
Abstract
Background:
Stigma shapes the lives of people living with HIV and may affect their willingness to seek medical care. But treatment delays can compromise health and increase the risk of transmission to others.
Purpose:
To examine whether the 4 stigma manifestations—enacted (discrimination), vicarious (hearing stories of discrimination), felt normative (perceptions of stigma’s prevalence), and internalized (personal endorsement of stigma beliefs)—were linked with delays in seeking care among HIV-infected people in India.
Methods:
A cross-sectional survey was conducted with 961 HIV-positive men and women in Mumbai and Bengaluru.
Results:
Enacted and internalized stigmas were correlated with delays in seeking care after testing HIV positive. Depression symptoms mediated the associations of enacted and internalized stigmas with care-seeking delays, whereas efforts to avoiding disclosing HIV status mediated only the association between internalized stigma and care-seeking delays.
Conclusion:
It is vital to develop stigma reduction interventions to ensure timely receipt of care.
Introduction
Stigma against HIV profoundly shapes the lives of people living with the disease. It leads to discrediting and discrimination against individuals who have the disease. 1 –4 Stigma’s effects are particularly pernicious when they influence people’s access to, or quality of, health care. In an era of successful antiretroviral (ARV) therapies, forgoing or delaying care compromises health and increases the potential for onward transmission of the virus. 5,6 Unfortunately, studies from around the world have demonstrated how stigma influences care practices. It shapes the attitudes of providers who deliver services 7,8 and at times leads to outright denials of care or mistreatment while in care settings. 9
In its most overt form, stigma manifests as interpersonal acts of discrimination, or what theorists call enacted stigma. 10 However, these enactments represent only a part of the overall picture. More comprehensively, stigma is a systemic and pervasive mechanism by which interactions and behaviors are regulated. 11 It is a socially shared phenomenon that exists within and among a community or set of people. In our work in India, we have found it critical to examine 4 specific forms or manifestations of HIV stigma: two interpersonal and two intrapersonal. 12,13 The interpersonal types include the aforementioned enacted stigma (discrimination), as well as what we have labeled vicarious stigma—heard stories or witnessed events that provide evidence of how others known to have HIV have been treated. 13 These interpersonal forms shape the two intrapersonal manifestations. Felt normative stigma consists of people’s perceptions about the prevalence of HIV stigma in the local community and their expectations that it will influence social interactions. 13 And internalized stigma is composed of people’s personal endorsements of stigmatizing beliefs. For individuals living with HIV, it is a form of self-judgment, in that they believe that prejudice or stigma against themselves is warranted and appropriate. 14,15
Recognizing and examining all 4 forms is critical to understanding the full impact of stigma. As an example, although there exist sometimes dramatic occurrences of discrimination and prejudice, 16,17 such events are in fact relatively rare in the lives of many people living with HIV. 12,13 If measuring only such enactments, one might be led to the incorrect conclusion that stigma has relatively little impact on HIV-infected individuals. But, in fact, the infrequency of discriminatory acts is due principally to the influence of intrapersonal manifestations of stigma. Because HIV-infected people believe that others hold prejudicial beliefs (felt normative stigma) and because they may personally endorse such beliefs (internalized stigma), they often go to great lengths to avoid disclosure of their HIV serostatus. 12,13,18 As a result, people with HIV infrequently encounter direct hostility or discrimination because in most situations they are not known or perceived to have the disease.
In our previous work, we were able to demonstrate mental health consequences of intrapersonal forms of stigma, by showing that these manifestations were associated with depressive symptoms, a relationship fully mediated by disclosure avoidance behaviors. 13 But we were not able to examine whether a link existed between stigma and receipt of care. In this article, we look specifically at the relationship between HIV stigma and delays in seeking care among a general sample of HIV-infected individuals recruited from diverse settings in two urban areas in India. In other parts of the world, stigma-related delays in care are known to exist and to have critical effects on health outcomes. 19 In the work reported here, we look at whether manifestations of stigma are linked with reported delays in seeking care, and at whether such a relationship is mediated by disclosure avoidance and depressive symptoms, both of which have been shown to associate with stigma in our prior work. 12,13
Methods
Participants
We recruited participants from two urban areas in India: Bengaluru (formerly Bangalore) and Mumbai. To be eligible, individuals had to self-report diagnosis with HIV/AIDS, be able to speak English or a local language (Kannada or Tamil in Bengaluru and Hindi or Marathi in Mumbai), and be at least 18 years of age. To ensure diversity, we sampled from a variety of settings, including nongovernment organizations (NGOs) serving people living with HIV and AIDS services organizations (ASOs). In Mumbai, we also recruited in hospitals. By utilizing diverse settings, we were able to enroll individuals who were not necessarily in active medical care, to strive for gender balance, and to oversample harder-to-reach subpopulations (eg, HIV-positive individuals who are also men who have sex with men or women engaged in sex work).
Recruitment in NGOs and ASOs followed similar protocols. At the agencies, study personnel explained the study to local staff and providers and supplied flyers with study information. Both NGO and ASO staff then referred eligible patients to study personnel. In some cases, the interviewers were able to sit in a private room at the organization and meet with interested individuals. In other cases, referred patients called a study phone line and made appointments with the interviewers.
Health care settings included government hospitals, private for-profit hospitals, not-for-profit government hospitals, and freestanding clinics. In these settings, we specifically recruited in units where HIV-positive patients, who may or may not have been on ARV medications, sought medical services. (Enrolling individuals for an HIV-specific study in non-HIV wards would have run the risk of disclosing participants’ serostatus. Many Indian hospital waiting rooms are configured so that patients waiting for appointments can see the individuals with whom other patients are interacting.) Following initial pilot testing of procedures, we decided to approach everyone who was likely to have at least a 1-hour wait. Patients with less than 1 hour wait were generally not interested in participating as they feared losing their place in line. Furthermore, it was not feasible to interrupt and resume an interview, as many patients could not return after their appointments because they had to obtain prescriptions, complete laboratory work, or return home.
Regardless of recruitment location, all study procedures were conducted in private spaces and consent was obtained by study personnel. Participants were asked to complete a structured interview consisting of our various research measures. Trained interviewers read each question to a participant and recorded the person’s answer on the interview form. Participants were provided with a small monetary token of appreciation for their time. Procedures were approved by the institutional review boards at the Tata Institute of Social Sciences (Mumbai), the National Institute of Mental Health and Neurosciences (Bengaluru), and the University of California–San Francisco, and received clearance from the Indian Council of Medical Research and Health Ministry Screening Committee.
All interviewers were required to undergo training that included basic information about HIV, good interviewing techniques (eg, remaining nonjudgmental, asking each question as it is written on the page), research ethics, and an introduction to the protocols specific to this study. Interviewers also conducted mock interviews prior to working in the field. Interviewers were supervised by study investigators to ensure that they adhered to protocols and evidenced good interviewing skills.
Measures
The instruments to measure enacted, vicarious, felt normative, and internalized stigma have been described previously in detail. 13 For convenience, we offer brief descriptions here. Subsequently, we describe the measures we used for potential correlates of stigma.
Enacted stigma
Ten items measured whether participants had experienced discriminatory acts because of HIV (eg, Has someone threatened to hurt you physically because you have HIV?). Response options were 0 (no) or 1 (yes). Because there is little conceptual reason to believe that responses on the measure would be driven by a single underlying construct (rendering interitem reliability statistics inappropriate), we treated the measure as an index of past experience and scored it by summing item responses.
Vicarious stigma
Ten items captured the frequency with which participants had heard about people being mistreated because of HIV (eg, How often have you heard stories about people being forced by family members to leave their home because they had HIV?). Responses ranged from 0 (never) to 3 (frequently). Answers were averaged for scoring (Cronbach α = .86).
Felt normative stigma
Ten items assessed participants’ perceptions of the prevalence of HIV stigmatizing attitudes. (eg, In your community, how many people avoid visiting the homes of people with HIV?) Responses were given on a 4-point scale ranging from 0 (no one) to 3 (most people). Answers were averaged for scoring (α = .91).
Internalized stigma
Ten items captured whether participants believed that they should be treated in a discriminatory manner or be a target of stigmatizing beliefs. Using a 4-point scale running 0 (not at all) to 3 (a great deal), participants responded to questions such as, How much do you feel that you should avoid visiting people because of your HIV? Items were averaged for scoring (α = .85).
Disclosure avoidance
We used a 14-item measure to assess the use of strategies to avoid revealing one’s HIV infection. 13 Examples included describing one’s illness as tuberculosis and seeking care away from the local community. Participants used a 4-point scale ranging from 0 (never) to 3 (often) to indicate the frequency with which they employed each disclosure-avoidance technique. Scores were derived by averaging responses (α = .82).
Depressive symptoms
To assess depression symptoms, we included a variant of the Beck Depression Inventory, Version I (BDI; α = .90), which had been validated previously in India. 20 The Indian BDI uses the same items as found in the United States, but with minor wording modifications to reflect local cultural norms or to make statements more understandable in local languages.
Delays in care seeking
Participants were asked to indicate whether they had ever delayed seeking treatment since testing positive for HIV (response options: 0 [no], 1 [yes]). Those who answered yes were then asked why the delay had occurred. The reasons were divided into 2 categories. Three items were explicitly tied to fear of stigma (Was it [delaying treatment] out of fear of stigma and discrimination? Was it out of fear of how you perceived health care staff would react? and Was it out of fear of disclosure to others?). The other 7 responses related to available resources and were not overtly tied to stigma (lack of money to buy medicines, lack of money to travel, no time to go to the doctor, too far away from the clinic, no one to take care of family or children, unable to take leave from work, and unable to find anyone to accompany them to the hospital or clinic). Based on these responses, we created 2 indicator variables. Participants were scored (1 = yes, 0 = no) as having stigma-induced care delays if they answered yes to one or more of the 3 fear of stigma items. Participants were scored as having resource-induced care delays if they answered yes to one or more of the 7 resources-related items.
Participant demographic characteristics
Individuals were asked to describe their gender, age, marital status, employment status, monthly income, education, and years since testing HIV seropositive.
Analyses
We initially examined the overall pattern of bivariate associations among stigma, disclosure avoidance, depression symptoms, and care-seeking delays using Pearson Product Moment Correlations for associations between continuous variables and Spearman rho for associations with ordinal variables. We then employed logistic regression modeling to examine the potential mediators of the relationship between stigma and care delays. More specifically, we looked for evidence of potential mediation by first examining the strength and significance of the bivariate association between a form of stigma (eg, enacted stigma) and care-seeking delays, and then looking to see whether the significance of this association was lessened or eliminated when adding potential mediating variables to the model. To validate our regression results, we then subjected the same associations to bootstrapping methods that allowed us to test whether the mediated indirect pathways (from stigma to delay in care seeking by way of a mediator) were statistically significant. 21 Bootstrapping involves “repeatedly sampling from the data set to estimate the indirect effects in each resampled data set. By repeating this process thousands of times, an empirical approximation of the sampling distribution …[is] built and used to construct confidence intervals for the indirect effect.”21(p880)
Results
We enrolled a total of 961 HIV-infected participants—511 from Bengaluru and 450 from Mumbai. Table 1 presents demographic characteristics. On average, participants were 33 years old (range 18-68), had 1.49 children (range 0-6), and a median income of 3000 rupees per month (interquartile range: 2000-5000 rupees/month). They had been diagnosed with HIV an average of 4.25 years before their interview (standard deviation [SD] = 3.36; range: 0.01-22.11 years). Slightly over half were currently on ARV medications (Table 1). A substantial proportion (26.5%) reported being widowed, a finding potentially due to the spouse having also been infected with HIV. Sixty-four participants described their marital status as “deserted.” Of these individuals, 52 (82%) were women.
Characteristics of the Participants (N = 961).

Associations among Stigma, Disclosure Avoidance, and Delays in Care
As noted in the methods, we created 2 indicator variables to represent care-seeking delays: (1) those attributed explicitly to stigma and (2) those attributed to a lack of resources. As shown in Table 2, approximately 11% of the sample reported some sort of delay in obtaining care. Relatively more participants attributed their delays to a lack of resources than to stigma. We initially examined the associations with each kind of care-seeking delay. However, our findings revealed that the pattern of relationships was identical regardless of the category of reason to which participants attributed the delays. Therefore, we collapsed the findings into one outcome indicator variable for purposes of the remaining analyses. Participants were scored as having had a care-seeking delay if they reported having deferred obtaining treatment for any reason.
Percentage of Participants Reporting Care-Seeking Delays Resulting from Stigma or Lack of Resources (N = 961).
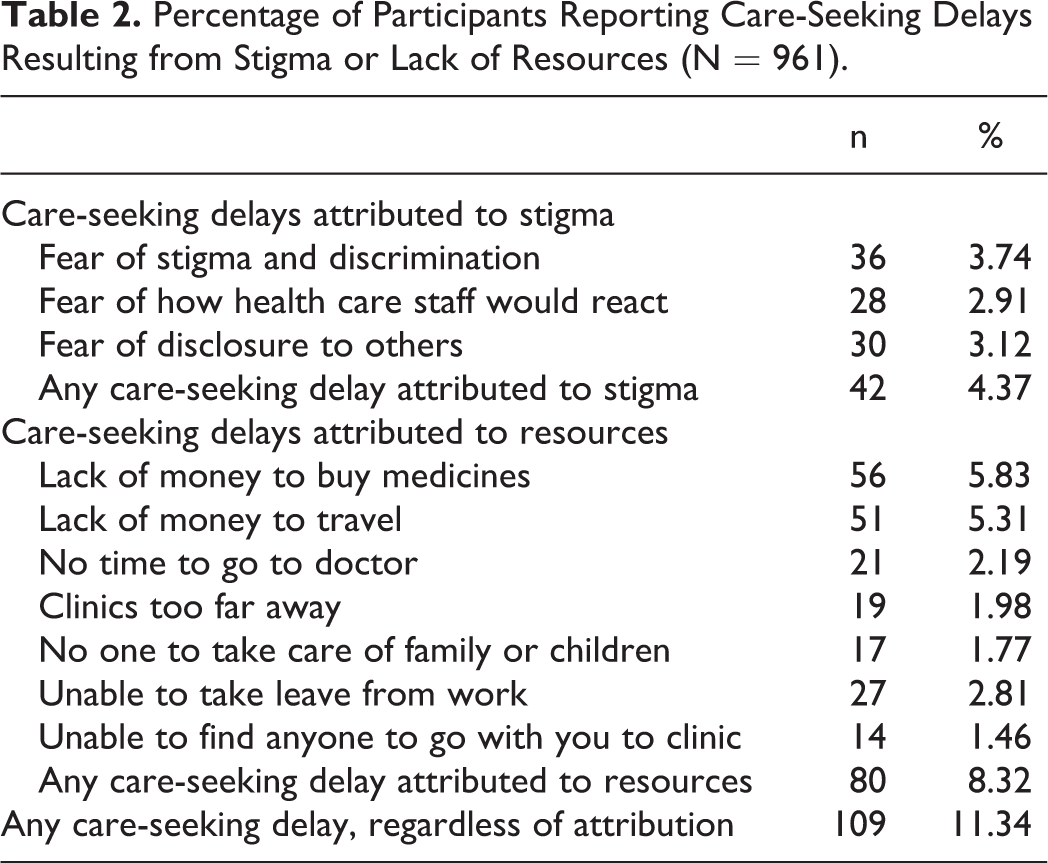
Table 3 displays the bivariate associations among stigma, disclosure avoidance, depression, and delays in care seeking. It also includes city of recruitment, time since diagnosis, and ARV drug use because these variables were significantly associated with explanatory or outcome variables of interest and hence subsequently used in regression modeling. Enacted and internalized forms of stigma were correlated with delays in care seeking, whereas vicarious and felt normative forms of stigma were not. Furthermore, disclosure avoidance and depression symptoms were correlated with enacted stigma, internalized stigma, and delays in care seeking.
Bivariate Associations among Stigma, Disclosure Avoidance, Depression Symptoms, and Delays in Care Seeking.a

Abbreviation: BDI, Beck Depression Inventory.
aCorrelations among city, yrs, ARV, BDI, and DCS were tested with the Pearson product-moment correlations. Associations involving ordinal variables (ES, VS, FS, IS, DA) were tested with Spearman's rho. City was coded as: 0 = Bengaluru, 1 = Mumbai.
*P < .05.
**P < .01.
Testing for Mediation
To examine whether the disclosure avoidance and depression symptoms might mediate the observed associations among enacted and internalized stigmas and delays in care seeking, we ran a sequence of multivariable logistic regression models. Because recruitment city, time since diagnosis, and ARV drug use had been associated with variables of interest, we controlled for them in the models. As shown in Table 4, both enacted and internalized stigmas were significant predictors of care-seeking delays when modeled without potential mediators (regression model 1). However, the associations of enacted and internalized stigmas with care-seeking delays fell to nonsignificant levels when disclosure avoidance and depression were added to the model (regression model 2). Bootstrapping methods 21 revealed that depression symptoms had a significant indirect effect on the relationship between enacted stigma and delays in care seeking and that both disclosure avoidance and depression symptoms had significant indirect effects on the relationship between internalized stigma and delays in care seeking (Table 4, Point Estimates of Indirect Effects). These findings are indicative of mediation.
Mulitvariable Models Testing Whether Disclosure Avoidance and Depression Symptoms Mediate the Associations between Stigma and Delays in Care Seeking.
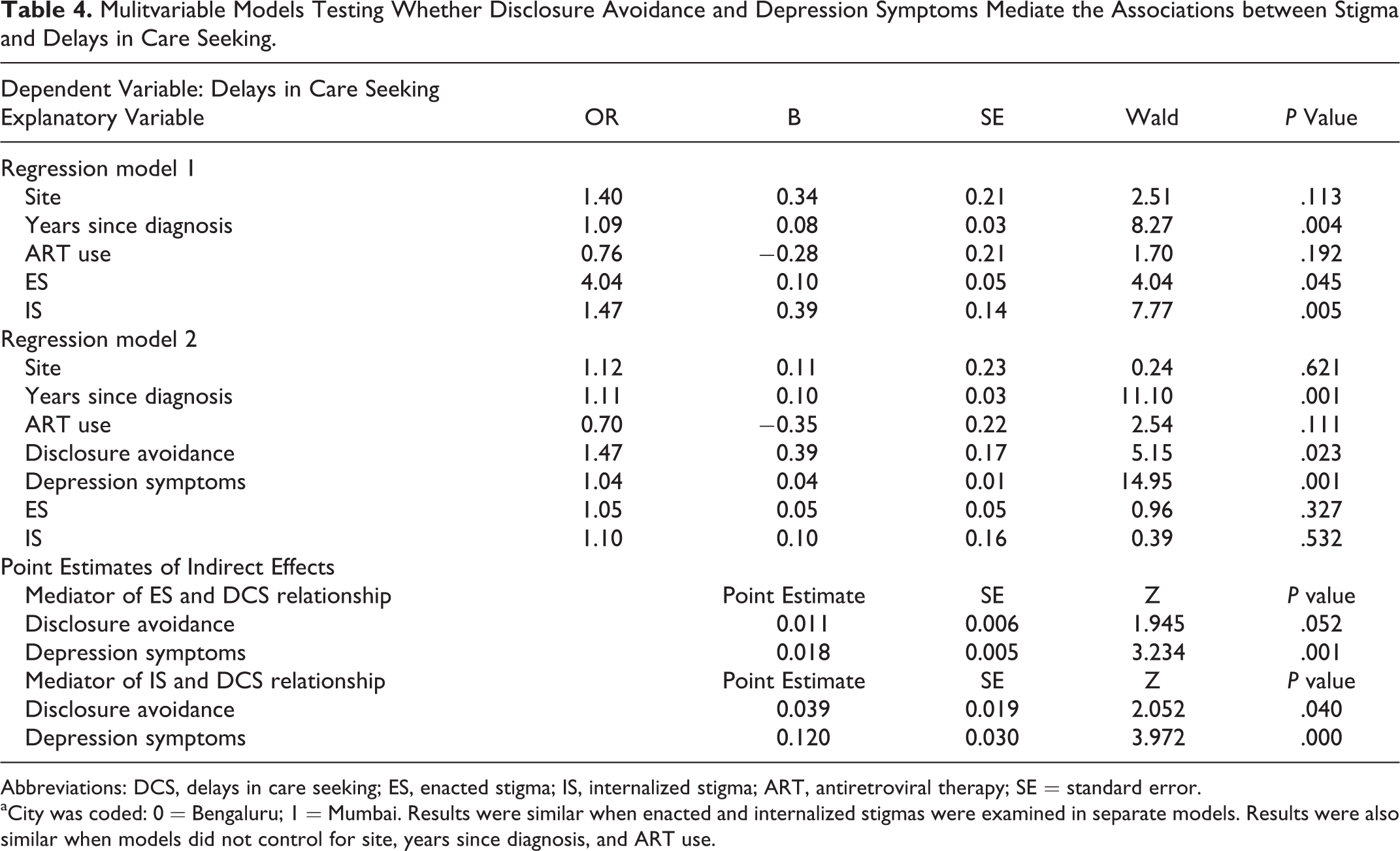
Abbreviations: DCS, delays in care seeking; ES, enacted stigma; IS, internalized stigma; ART, antiretroviral therapy; SE = standard error.
aCity was coded: 0 = Bengaluru; 1 = Mumbai. Results were similar when enacted and internalized stigmas were examined in separate models. Results were also similar when models did not control for site, years since diagnosis, and ART use.
Discussion
Our findings revealed that both enacted and internalized forms of stigma were correlated with self-reported delays in seeking care after testing positive for HIV. People who experienced discrimination and prejudice were more likely to report feeling depressed, which in turn was associated with greater reports of care-seeking delays. Similarly, HIV-infected people who held their own prejudicial views about the disease were more likely to avoid disclosing their HIV status and to experience depression symptoms, which were correlated with a greater likelihood of reporting care-seeking delays. These findings are consistent with a variety of prior research showing that avoiding disclosure of a stigmatized status cuts off people from resources in their social support network, increases the risks for depression, and impairs the overall well-being. 12,13,22 –24
Highlighting stigma’s pervasive influence, the observed pattern of associations was similar both for care-seeking delays explicitly attributed to stigma and those attributed to an absence of resources (eg, lack of money for travel). Sometimes stigma’s impact on a situation is direct, such as when a person chooses not to seek health care because he or she specifically fears mistreatment by hospital staff. But at other times, stigma’s impact is more indirect. For example, a person may be uncomfortable revealing his or her HIV status to family members, is then unable to ask for financial help, and ends up not having sufficient funds to travel for medical appointments. Unfortunately, regardless of the cause, delaying care has potentially devastating consequences. It may reduce the success of treatment once it is finally sought 5 and increases the likelihood that infected individuals—who have relatively higher viral loads while untreated—will pass the virus to sexual partners. 6 Furthermore, stigma may increase the chances that a person with HIV will cycle in and out of treatment—for example, by missing clinic appointments or failing to refill prescriptions in a timely manner. Prior work by our team has shown that treatment interruptions are a major contributor to suboptimal ARV drug adherence in parts of India, which is associated with resistance mutations to first-line ARV regimens used in the country. 25
At first pass, it may seem counterintuitive that we did not observe a relationship between care-seeking delays and felt normative stigma. By definition, this form of stigma involves perceptions that others in the community have prejudicial attitudes, which in turn would be expected to drive decisions about when and where to seek treatment. The absence of a significant correlation suggests that the critical factor in determining people’s care-seeking decisions may be the perception that they can cope with potential prejudice, rather than the expectation that prejudice exits. It is notable that care-seeking delays were more common among people reporting higher levels of internalized stigma and depression. Those who believe they deserve to be targets of discrimination and who experience the negative affect and lack of motivation typical of depression would be expected to have relatively little self-efficacy, especially when confronting the challenges of HIV-related discrimination. Further research will be necessary to prove conclusively that coping expectations explain the observed differences in our felt normative and internalized stigma-related findings. But if our hypothesis is true, it would have important implications for intervention. It is likely not sufficient to advise people to disclose their HIV status, as not all individuals will have the emotional resiliency to handle potentially negative reactions from family and friends. Rather, interventions must seek first to instill a sense of self-worth and of agency. We previously observed marked improvements in internalized stigma and depression after simply asking people to reflect regularly on their experiences. 12 This suggests that relatively straightforward and easily implemented intervention procedures could potentially provide a foundation for greater psychological resiliency among HIV-infected individuals in India. Furthermore, for people who lack supportive family and friends, it may be possible to build—and have the participants enjoy the benefits of—alternate support networks created through an intervention.
Our research has several limitations. First, the cross-sectional design limits our ability to determine directionality in observed relationships. While it is plausible that enacted and internalized stigma affected decisions about care, it also is possible that failing to seek care reinforces negative beliefs about oneself and hence contributes to internalized stigma. Prior longitudinal work suggests that other key stigma associations are bidirectional, with stigma both reinforcing and being reinforced by disclosure avoidance and depression. The same may also be true of the relationship between stigma and care-seeking delays. Second, our data rely on participant self-reports, which could be influenced by poor recall, selective memory, or a desire to present oneself in a particular way during study participation. We do not have any reason to believe that these factors would systematically bias responses in one direction, but we cannot fully rule out the possibility. Third, our questions asked only whether care-seeking delays had ever occurred. They do not allow us to determine how long delays lasted or when exactly they occurred. More nuanced information would permit a better understanding of how exactly stigma influences care seeking in different situations. Finally, our recruitment strategies, most especially the use of referrals from providers, preclude us from determining refusal rates (as only those agreeing to participate were referred) or from understanding how participants differed from those who chose not to be in the study. We do not have any reason to believe that our participants differed systematically from others on stigma or care-seeking delays, but we also cannot rule out the possibility completely.
Stigma continues to have profound effects on people living with HIV in India. Our research indicates that experiences of discrimination and internalized prejudicial beliefs are associated with whether or not care is sought in a timely manner. It is vital that we conduct further research to better understand this relationship and address it. Receipt of appropriate medical care is a key component of modern efforts to treat and prevent HIV. Global efforts to combat HIV will not be successful if people remain wary of accessing care and intervention services.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an award to ML Ekstrand by the John E. Fogarty International Center for Advanced Study in the Health Sciences at the United States National Institutes of Health (R01TW006314).