
Abstract
People living with HIV are at high risk for anal cancer (AC); however, the impact of screening for and treatment of precancerous anal lesions on AC incidence remains uncertain. In 2013, we conducted a survey of HIV providers evaluating the perceived need for an institutional AC screening program. Based on an overwhelmingly positive response, we established a dedicated AC screening clinic (including provision of high-resolution anoscopies) embedded within the institutional HIV clinic. Here, we describe that referral of high-risk patients in the first 3 years was lower than expected. Referral patterns suggest that screening practices vary widely among HIV providers within the institution. Anal cancer clinic patients who completed a perception survey rated the value of AC screening as high, with perceived positive health impact, and identified their providers as the main source of information on AC and AC screening. Our findings imply remaining provider-related barriers to AC screening.
Keywords
What Do We Already Know about This Topic?
Anal cancer screening is generally well accepted by patients; however, screening practices vary widely between providers and regions.
How Does Your Research Contribute to the Field?
By analyzing referral patters to a recently opened anal cancer screening clinic and patients’ perception of the clinic, we show that patients value anal cancer screening highly but that uptake of screening varies widely even among providers of one clinic; we discuss potential barriers impacting screening.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
Our results emphasize the importance of educating providers and patients on anal cancer screening, the urgent need for improved evidence-based understanding of the impact of anal cancer screening, as well as the need for nationwide screening guidelines.
Introduction
Incidence of anal cancer (AC) has been rising over the last 4 decades in the general US population and is up to 50 times higher among high-risk populations. 1 However, among men who are men who have sex with men (MSM) living with HIV, the upward trend in incidence appear to be stabilizing since 2008, 2 possibly due the impact of effective antiretroviral therapy or more screening in this population. The impact of screening on incidence, morbidity, and mortality of AC has however not been demonstrated, and there are no national guidelines for screening in high-risk populations. Providers of various medical subspecialties caring for people living with HIV (PLWH) have initiated AC screening modeled after cervical cancer screening programs, most commonly starting with a digital anorectal exam (DARE) and anal cytology testing from Papanicolaou smear, followed by high-resolution anoscopy (HRA) for abnormal cytology results and treatment of high-grade precancerous lesions. 3,4 HIV providers at our institution offer specialty and primary care for approximately 2800 adult PLWH across 3 clinics. As of 2013, an AC screening program and access to screening HRA in the outpatient setting were lacking. HRA referral options were limited to 2 colorectal surgeons within the institution who performed the procedure only under general anesthesia and 1 colorectal surgeon in private practice. Herein we describe efforts undertaken to implement a dedicated AC screening clinic (subsequently referred to as ACSC) based on provider feedback, characterize referral patterns to the new ACSC, and share clinical findings and survey results of patients screened through this clinic.
Provider Survey
In June 2013, an anonymous online survey contacted 47 HIV care providers at the institution to evaluate knowledge of AC screening and perceived need for a standardized, comprehensive, clinic-based screening program. Twenty-six providers responded to the survey of whom 2 only provided demographic information and were not included in further analysis, 13(54.2%) performed anal pap smears, 14 (58.3%) respondents would prefer another provider to conduct the screening, and 23 (95.6%) supported the establishment of a dedicated ACSC. 5
Implementation of Screening Program
In August 2013, 2 providers attended the “American Society of Colposcopy and Cervical Pathology Comprehensive Colposcopy and HRA” course, followed by 22 hours of observation of HRAs in the clinics of 2 highly experienced providers within 2 health systems. The dedicated ACSC, embedded in 1 of the 3 HIV clinics, opened in January 2015. The HRA providers organized educational lectures and case discussions for all staff of the HIV clinics and advertised the ACSC through e-mail and staff meetings. Patients of all 3 HIV clinics were eligible for referral including for initial screening with DARE and anal cytology testing or for HRA following abnormal anal cytology results, defined as atypical squamous cells of undetermined significance, low-grade squamous intraepithelial lesion, or high-grade squamous intraepithelial lesion (HSIL). It was emphasized to consider AC screening at least for high-risk patients according to New York State Department of Health guidelines 6 (MSM, women with prior abnormal cervical cytology, and patients with history of external genital warts).
From January through August 2015, the ACSC was staffed one half-day per week with the 2 HRA providers. In August 2015, both providers left their full-time positions; one continued to see patients twice per month as volunteer. In November 2016, all 3 HIV clinics merged into one, thus allowing all patients to have AC screening within their “home clinic.” Due to insufficient referrals from within the institution, the ACSC was opened for referrals from outside University of Maryland Medical System (UMMS) in early 2017.
Referral Patterns
As of December 2018, 116 unique patients (112 male, 1 female, and 3 transwomen) had been seen in the ACSC, of which 113 underwent HRA and 32 came for at least 1 follow-up evaluation with HRA, with no-show rates of approximately 25%. Two patients were HIV-uninfected MSM receiving HIV preexposure prophylaxis. Fourteen patients were referred from outside UMMS, and 16 patients were referred from the primary care clinics of the 2 HRA providers. Twenty-one different providers who see patients in the institution’s HIV clinics referred the remaining 86 patients; 40.7% of these referrals came from 2 female providers who referred 19 and 16 patients, respectively. Forty-one (35%) patients were diagnosed with HSIL on anal cytology or biopsy and were offered further evaluation or treatment. The primary treatments recommended for biopsy-confirmed HSIL were office-based infrared coagulation and surgical referral. 7
Patient Survey
In June 2015, a prospective cohort study was implemented enrolling patients of the ACSC into a knowledge and perceptions survey regarding anal health utilizing a self-administered questionnaire. Study protocol HP-00062615 was approved by the University of Maryland, Baltimore Institutional Review Board and the University of Maryland Midtown Hospital Research Committee. Inclusion criteria were age ≥ 18 years, living with HIV, and being a patient at the ACSC; prior history of AC was an exclusion. From June 2015 to December 2018, 72 patients signed informed consent and were given the questionnaire of which 47 (65.3%) returned it completed, mostly after their first clinic visit. Nine patients declined to participate, and participation was not offered to 34 patients due to not meeting inclusion criteria or inadequate resources to to discuss the study with patients. All study participants were men and the majority (79%) were African American, similar to the clinic demographic. Questionnaire nonrespondents did not differ significantly from respondents by age (mean age 41.1 vs 39.3 years respectively; P = 0.5) or race and ethnicity (P = 0.7).
Respondents had received the HIV diagnosis between 1985 and 2017, with only 25% being diagnosed after 2010. All had completed some form of formal education; median household income fell within $30,000 and $50,000 a year, with 38.3% making below $30,000. Fifty percent of patients were covered by Medicaid/Medical Assistance Programs, 43.4% by private insurance, and 6.5% by Ryan White. The reported payer mix differed from the general clinic population (80% Medicaid, 12% Medicare, 5% Private, and 3% Ryan White).
As expected for a screening clinic, the majority (59%) of respondents were asymptomatic with regard to anal symptoms. Among those with symptoms, the most common were anal pain (24%), bleeding (22%), and itching (15%). In all, 38% had prior diagnosis of hemorrhoids, 13% had discharge, 23% had abscess, and 11% had anal tears. Prior anorectal procedures included wart removal (24%), endoscopies (35%), and unspecified surgical procedures (24%). There was no statistically significant difference in likelihood of an endoscopic procedure in those older than 50 years (44%) versus under (32%; P = 0.5).
Only 23 (49%) of the 47 respondents reported having ever had DARE, with a higher proportion of patients older than 40 years reporting it, but the difference was not statistically significant. Thirty-four (72.3%) respondents reported having had prior anal cytology, 60% within 1 year of referral, and 11 reported a previous diagnosis of anal dysplasia. Nineteen (40%) reported having had a prior HRA. There was variable awareness of anal cytology test (77%), HRA (53%), knowing someone who had AC screening (4%), or who had AC (21%). Only 1 patient felt “very well informed” on anal dysplasia and AC. Self-reported knowledge did not differ by age or prior college education. The most commonly reported source of information about anal dysplasia and AC was the doctor’s office (67%; Table 1).
Demographics and Results on Questions Regarding Knowledge of Anal Cancer and Perception of Anal Cancer Screening for 47 Survey Respondents.
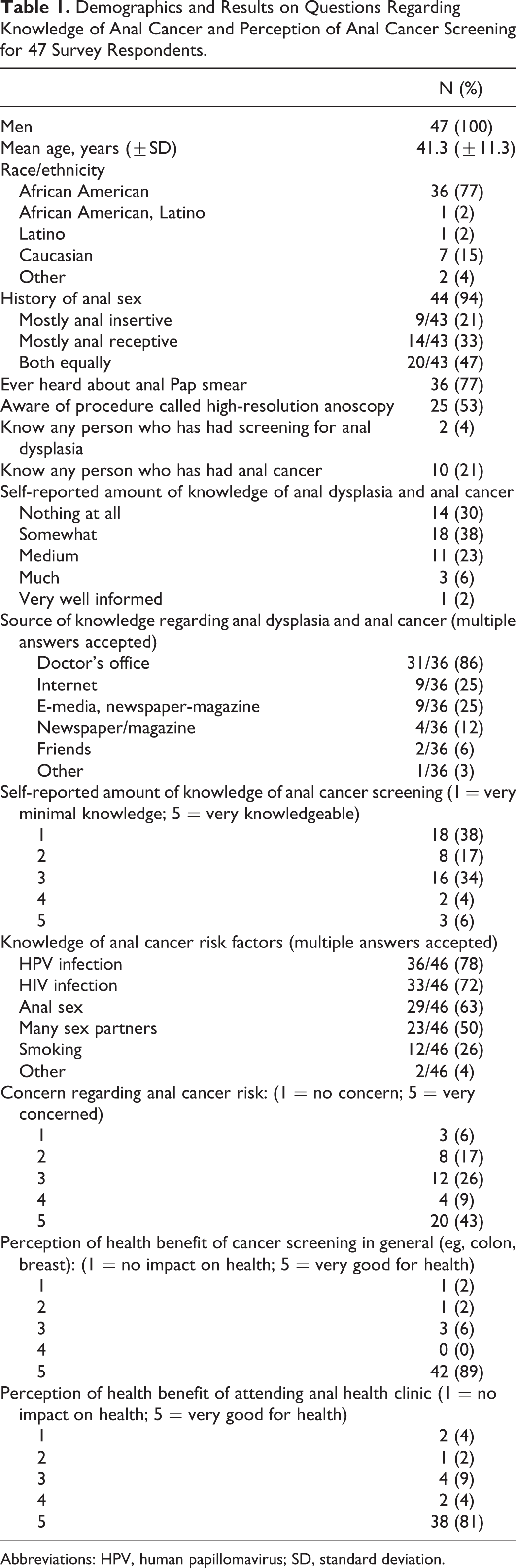
Abbreviations: HPV, human papillomavirus; SD, standard deviation.
Respondents were aware of AC risk factors, identifying receptive anal intercourse (63%), human papillomavirus (78%), HIV infection (72%), multiple sexual partners (50%), and smoking (12%) as risk factors. Respondents reported high levels of concern about AC, with 77% rating level of concern at 3 of 5 and above on the Likert-type scale. Eighty-one and 89 percent, respectively, reported that cancer screening in general and attending the AC screening clinic were “very good” for their health (Table 1).
Discussion
Patients seen in the ACSC were mostly African American MSM with HIV, a group at high risk for AC. Among ACSC patients who completed the patient survey, the majority reported being asymptomatic at time of referral, but 40% of patients reported prior anal symptoms. The proportion of ACSC patients diagnosed with HSIL on anal cytology and/or HRA-guided biopsy was high but within the expected range for this population. 8,9 ACSC survey respondents rated the potential benefit of clinic attendance to their health very positively, similar to previous studies showing high patient satisfaction with anal dysplasia screening and evaluation. 10 No-show rates in the ACSC were comparatively low for an inner-city clinic, supporting patient acceptance of the service. The majority of survey respondents reported learning about anal dysplasia and AC in their physician’s office and had fair knowledge of risk factors, but an analysis of the referral patterns to the ACSC from individual HIV providers suggested that not all consistently perform AC screening; this observation is also supported by the low proportion of survey respondents reporting prior DARE and anal cytology screening. Between clinic inception and December 2018, less than 50% of the HIV clinic providers ever referred patients to the ACSC, and the number of referred patients were below the estimated number of high-risk patients. Within the HIV clinic population, approximately 15% of patients self-identify as MSM, suggesting that around 420 patients would have been eligible for AC screening based on this risk factor alone; with an estimated prevalence of abnormal cytology in this population of 60% or higher approximately 250 MSM would have been expected to be eligible for HRA based screening. 8 Women living with HIV and having a history of abnormal anogenital histology are also at increased risk for AC, but only 1 female and 3 transwomen were seen in the ACSC. These referral patterns were somewhat surprising, as 95.6% of providers participating in the 2013 preimplementation survey supported the establishment of the institutional ACSC as an important part of HIV care. However, other reports have suggested that provider-related barriers impact preventive screening, 11 especially around sensitive topics such as anal health. 12 Using in-depth interviews with 58 MSM living with HIV, Koskan et al found that patients were eager to learn about AC but reported a lack of recommendations from and discussion with their physicians as a major barrier to screening. 13
The low scores on AC self-perceived knowledge in our survey support a need for providers to discuss AC risk with their patients. However, awareness of some individual risk factors for AC was high, suggesting that referred patients had either discussed their risk with their providers or had information from other sources.
Contributing factors for not identifying, screening, or referring at-risk patients may have been provider comfort level with discussing AC screening and performing anal cytology 14 providers’ unconfirmed assumptions regarding patients’ sexual orientation and practices, 15,16 and time constraints during clinic visits. 17 Consistent with our previous provider survey findings, male providers were less likely to refer their patients for screening, and the 2 highest referring providers to the clinic were female. 5 The lack of clinical trial data on the impact of AC screening adds uncertainty around the value of screening. The ANCHOR (ANal Cancer/HSIL Outcomes Research) study is currently enrolling more than 5000 patients in the mainland United States and in Puerto Rico to better understand the impact of HSIL detection and treatment on AC incidence. 18
Limitations of this short communication include lack of information on number and results of anal cytologies performed among all HIV clinic patients; lack of information on patients who declined AC screening or ACSC referral; incomplete enrollment of ACSC patients into the survey and only partial survey completion as well as biases associated with questionnaire design and responses. 19 Future research should evaluate perceptions and knowledge on AC screening among all patients in the HIV clinic as well as discussions with providers to explore barriers to screening.
In conclusion, by linking the ACSC implementation with providers’ referral patterns and patients’ perceptions, our findings suggest wide differences in provider practices regarding AC screening and overall very positive perception and acceptance of AC screening, including HRA, by referred patients. Given the high incidence of AC in some populations, high-risk patients should be empowered to make informed decision regarding their participation in AC screening, especially as surveys of patients in AC screening programs do not suggest a negative impact of screening on psychological well-being. 20
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Leonard A Sowah is currently employed by National Institute of Allergy and Infectious Diseases, Bethesda, MD, USA. The views expressed here are his personal views and do not represent the views of the NIH. Ulrike K Buchwald is currently employed by Merck & Co, Inc., Kenilworth, NJ, USA and may hold stock and or stock options in the company.
Funding
The author(s) disclosed receipt of the following financial support for the research, and/or authorship of this article: Ryan White Part A Clinical Quality Improvement grant funds were used to develop an embedded anal cancer-screening clinic. HRSA Ryan White Part A Clinical Quality Improvement support was used for the purchase of anoscopy equipment.