$11 490. 13
cFederal poverty line for a household of 4 is US$23 550. 13
Despite these risk factors in our population, adherence to PrEP was excellent. Overall, the weighted average adherence was 73%, with a median adherence of 82% for participants who had taken PrEP for at least 1 month (Figure 1A). Adherence ranged from 13% to 100% with a lower quartile of 70% and an upper quartile of 92%. Additionally, our data showed a consistent adherence over time. The average adherence was 79% for participants who had completed 16 weeks, 69% after week 20, 69% after week 24, and 88% after week 28 (Figure 1B).

Adherence to pre-exposure prophylaxis (PrEP) for the 20 participants who have taken at least 4 weeks of medication. A, The interquartile range. n = 20 is less than the n = 23 participants who have completed surveys, as 3 participants had not yet been enrolled and picking up medication for 4 full weeks. B, Adherence by 4-week block. Enrollment is rolling, so participants have spent varying amounts of time in the program. Four weeks represent the data for all the participants’ first month in the program, and 28 weeks represent the adherence in the seventh month for the 2 participants who have been enrolled that long.
Discussion
The success of this program in generating adherence can be attributed to a series of intervention methods. Although there is significant overlap, the methodology can be broken down into 4 categories: Colocalization of the PrEP program at a site already frequented by yMSMc: Housing the PrEP program at a site where yMSMc already feel safe and derive benefit from other services provided (meals, trauma therapy, washer/dryer, shower, computer labs, leadership training courses, etc.) has no doubt been a critical part of our early success. Frequency of contact: Participants receive 7 pills each week, which ensures consistent contact with the PrEP team. Additionally, participants are sent weekly Facebook messages to remind them of their visits. Due to the frequency of lost and stolen cell phones, as well as unpaid phone bills, Facebook has proven to be the most consistent medium of communication with participants. Holistic focus on participants’ well-being: In addition to HIV prevention, the program promotes other components of a healthy lifestyle. Staff members make condoms available at medication pickups, emphasize risk-reduction practices, screen for STDs every 3 months, treat any diagnosed STDs, and provide hepatitis vaccines. Additionally, several members of the PrEP team have organized activities for the participants, such as a running program and a cookout with healthy dining options, and 1 participant has been set up with a tutor to assist him with his community college course work. Sense of community: The team’s social worker conducts a weekly workshop that the majority of participants choose to attend. The curriculum covers diverse topics, such as leadership, risk reduction, and improving self-awareness. These workshops have coincided with private interviews conducted with each participant to get their feedback on the PrEP program. Participants are also actively involved in the leadership and community development programs that Y-HEP offers. Finally, PrEP team T-shirts are being made for each participant and PrEP team member.
Financial incentives have not been used in the program to generate adherence. We hope to create the mind-set that the value of this program is receiving a free-of-charge, risk-reducing medication and having consistent access to the peer and provider resources of the program. When asked by a nonparticipant if there was a program stipend, 1 participant stated, “you can’t put a price on your life.”
Impact and Next Steps
We believe that the methodology, which produced the high adherence rates in this program, will be replicable in future efforts. A series of analyses have shown that PrEP drastically reduces HIV transmission and is cost-effective when targeted at the appropriate high-risk populations. 14 In 2008, Desai et al 15 reported that providing PrEP to 25% of the MSM population in the United States would be cost-effective when compared with the status quo HIV-infection risk and cost of ART in a similar care environment. More recently, Juusola et al 1 showed that, while PrEP is currently too expensive to be cost-effective in the general MSM population, targeting it to MSM who have multiple sexual partners is attractive at current costs and comparable to the cost per quality-adjusted life year of other currently endorsed intervention methods.
With the effectiveness of PrEP established through multiple international trials and our methodology demonstrating encouraging adherence, we plan to take the following 2 steps: Implement a more accurate measure of adherence- In July, our program received National Institutes of Health funding through the Center for AIDS Research at the University of Pennsylvania to validate a urine TDF assay for measurement of adherence compared with plasma TDF levels. Rather than requiring frequent blood draws, a urine assay could provide a minimally invasive yet effective method for measuring medication adherence. Scale the program up while maintaining adherence rates- We aim to enroll a total of 50 patients and have applied for further funding to ensure that participants will have access to the same level of personnel and resources in an expanded program. We plan to expand outreach efforts to local bathhouses and university student groups at risk of HIV.
In addition to scaling up our own program, we hope the methods outlined in this article can be implemented by organizations with a focus similar on Y-HEP and our PrEP team. The populations most in need of a risk-reduction program for HIV are those least likely to receive it, but we believe PrEP represents an excellent opportunity to both reduce HIV infection risk and encourage a holistic focus on personal health.
Footnotes
Acknowledgments
The authors acknowledge the support of the New York Academy of Medicine, the Infectious Disease Society of America, and the Arnold P. Gold Foundation. Dr. Laura Bamford MD, MSCE, provided assistance in generating the paper’s figures, and the PrEP team consisting of Victoria Lopez, Caroline Sloan, Elizabeth Ketner, and Jordan Caldwell Lollis was absolutely critical to the program’s operation and success. Additionally, Y-HEP provided the space for the weekly clinic and was invaluable in assisting our recruiting and retention efforts, and the Jonathan Lax Treatment center assisted with testing procedures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.