
Abstract
Background
Despite advancements in HIV treatment modalities, HIV-related stigma among healthcare providers (HCPs) persists, impacting people living with HIV.
Methodology
A cross-sectional research design with a non-probability consecutive sampling technique was used to assess HIV-related stigma, and its association with individual characteristic, fear, and knowledge of HIV among 100 HCPs at a university hospital in Nepal.
Results
The average age was 29.83 years, with work experience of 84.24 months. The fear score was 14.11, and the HIV knowledge score was 36.74. The stigma reflected a moderate stance. Age (rs = −0.22, P < .05) and work experience (rs = −0.29, P < .01) negatively correlated with stigma, while fear positively correlated (rs = 0.45, P < .01), and no correlation was observed with HIV knowledge.
Conclusion
HCPs’ age, work experience, fear, and marital status are linked to HIV-related stigma. Interventions should tailor stigma reduction strategies considering these factors.
Introduction
Human immunodeficiency virus (HIV) remains a global health challenge, affecting approximately 39.0 million people in 2022 with 630 000 deaths due to HIV worldwide. 1 Although advancements in HIV testing and medication have transformed it into a manageable chronic condition, persistent stigma and discrimination hinder testing, treatment, and care.2–6
Studies show that people living with HIV (PLHIV) often face stigma within healthcare settings, primarily from healthcare providers (HCPs), even during non-HIV-related hospital visits.7–10 More than half of HCPs display at least 1 stigmatizing attitude toward PLHIV. 11 Examples include refusal to care, ignorance and differential in treatment, physical isolation, verbal abuse, and unnecessary use of gloves regardless of physical contact.12–15 Doctors and nurses, as primary HCPs, take oaths to care for patients regardless of health conditions. However, previous studies show they often hold stigmatizing attitudes towards PLHIV.16,17 In Nepal, qualitative studies reveal similar issues where doctors and nurses compromise the quality of care for PLHIV in non-HIV clinics.10,18
The literature reveals that HCPs’ age, sex, professional category, education, work experience, area of work, knowledge of HIV infection, fear of contact with HIV, and inadequate continuing training regarding HIV are associated with stigmatizing behaviors.19–22 However, limited evidence exists on HIV-related stigma among HCPs in Nepalese healthcare settings. Anecdotal evidence and occasional newspapers report provide only a glimpse of the issue, with little comprehensive information available. To address HIV-related stigma in Nepal's healthcare settings, it is crucial to assess its extent and explore associated factors.
Therefore, this study aims to assess HIV-related stigma among HCPs, exploring associations with their characteristics (age, gender, marital status, professional categories, work experience, and HIV-related training), fear of contact with HIV, and knowledge of HIV. By uncovering the extent and factors contributing to stigma, the study seeks to inform plans and policies for stigma reduction in healthcare. Ultimately, the findings can guide interventions to improve HCPs attitudes and behaviors toward PLHIV, enhancing overall care quality.
Methods
A descriptive correlational study with a cross-sectional research design was conducted at a University Hospital, a 475-bed multi-specialty Hospital in Nepal, where 1245 staff, including 339 nurses and 227 doctors were employed. The non-probability consecutive sampling technique was employed to collect data.
The study focused on doctors and nurses at a University Hospital who had provided care for PLHIV during their clinical practice and were willing to participate. The sample size was calculated using G* power 3.1.9.2, setting an acceptable level of statistical significance set at α = 0.05, effect size = 0.30, and power = 0.80 with 2-tailed direction, 23 considering a 20% attrition rate. 19 The final sample size was 100.
Data were collected using a self-administered questionnaire from February to April 2020. The first author approached the participants during their break and asked them to complete the form. All participants completed the form and returned it on the same day. The response rate was 100%.
The socio-demographic-related questionnaire was adapted from previous studies.11,17,22,24,25 HIV-related training, representing formal training on HIV infections received by HCPs. Participants were asked if they had attended any certified workshops, seminars, or short-term courses organized by national and international organizations. Those who answered yes were further asked about the duration of their training.
The perceived fear of contracting HIV while caring for PLHIV, termed “Fear,” was measured using a tool adapted from Nyblade et al. 26 The 11-item questionnaire utilized a rating scale ranging from “0” to “3,” with 0 = not worried, 1 = a little worried, 2 = worried, and 3 = very worried, with total scores ranging from 0 to 33, higher scores indicating greater fear. The content validity index (CVI) of a tool was 1 and the reliability was calculated using Cronbach's alpha coefficient, resulting in 0.85.
Knowledge of HIV was assessed through a self- administered questionnaire adapted from previous study. 27 The 46 questions covered basic knowledge, preventive measures, transmission, and treatment. Participants received 1 point for a correct answer and 0 for an incorrect or ‘do not know’ response with scores ranging from 0 to 46. A higher score indicates more excellent knowledge of HIV. The CVI of a tool was 1. The reliability was calculated using Cronbach's alpha coefficient, resulting in 0.73.
The dependent variable, HIV-related stigma, was measured using The Health Care Provider HIV/AIDS Stigma Scale (HPASS) developed by Wagner et al. 28 The 30-item questionnaire included 3 subscales: stereotyping (11 items), discrimination (6 items), and prejudice (13 items). Participants responded on a 6-point Likert scale, with strongly disagree = 1 and strongly agree = 6. The calculated mean score of a single item of HPASS could range from 1 to 6, with lower scores indicating a lower level of stigma and higher scores indicating a higher level of stigma. The overall reliability of HPASS was confirmed with a Cronbach's alpha coefficient of 0.94. In this study, the Cronbach's alpha of HPASS was 0.93.
Data analysis was performed using Statistical Package for Social Sciences (SPSS) statistics, version 21. Descriptive statistics, including frequency distributions, percentages, means, ranges of scores, and standard deviations, were utilized to analyze individual characteristics, fear, knowledge of HIV, and HPASS. Since the data were not normally distributed, Spearman's rank-order correlation (rs) was computed to examine relationships between HCPs’ age, work experience, fear of contracting HIV, and knowledge of HIV with HIV-related stigma. While an independent t-test was used to examine the differences in mean score of HIV-related stigma based on gender, marital status, professional category, and HIV-related training of HCPs.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Ethical Clearance Committee on Human Rights Related to Research Involving Human Subjects, Faculty of Medicine Ramathibodi Hospital, Mahidol University, No. MURA219.1253 and the Institutional Review Committee of Kathmandu University School of Medical Sciences (KUSMS-IRC), No. 04/20. Written consent was obtained from all the participants before collecting data.
Results
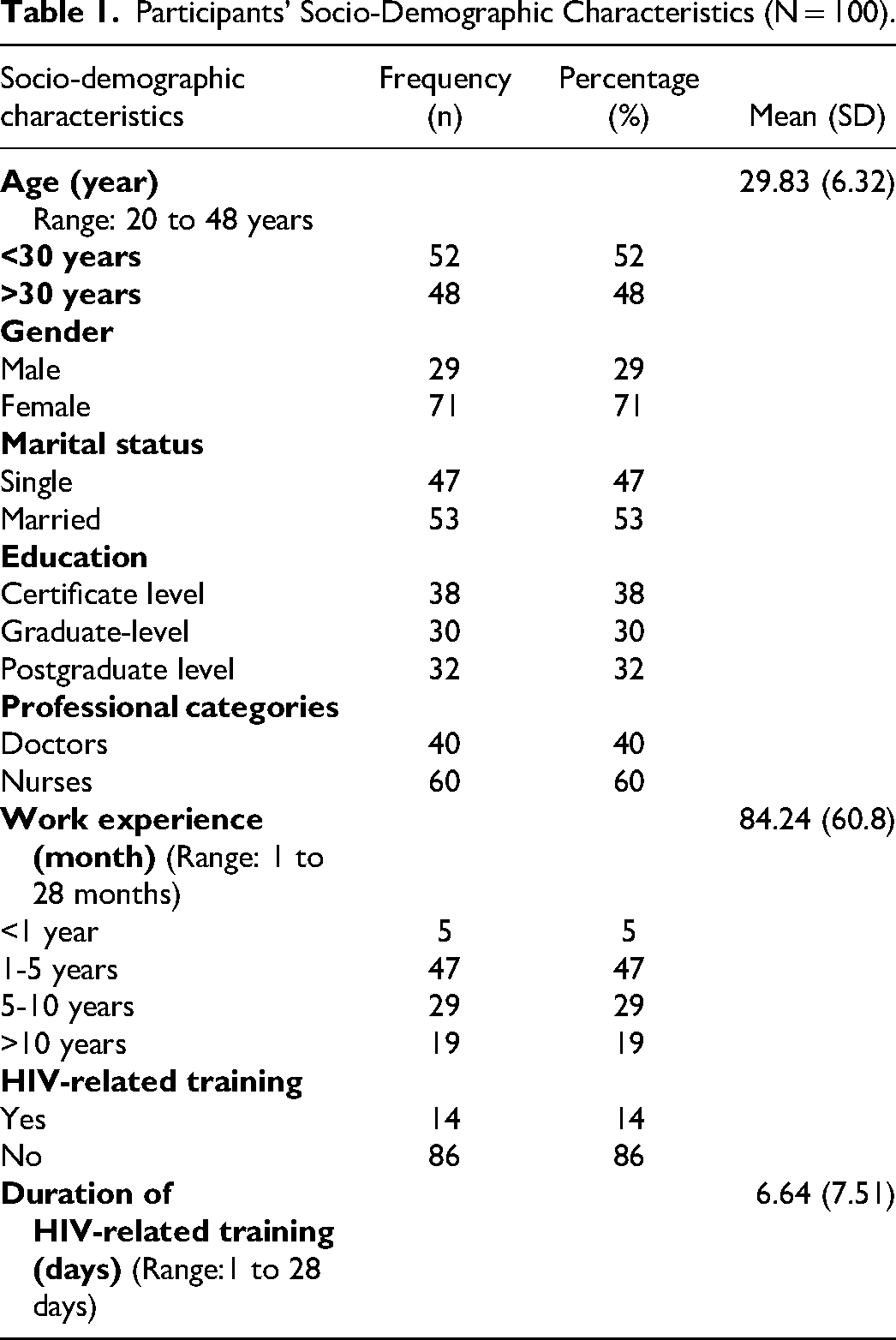
A total of 100 participants were enrolled, with a mean age of 29.83 years (SD = 6.32). The majority were female (71%), and 53% were married. Educational levels varied, with 38% holding a certificate, 32% postgraduate, and 30% graduate degrees. The participants comprised 60% nurses and 40% doctors, with a mean work experience of 84.24 months (SD = 6.32). Only a few had HIV-related training, lasting an average of 6.64 days (SD = 7.51) (Table 1).
Participants’ Socio-Demographic Characteristics (N = 100).
The participants had a mean fear score of 14.11 (SD = 7.26). Higher mean scores were noted in situations involving direct blood contact, such as assisting in surgical procedures (Mean = 2.23, SD = 0.91), drawing blood from a PLHIV (Mean = 1.99, SD = 0.93), and establishing an intravenous line (Mean = 1.86, SD = 0.91). Lower mean scores were observed in non-invasive procedures like taking temperature (Mean = 0.50, SD = 0.73), performing a physical examination (Mean = 0.78, SD = 0.82), and touching clothing (Mean = 0.79, SD = 0.90) (Table 2).
Description of Fear of the Participants (N = 100).
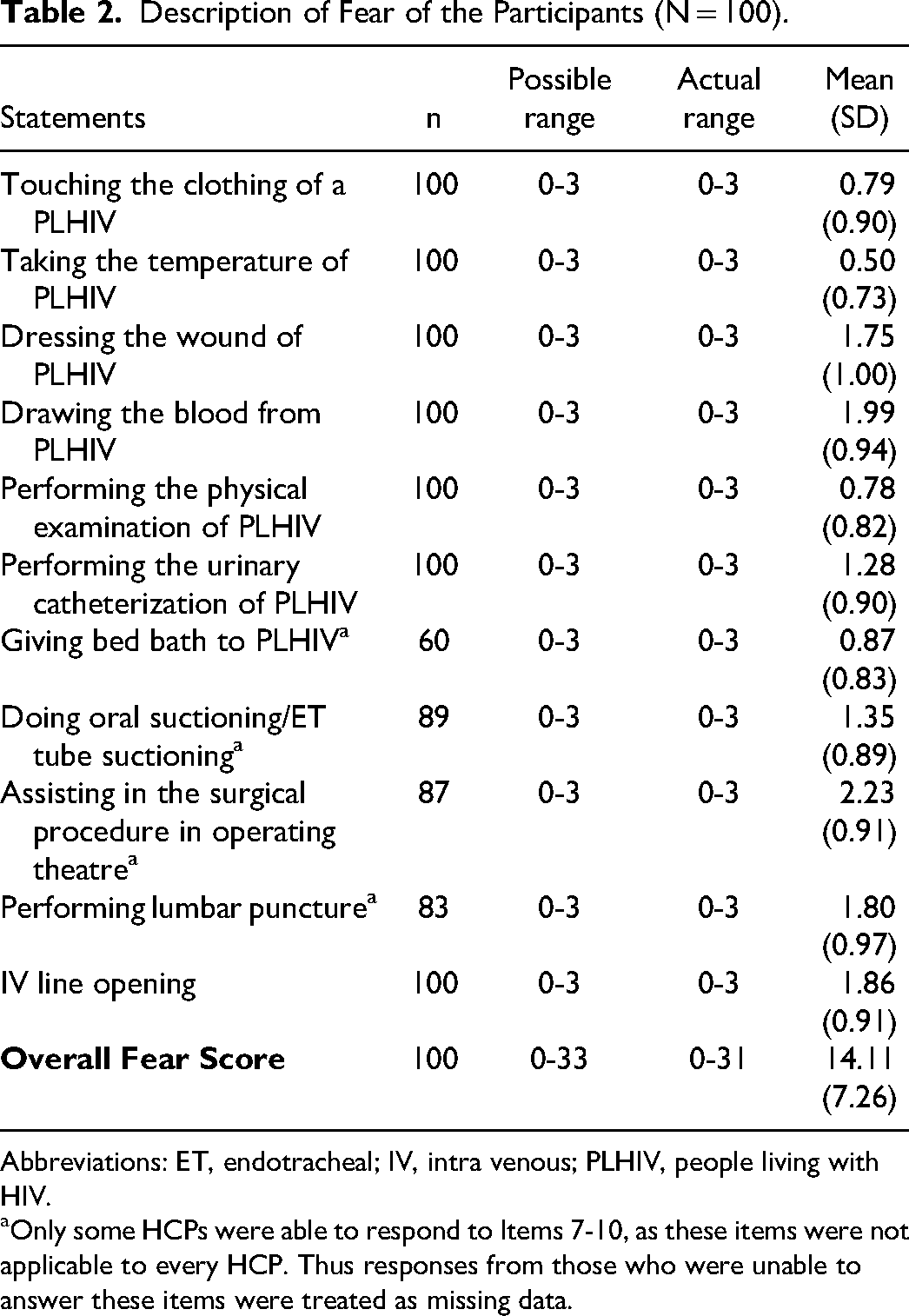
Abbreviations: ET, endotracheal; IV, intra venous; PLHIV, people living with HIV.
Only some HCPs were able to respond to Items 7-10, as these items were not applicable to every HCP. Thus responses from those who were unable to answer these items were treated as missing data.
Out of 46, the mean HIV knowledge score was 36.74 (SD = 4.78) indicating higher level of knowledge on HIV. Participants had good basic knowledge of HIV, while their knowledge of treatment was not good. Knowledge of prevention and transmission showed more variability (Table 3). More than half answered incorrectly about preventing HIV transmission and other blood-borne infections. Only, 66 (66%) of the participants answered correctly that the risk of HIV transmission following a needle stick or sharps injuries was minor, approximately 0.3%, while only 59 (59%) of them correctly answered that the risk of HIV transmission following a splash of blood to non-intact skin or mucus membranes is minimal, approximately 1 in 1000 (Supplemental Table 1).
Description of Knowledge of HIV and HIV-Related Stigma of the Participants (N = 100).
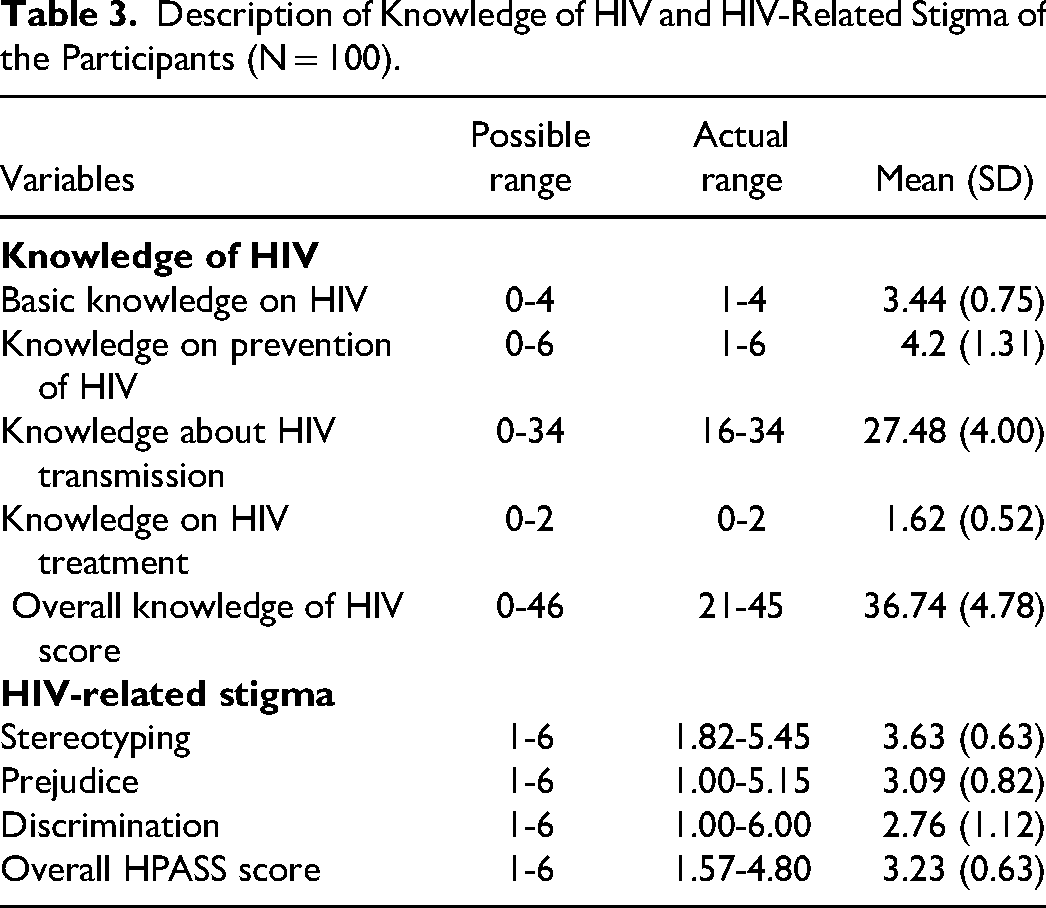
The mean HPASS score was 3.23 (SD = 0.63), indicating a stance between somewhat disagree and somewhat agree. The highest mean scores were on the stereotyping subscale (3.63), and the lowest were on the discrimination subscale (2.76) (Table 3). The stereotyping statements with the highest mean scores were; “I believe most PLHIV acquired the virus through risky behavior” (Mean = 4.53, SD = 1.43) and “I think if people act responsibly, they will not contact HIV” (Mean = 4.35, SD = 1.50). Similarly, the discriminating statements with the lowest mean scores were; “I would avoid conducting certain procedures on PLHIV” (Mean = 2.38, SD = 1.270) and “I believe I have the right to refuse to treat PLHIV for the safety of other patients” (Mean = 2.48, SD = 1.57) (Supplemental Table 2).
The study found a significant negative correlation between age (rs = −0.22, P < .05) and work experience (rs = −0.29, P < .01) with HIV-related stigma. Specifically, as the age and work experience of participants increased, the level of HIV-related stigma decreased. A positive relationship was observed between fears of contracting HIV and HIV-related stigma. However, no significant relationship existed between HIV knowledge and HIV-related stigma (Table 4).
Correlation Between age, Work Experience, Fear, and Knowledge With HIV-Related Stigma.
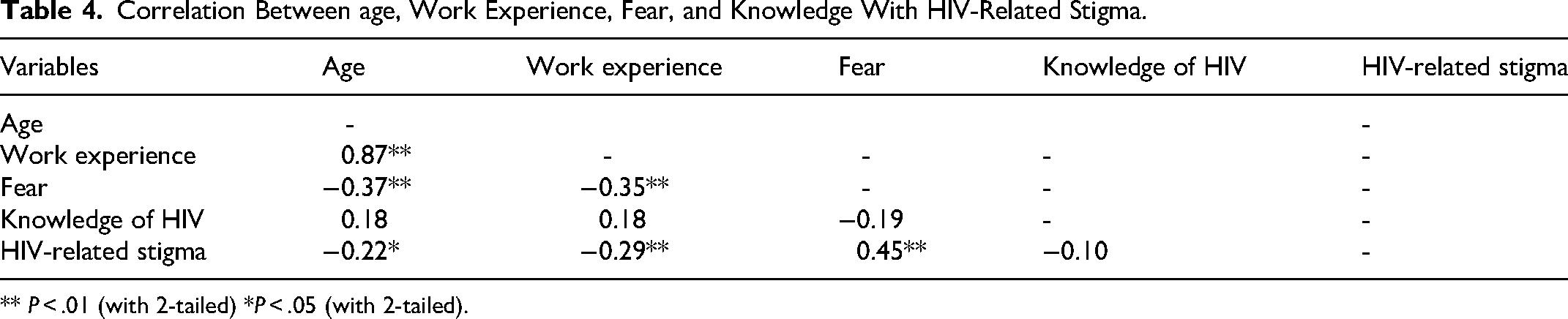
** P < .01 (with 2-tailed) *P < .05 (with 2-tailed).
An independent t-test revealed no differences in stigma based on gender, professional category, and HIV training. However, significant differences were found in stigma scores between single and married participants (Table 5).
Differences in the Mean Scores for HIV-Related Stigma Across the Dichotomous Variables.
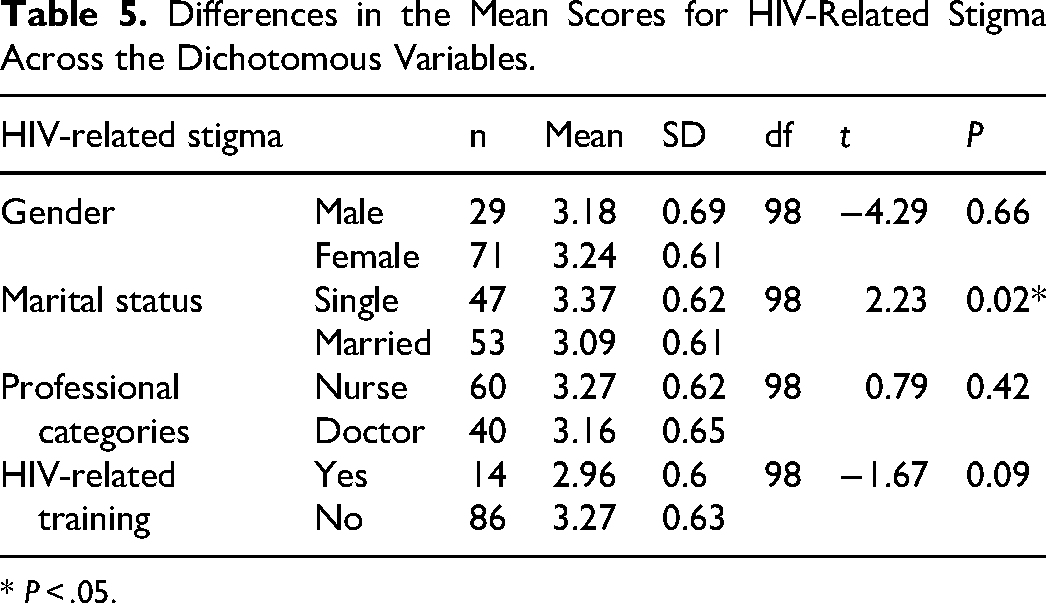
* P < .05.
Discussion
The study aimed to examine HIV-related stigma among HCPs at a university hospital in Nepal and investigate associations between individual characteristics of HCPs, fear, and, knowledge of HIV with HIV-related stigma. Similar to prior research,11,29,30 this study found the presence of HIV-related stigma among HCPs. PLHIV infected through illicit drug use and unsafe sex experienced more stigma than those infected through blood transfusions, aligning with perceptions from other studies attributing HIV infections to high-risk behaviors.11,16,25,29–32 These negative attitudes towards HIV are due to the stereotypical association of HIV with high-risk behaviors, such as sexual promiscuity, and moral affairs, such as homosexuality and drug abuse. 33 In line with earlier studies,16,25,31,34 most participants were comfortable working with colleague PLHIV. However, they expressed fears of contracting HIV from patients, preferring limited physical contact, preferring HIV-negative patients, and using extra precautions. Despite this, participants disagreed with the right to refuse treatment, citing the contagious nature of the disease, fear of illness, and death as possible explanations. 33 Additional training on HIV and standard precautions could help mitigate HIV-related stigma among HCPs. 35
Current study revealed an inverse association between HCPs’ age and HIV-related stigma, consistent with previous research.36–38 The possible reason could be, with an increase in age, HCPs become more mature, more responsible, and strictly follow the professional code of conduct. 36 Moreover, older HCPs may have accurate information about standard medical protection procedures and can easily access institutional support compared to the younger ones. 37 Regarding marital status, married participants showed lower HIV-related stigma compared to single participants, in line with previous studies.30,31 Possibly due to the stability of a marital relationship promoting more logical treatment of PLHIV. 28 In contrast to previous studies,11,17,39 current study did not find any significant differences in HIV-related stigma among the gender and professional categories. It could be assumed that the inconsistencies across the different dimensions and domains of HIV-related stigma across the studies might be the origin of the disparity between the findings of the current and earlier studies. Current study noted a negative association between work experience and HIV-related stigma, consistent with prior studies.13,19,40 Increased exposure to PLHIV during work may enhance competence in managing and preventing HIV, thereby reducing stigma. Contrary to previous studies,17,36,39 no significant relationship between HIV knowledge and training with HIV-related stigma was found in this study. As stigma is a personal feeling, knowledge of HIV alone might not be the sole reason for minimizing HIV-related stigma. 41 This could also be related to the contagious nature of the disease and the fear of contracting HIV while providing care.21,24,29 This is further supported by the current study, where the fear of HIV infection while caring for PLHIV was positively associated with higher HIV-related stigma, emphasizing the importance of continuous education on HIV transmission prevention and the necessity of policy guidelines related to HIV infection and stigma in healthcare settings.29,42
The study results serve as a foundation for future research, although limitations include the use of purposive sampling and the focus on doctors and nurses, which may limit generalizability. Future studies should diversify samples and explore a wider range of HCPs for enhanced applicability and comprehensiveness.
Conclusion
HIV-related stigma among HCPs can impact the quality of care provided to the PLHIV. Among younger HCPs, having less work experience and having a fear of getting HIV while caring for PLHIV are associated with HIV-related stigma. Thus, stigma reduction interventions must be tailored to reduce the fear of contracting HIV while caring for PLHIV. The age, work experience, and marital status of the HCPs must be considered while designing and conducting any stigma reduction interventions. Targeted interventions should include counselling and educational programs for younger, less experienced, and single HCPs. These programs should focus on interacting with PLHIV, addressing fears of HIV transmission, and strategies to overcome stigma. By enhancing confidence in providing care, these interventions will improve the overall quality of care for PLHIV and foster a more supportive and informed environment for both providers and patients.
Supplemental Material
sj-docx-1-jia-10.1177_23259582241282583 - Supplemental material for Factors Associated With HIV-Related Stigma Among Healthcare Providers at a University Hospital in Nepal
Supplemental material, sj-docx-1-jia-10.1177_23259582241282583 for Factors Associated With HIV-Related Stigma Among Healthcare Providers at a University Hospital in Nepal by Pratima Wenju Shrestha and Poolsuk Janepanish Visudtibhan, Sasisopin Kiertiburanakul in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
Special thanks are extended to Dhulikhel Hospital, Kathmandu University Hospital for granting permission to conduct this study and heartfelt gratitude is expressed to all the participants for their invaluable participation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Ethical Clearance Committee on human rights related to research involving human subjects of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University (MURA2019/1253), and the review board of Kathmandu University School of Medical Sciences Institutional Review Committee (approval no. 04/20). Written consent was taken from participants and confidentiality was assured before seeking consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.