
Abstract
Responding to the increasing reports of health students and professionals demonstrating stigmatized attitudes toward people living with HIV (PLHIV), this article examined the learning process that takes place during their academic training. Using symbolic interactionism as a theoretical framework, we studied the way lecturers in dietetic schools in Indonesia make meaning of their understanding and experience of HIV in relation to their teaching conduct. We found that the current curriculum does not provide adequate opportunities for students to learn and interact with PLHIV. Participants described HIV discussion is mainly limited to the clinical aspects and essential treatment as they were uncomfortable discussing HIV with the students. The ostensible symbolic meaning of HIV among dietetic lecturers in Indonesia was compounded with limitations and restrictions affecting their teaching practices and attitudes to PLHIV. Future intervention is required to help lecturers recognize their degree of awareness and personal values about HIV.
What Do We Already Know about This Topic?
Prejudicial attitudes and discriminations toward people living with HIV (PLHIV) persist among health professionals and students despite their training.
How Does Your Research Contribute to the Field?
We found that the academic experiences that take place during their clinical trainings are likely to contribute to poor understanding and lack of acceptance toward PLHIV.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
The attribution theory proposes an explanation on how lecturers feel ambivalence about initiating HIV discourse in class; a strong call to action for policy makers in the health and education sectors to take corrective measures by improving curriculum and training for lecturers.
Background
The growing problems of HIV and AIDS require health professionals, including dietitians, to mobilize for HIV care and control. However, studies reported that acceptance to people living with HIV (PLHIV) in Indonesia is low in the general population and so is among health professionals. Patients reported of being isolated, discriminated, forced to undergo HIV testing, received substandard care, and denied from getting treatment. 1 -4 These resulted in not only low HIV testing and counseling uptake but also delayed treatment and poor adherence to medication among the patients. 5,6
Dietitians play an important role in HIV treatment as adequate nutrition improves immune function, treatment outcomes, and quality of life. 7 -9 Nonetheless, limited studies have been conducted to evaluate their capacity and willingness to treat PLHIV. Earlier studies were mostly done among doctors and nurses. 1,2,4,6,10 One should note that, however, the interaction between patients and dietitians are limited compared to doctors and nurses. 11 This situation is likely to undermine their awareness of prejudice and stigma toward PLHIV.
Education contribution to HIV prevention and stigma reduction is evident. Review from several education programs in Africa found that context-specific action-based teaching method was effective to initiate a discussion about HIV and reduce stigma. 12 This study highlighted 2 important elements that contribute to effective school-based HIV prevention program; the curriculum and instructors. The curriculum needs to be developed in accordance with the social context of HIV, whereas the instructors need to be trained to deliver HIV information with sensitivity to encourage much deeper discussion. 13
Sensitivity is necessary for communicating HIV in Indonesia because sexuality is considered a taboo topic and thus heavily stigmatized. 2 HIV awareness campaign is limited since often the actions are deemed to contradict the cultural value and beliefs. For instance, as all religions in Indonesia condemned promiscuity and extramarital sex, the promotion of condom use is often seen as a campaign to support free sex instead of safe sex. 2,14,15
Because health professionals are not immune to the stigma and discrimination toward PLHIV, 1,16,17 understanding what is happening in each academic institution is of an important topic. We performed this study with the purpose to explore the experiences of lecturers in dietetic schools in Indonesia on teaching topics related to HIV considering the lack of literature from dietetics’ perspectives. Since the curriculum is critical to ensure the effectiveness of educational-based endeavors, we elaborate on curriculum analysis in this article.
Methods
Research Purpose and Questions
This study aimed to explain the perspective of lecturers teaching in dietetics schools in Indonesia about HIV and how that affects their teaching conduct. To attain the research objective, this study sought to answer 2 research questions: How do lecturers describe their experience and perspective on HIV and AIDS? How do lecturers make meaning of their experience and perspective on HIV and AIDS to their teaching conduct?
Theoretical Framework and Research Design
The theoretical perspective that provides a framework for this study was symbolic interactionism that aims to understand the dynamics of how people make meaning to the physical and/or social objects in their lives. 18,19 Although limited, lecturers in dietetics schools are likely to exposed to several resources about HIV and AIDS throughout their careers. Their interaction could include symbols such as textual information, statistics, dialogues, academic discussion and debate, policies, artifacts, and social reality. However, as dynamic as the interaction or exposure is, there is no fixed outline of human conduct as implications of the encounter. 19 The interaction includes responses such as acceptance, refusal, resistance, and coping strategies to deal with the pressure exerted by structure and system. 19 This means that no one could predict how lecturers would turn their interaction with HIV and AIDS resources to their teaching conduct. Therefore, Oliver (2012) suggested that to understand the process of making inferences, the focus of analysis should not be on the symbol or events rather the focus should be on how individuals perceived the events. 20
Align with the symbolic interactionism; attribution theory was applied as a substantial theory in this study. This theory is rooted in the social psychology area and aimed to explain perceived causation and the consequences of such perception. The basic tenet is divided into 2 parts: (1) people interpret events for its causes and; (2) the way people construe perception affects their emotional reactions. 21,22 Studies found that HIV interventions were surrounded by sociocultural symbols and meanings. HIV testing, for example, was viewed as a symbol of responsibility and mutual commitment to the relationship among dating couple, yet, between a married couple, it was considered as a sign of infidelity accusation to one partner and a lack of trust. 23,24 Using the first part of the theory, this study explored the symbolic interpretation of HIV-related matters from the lecturers’ point of view, and using the second part of the theory, it explained the impact of the attribution they have on their teaching conduct. Considering the nature of the research question and theoretical framework, we used an interview study as a methodological approach to solicit data and information from the study participants.
Participants
Participants in this study consisted of lecturers teaching in 3 dietetics schools in Indonesia (2 state universities and 1 private university). They were selected using the maximum variance sampling method as well as purposeful sampling to obtain participants with diverse background and experiences. 25,26 There were 2 variabilities considered for selection; university affiliation and areas of specialization. All participants mainly teach in an undergraduate program and have at least 1 year working experience. To protect the confidentiality, they were contacted separately, and pseudonyms were used throughout data analysis and reporting. Since all the study participants know the primary investigator personally, we assumed the role of a cultural insider.
The participants’ characteristics are summarized in Table 1. Thirteen lecturers agreed to participate in this study; 8 were from the state universities and 5 were from the private university. Most of the participants were women, Muslims, specialized in clinical nutrition, and held a master degree. Regarding cultural background, all of them were Indonesians and of the Java tribe.
Characteristics of Participants of the Study.

Data Collection
Data were collected over a period of 5 months between November 2016 and March 2017. A conversational interview was utilized as a primary method of data collection considering the close contact between participants and the primary investigator. An interview guide was utilized as a prompt for the interview (Appendix A). The interviews were conducted twice and face to face, with an average length of 50 minutes per interview. We translated all participants’ direct quotation from the Indonesian Language into English.
In addition to the interview, a document analysis was conducted to seek further explanation and clarification. Participants were asked to submit various documents such as syllabus, reading materials, handouts, lecture notes, academic publications, university handbooks, samples of student assignments, and any relevant documents at any time between the first and second interviews. These documents were also used as a prompt during the second interview. We also maintained a reflective journal throughout the study to record participants’ reflection, thoughts, and reactions during interviews. This process enables the researcher to shackle the interplay of one subjectivity during data collection and interpretation, and thus, enhancing trustworthiness. 27,28
Data Analysis
All interviews were transcribed at verbatim within the same week to avoid losing the nonverbal expression and cues. Transcripts were typed and digitally saved as word files in a password-protected personal computer, which only the primary investigator could get access to it. The transcriptions were made separately for each interview and coded with the participants’ pseudonyms. The transcripts, then, were shown to the participants for a member check. Also, documents received from the participants were filed and dated for future references in the analysis. The focus of the document analysis was on the mapping of HIV discourse within the current curriculum in each dietetic school.
A manual thematic analysis with an inductive approach was performed on the data. We followed the 6 steps of data analysis to analyze content, identify codes, categories, and themes. 29 The first cycle coding for all data sources (interview transcripts, documents, and reflective journals) was done manually using the In Vivo open coding method to extract the literal words from the actual records. For the documents analysis and reflective journal, attribute coding was conducted to complement results from the In Vivo coding. Next, axial coding was used to determine the relationship between codes and group them into categories. Lastly, using the selective coding, the categories were integrated into themes that reflected the symbolic meaning of HIV among participants and their impact on teaching conduct. 25,30 Table 2 shows the themes and their constituent categories.
Themes and Categories.

Abbreviation: PLHIV, people living with HIV.
Ethical Approval and Informed Consent
This study was approved by the Institutional Board Review (IRB) of Kansas State University # 8555 as well the Indonesian Medical and Health Research Ethics Committee Faculty of Medicine Universitas Gadjah Mada—Dr Sardjito General Hospital reference number KE/FK/0129/EC/2017. Participation was voluntary based; participants were free to decline the invitation to take part in the study, refuse to respond to the interview questions, and withdraw their participation at any time. They were given information about the study objectives and protocols of data collection before consenting to the study. All participants provided written consent to the study. Their confidentiality and anonymity were protected and pseudonyms used in the study and its subsequent publications.
Results and Discussion
This study provides an explanation on how lecturers in dietetics schools in Indonesia make meaning of their understanding of HIV in relation to their teaching conduct. To our knowledge, this is one of few studies to examine the root cause of stigma toward PLHIV in health facilities as well as the likelihood of an “intergenerational” stigma learned from lecturers to students. This is also the first study within the Indonesian dietetic education system. Understanding the situation can help to inform the development of better curriculum and learning environment to alleviate stigma. Moreover, it has the potential to facilitate better quality of care for PLHIV.
There were 13 categories and 4 major themes arose from the data provided insight into 2 research questions. Using the attribution theory, the first and second themes, limited access to HIV resources and selective acceptance to PLHIV, explain the antecedent of HIV attributes. These 2 themes show how participants make attributes toward PLHIV according to the information they have about HIV and their beliefs. On the other hand, the third and fourth themes explain the consequences of such attribution, which are medicalization of HIV and reluctance to discuss HIV (Figure 1).
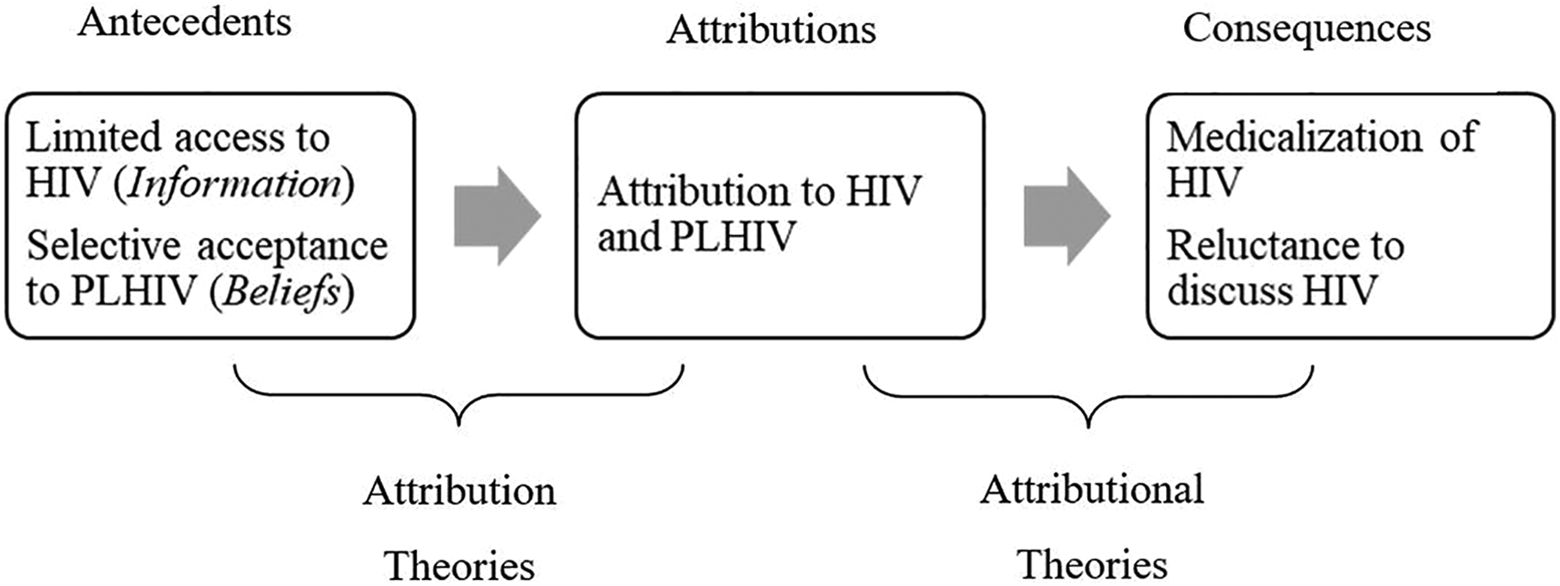
Application of attribution theory, modified from Kelley and Michela.21
Limited Access to HIV Resources
According to the first central assumption of attribution theory, cognition mediates the relationship between an antecedent or stimuli and the emotional reactions. Individuals follow the process of acquiring, selecting, processing, restoring, and evaluating information before making inferences and decisions for their emotional reactions. 21,22 Earlier studies showed a positive correlation between providing adequate information or knowledge to favourable attitudes that in turn lead to the adoption of positive behaviors. Improving HIV-related knowledge was found to lead to more positive attitudes to testing and treatment as well as acceptance to the key populations. 31 -33
However, most participants in our study acknowledge their limited understanding of the interrelation of HIV and nutrition due to the lack of opportunity to learn about HIV during their academic and clinical training. Topics related to HIV and AIDS were poorly taught merely as part of other courses and was never thoroughly covered. Participants also mentioned about the lack of chances to participate in any professional development activities to improve their knowledge and skills on HIV care and control. Therefore, they rely on other sources to obtain information such as TV, newspapers, the internet, and research publications. The first time I learned about HIV was in senior high school [grade 10]. The science teacher talked about reproductive organs broadly and discussed a bit about HIV. Also, I once volunteered in an NGO [nongovernment organization] worked in family planning and HIV. They gave us training about that [HIV]. It was very basic mainly about the transmission and the severity of AIDS. I could not recall if I got that [information about HIV] during either my bachelor or master study. One thing that I remember, the lecturers did not allow us to take care of HIV-positive patients during clerkship; they just let me know that the person was HIV positive. (Daisy, female, private university) I have never really studied HIV. I think they discussed it a bit in my pathophysiology class together with sepsis when I did my undergraduate study. During my master study, we discussed HIV and its five-level of prevention. Thus, I learned about the prevalence and preventive programs. I do not think I got the diet [for HIV], but I believe we can follow the dietary guideline for general infectious diseases. Well, I am not so sure, but we can always read a journal [research publication]. (Mimosa, female, state university)
Besides limited access to HIV information and training, participants in this study also mentioned about the apparent restriction imposed on them to conduct research on HIV-related topics. This restriction is not officially documented anywhere; however, the participants shared that when an idea about conducting research in HIV is being proposed, the restriction comes up. While training can directly improve knowledge, a previous study suggests that personal contact with key populations might reduce prejudice.
37,38
This strategy has been initiated in a simulated clinical setting to promote nondiscriminatory behaviour among health professionals.
39
So, I wanted to conduct a study on HIV and nutrition among female sex workers. This was supposed to be lecturer-students collaborative research. My team and I presented the proposal. We wanted to conduct the study in brothels, measuring their nutrition status, asking about their dietary habit and such things. We also planned to give them training about healthy eating and measured the difference in knowledge and practice before and after the training but the grant reviewer said that we should drop the word “HIV”. They said if we insist to study HIV, we would not get the ethic [ethical approval/IRB]. (Ursine, female, state university) I have never done any research on HIV. I am not sure if I want to do that. I heard that it is difficult to get ethic approval [IRB]. They are [HIV-positive patients] just so vulnerable, we must treat them with caution. (Silene, female, state university)
Selective Acceptance to PLHIV
A study in Malaysia involving 1296 health care students found an alarming rate of stigmatizing attitudes toward PLHIV who has a history of drug use or homosexuality, which was attributed to values and norms.
33
Since Indonesia shares common cultural and spiritual characteristics traits, a similar situation is likely to happen. Indonesia is known to have immense and highly devoted religious involvement among the population. Both cultures and religions share similar values that condemn the practice of homosexuality, extramarital sex, and drug use.
15,40
While diseases are usually seen from the clinical perspectives, there is so much of the interplay of culture and religion that influences actions directed to PLHIV that makes it impossible to leave culture and religion in HIV discourse. Moreover, there is a prevailing consensus of construed negative perception and attitudes to those who were considered to deviate from the standard norms in the general population in Indonesia. The lecturer participants brought up the discussion that somewhat reflected these dominant values of Indonesians. I once assisted my friend in his community service in a HIV care center. I met some HIV people, men. They look normal; people said that they cause the transmission. They are gays. These days, I am very worried. I know that the rapid increase in new cases of HIV in my province is due to homosexuality. There is also that Facebook group circulating [about homosexuality], which I believe increases the risk of HIV transmission to others. I believe we need to take actions to this phenomenon (Heather, female, state university) Everyone can get HIV if he or she does not behave according to the religious norm. That is what I had observed from my patients. I met two of them [HIVpositive patients] and all of them are the same, they have sex with so many people. (Tauri, male, state university) One of my friends posted a picture and story of his HIV-positive patient on Facebook. She was a little girl, the same age as my daughter. She got the disease from her parents. When I read her story, I felt so sad that I almost cried. She reminded me of my daughter. She was small for her age, very thin, and this disease caused her to have low self-esteem. She never played with other kids; so, my friend, who was a psychologist, tried to motivate her. I hope that her parents can learn from this experience. They must contemplate and repent for their sin that brings the problem to their innocent daughter. (Fern, female, private university) I felt a myriad of emotions when dealing with HIV-positive patients. I felt so sad when I met an HIV-positive patient who was a stay at home mother. She is innocent and did nothing wrong that can cause the disease. I must help her. However, when I met one [HIV-positive patient] who works as a prostitute in a brothel, well, I was raised within a highly religious family and I can differentiate the right from wrong. I think they [PLHIV] deserve whatever comes to them. (Iris, female, private university)
Medicalization of HIV
Since the beginning of the epidemic, research in HIV is mostly conducted from the medical perspectives. The early studies were mostly focused on detecting signs and symptoms of the disease to help doctors establish the diagnosis, isolating the virus DNA to develop vaccines, as well as developing drugs and treatment regimen. 43 -45 Most recent studies shift the focus to a larger bounded with health professionals as pivotal elements in HIV care and control.
Few studies discussed HIV from nutrition perspective mostly focused on the effect of nutrition intervention such as supplement on metabolism and nutrition status or explored common nutrition problems among PLHIV.
9,46
-48
Although these studies help promoting the role of dietitian in HIV case management, they even led to the discussion of “medicalized” nutrition. Under these circumstances, the data analysis resulted in one analytical theme that HIV is a medical area. I mainly teach food service management. In this division, we do not really talk about HIV because there is no specific protocol for food service for HIV-positive patients. They can eat everything. Besides, in food service management, we deal with mass food production, not for specific clients like PLHIV. That is why; HIV here is mostly discussed from the clinical perspectives. (Daphne, female, private university) We have covered all aspects of HIV although we do not have one special course allocated for HIV only. We teach them (the students) the biomedical aspects of HIV, immunology, pharmacology, and pathology. Of course, we teach them the NCP [nutrition care process], so they know how to assess nutrition status, diagnose, treat [prescribed diet], and monitor and evaluate the patients’ nutrition status. That is enough, I believe. (Hydra, male, state university) I do not think a HIV and nutrition course is necessary to be offered as a separate subject in our curriculum structure. I believe it is enough for them [the students] to understand the principle of high-calorie high-protein diet for HIV-positive patient. Our current curriculum is adequate to equip them with the work with HIV-positive patients later in the future. Maybe we just need to strengthen what we already have in our clinical nutrition courses. (Fern, female, private university) I teach clinical nutrition at my university. We discuss HIV during the tutorial and the focus of our discussion is the NCP [nutrition care process], we talk about the assessment, diagnosis, intervention, monitoring, and evaluation. The diet prescription for HIV is straightforward; we just need to give them a high calorie and high protein diet. We might need to modify the consistency of the diet if the patients have candidiasis. (Silene, female, state university) I used to teach HIV in our counseling class but with the changes in our curriculum, we lost that course. In that class, we taught counseling for HIV and cancer simultaneously in one meeting because HIV and cancer patients have similar emotional problems. (Dahlia, female, state university) I want to highlight that HIV is a very complex biological process. Our role as dietitians is to prevent those who are infected with HIV from becoming more severe. There is this clinical trial from Thailand reported that nutrition supplementation could improve the survival rate of HIV-positive patients. (Hydra, male, state university) I think the role of dietitians in HIV care in the clinical settings is clear. We can help them maintain their nutrition status by providing a healthy diet during their stay in the hospital. It seems that we can also contribute to the community, although preventing them from getting the virus is not our job. That should be the job for public health practitioners. (Nolana, female, state university)
Reluctance to Discuss HIV
There is one musical terminology comes up while examining the emerging themes from the data in this study; HIV as an intermezzo. The Merriam Webster dictionary defines intermezzo as “a movement coming between the major sections of an extended musical work (such as an opera)” or “a usually brief interlude or diversion.”
55
This musical terminology is reflected in the fact that as much as lecturers want to discuss HIV with their students, they have no opportunity to do that. They must follow the institutional curriculum, which dictated that HIV is not an important topic of discussion among dietetic students. In many instances, participants argued that it is enough to explain HIV in the framework of another aspect of clinical nutrition. HIV can be part of the class that discusses infectious disease, food safety, nutrition care process, immunology, or pathology. We can have an elective class in HIV if we want, but I think we have enough problems in nutrition such as obesity, undernutrition, anemia, and other nutrients deficiencies to learn. I am afraid that if we design a class specifically for discussing HIV, we have not enough credit to teach other subjects that are more important. I think what we have now is enough. I teach HIV as part of my class in immunology. I know that Dr X (a name of lecturer in the university) also mentions about HIV in her class on pharmacology. Dr Y and Dr Z (other lecturers) sometimes also discuss a bit about HIV in their classes. (Hydra, male, state university) Sometimes I insert information about HIV in my class, which is the health administration class. I talk about the prevalence of HIV, health system response, and insurance coverage for HIV. I sometimes also insert HIV when I discuss condoms as a means of family planning in my public health class. I do not really talk about HIV and nutrition. (Elm, female, private university) Their [the students] questions are sometimes ridiculous and trivial. They asked me whether the tattoo could cause HIV. Most of the time, they are just curious about the sexual aspects of HIV. They should already know about that. I cannot believe they ask me those questions. (Daisy, female, private university) We do not really discuss myths and misconceptions of HIV in my class. The students sometimes asked whether it is safe for them if they accidentally touch the sweats of their patients. I think they need reassurance that they would not be infected with the virus during their clinical rotation. We limit our discussion on that and the clinical aspects of HIV. I felt not comfortable when they ask questions and make sexual innuendos. (Hydra, male, state university) We do not let the students take care of HIV-positive patients during their clerkship. Their dietetic supervisors in the hospital also agree with this policy. HIV is very dangerous. It is too risky for them [the students] to handle HIV-positive patients. (Iris, female, private university) There were some students here who got HIV-positive patients during their clerkship, but I think they were scared and uncomfortable so they refuse to treat the patients. They should be okay, though, because we expect that they will just give the diet prescription to the patients, talk a little bit, and then it will be done. However, I can understand their fear and discomfort in taking care of HIV-positive patients. They should wear a mask while talking to the patients. I understand that [the refusal]. (Silene, female, state university) For my anthropology class, I sent a group of students to visit a red-light district in our province to learn about the livelihood of the community members. They can also learn about HIV there. Before they went there, I told them “Go in groups, not alone, not in pairs. Just in case something happens, then, you can help each other.” Those people [in the red-light district] are very dangerous and the place is scary. I told them that they should not hang out in those shady places because the effect will be harmful to their reputation. I was scared of sending the students there [the red-light district]. I also sent another group of students to visit shelters for homeless kids. Again, that place is also very risky, so I warned them multiple times. I told them to bring the institutional cover letter and their alma mater jacket for protection. (Tauri, male, state university)
We found that by highlighting the danger of interacting with HIV key populations multiple times, denying opportunities to treat the patients, and refusing to remedy their prejudicial attitudes through class discussion; lecturers are likely to do more harm to stigma reduction efforts. The Italian study on HIV stigma suggests that educators can act as an agent of change by teaching comprehensive knowledge about HIV to health workers, which include methods of HIV transmission, the use of safety procedures, post exposure prophylaxis, and professional behavior. 56 Additionally, educators could create more opportunities for health care students to work with PLHIV and thus improving awareness and acceptance toward the individuals.
The World Health Organization (WHO) underlines that health care providers’ responsibilities are pivotal in HIV treatment, prevention, case management, and stigma reduction. The WHO reported that often times, efforts to control the epidemic are hindered by a lack of trained health professionals. 57 Furthermore, from the increasing report of negative attitudes, stigma, and unfavorable behaviors of health workers and students toward PLHIV, 1,2,6,10,33 it is clear that HIV discussion in the classroom should go beyond the medical or clinical aspects of the disease. It indicates the need to reform HIV discussion in the classroom, in which lecturers need to discuss HIV from a wider perspective and open discourse to sensitive aspects of HIV such as ethics, morals, stigma to address the students’ fear or anxiety toward PLHIV. They need to inspire their students on professional behavior and integrity.
The Symbolic Meanings of Teaching HIV
Symbolic interactionism focuses on explaining how people define and give meaning to their experiences through their social interaction with other people. From this perspective, human behavior at the present times is determined by what happened in the past. 18,58 We sought to identify the experiences of lecturers using this theory, and the results revealed that their experiences are full of restrictions on the attribution of HIV among the general population. We found 2 underline factors to the symbolic meaning of HIV that considers HIV is a restricted area for a dietetic student to enter.
First, participants’ lack of access to comprehensive HIV information in the past contributes to a similar practice in their current academic career. They limited themselves from learning more about HIV through professional development activities or research, and when they met with obstacles along the way, they quitted the effort altogether. Since HIV was considered a medical problem primarily for a long time, they refused to perform their Tri Dharma (teaching, research, and community services) on HIV beyond that area. On the other hand, in their capacity as lecturers, participants also seemed to put similar restrictions on their students to have more access to HIV resources. They refused to discuss HIV out of the clinical context and prevent their students from taking care of HIV-positive patients during their clerkship. They implemented the same curriculum design as the one that they experienced in their past dietetic training without recognizing the need to innovate and improve it considering the advancement in HIV research. A study among doctors and nurses in Lao PDR concluded that missed opportunities to learn about HIV could undermine efforts to control HIV. 16
Second, adherence to cultural and religious values are likely to impose a restriction to discuss HIV to the students. Participants’ main concern is the sexuality aspect of HIV because sex is treated as a very private matter and culturally regarded as a taboo topic in Indonesia. Discussion about sexuality often occurs only within the frame of marriage and resulted in an unwillingness to discuss HIV in public. 15 This explains the reluctance and discomfort feelings that the participants’ experienced during HIV discussion in class. Conversely, some religious and cultural teachings deliver messages that condemn certain key populations of HIV and contradict intervention to prevent HIV. 15,40,59 Social isolation imposed on HIV individuals and refusal to HIV prevention method become common practices so that encouraging acceptance to those topics might be seen as disconformities to social norms. As opposed to the Western culture, the Asian culture, in general, seeks conformity instead of presenting individual uniqueness to avoid discord in harmony. 60 The preference to conformity explains the participants’ implicit teaching about selective acceptance toward PLHIV. In this case, the act of teaching HIV symbolizes one’s moral character and adherence to religious beliefs, thus, in that sense presented lecturers with the social dilemma of being an agent of change in HIV control.
Limitations of the Study
This study was conducted in 3 universities in Indonesia with a sample size of 13 lecturers in dietetic schools. Participants in these universities might be different from other lecturers in other universities regarding their HIV awareness and acceptance. However, one must not seek generalization from a qualitative study. Additionally, there is a possibility that the participants provide answers that are favorable to avoid judgment and satisfy the researcher. However, the use of multiple techniques of data collection ensures the credibility of responses and the trustworthiness of data analysis. Moreover, close personal contact between the researcher and the participants is likely to establish a trust that encourages participants to share their truthful experience and perception.
Conclusion
HIV discourse in dietetics schools in Indonesia is very limited. It focuses only on providing information related to the medical aspects, biological pathways, and essential treatment of HIV. Examining the experiences of lecturers provides insight into the reason behind this situation, where HIV is regarded as a restricted area for dietitians. This restriction is a result of a lack of access to HIV resources as well as conformity to the social norms that lead to selective acceptance to PLHIV. Consequently, participants impose further restrictions on their teaching conduct on HIV to their students. The focus of their teaching is limited to the technicalities of nutrition care and devoid of the humanistic aspects of HIV.
Considering the increasing report on stigmatized attitudes among health workers, lecturers need to be health advocates to promote acceptance and reduce stigma among their students. Lecturers might need to recognize their own ingrained personal beliefs and values about HIV before teaching the topic. Acknowledging personal bias might help them improve their teaching conduct.
Footnotes
Appendix A
Acknowledgments
The authors thank the Graduate School of Kansas State University for providing financial support. The authors would like to acknowledge and thank all study participants and all academic officers from the 3 dietetic schools in Indonesia for assisting the study team to connect with the study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 2017 Arts, Humanities and Social Sciences Small Grant Program from The Graduate School of Kansas State University.