
Abstract
Persons living with HIV (PLWHs) are at high risk for medication errors when hospitalized, but antiretroviral medications are not often evaluated by antimicrobial stewardship programs (ASPs) because they are not specifically discussed in the standards of practice. However, antiretroviral (ARV) stewardship programs (ARVSPs) have been shown to decrease medication error rates and improve other outcomes. The goal of this article is to review published literature on ARVSPs and provide guidance on key aspects of ARVSPs. A MEDLINE search using the term “antiretroviral stewardship” was conducted. Original research articles evaluating ARVSPs in hospitalized, adult PLWHs were included. Six original research articles evaluating unique inpatient ARVSPs met inclusion criteria. All 6 studies evaluating medication errors as the primary outcome found a significant reduction in errors in the postimplementation phase. Based on current standards for ASPs, we propose core elements for ARVSPs. Future organizational guidelines for antimicrobial stewardship should include official recommendations for ARV medications.
What Do We Already Know about This Topic?
Persons living with HIV are at high risk for medication errors when hospitalized, but antiretroviral medications are not often evaluated by antimicrobial stewardship programs because they are not specifically discussed in the standards of practice.
How Does Your Research Contribute to the Field?
This article increases awareness of the importance of antiretroviral stewardship and provides needed guidance on key aspects of antiretroviral stewardship programs.
What Are Your Research’s Implications Toward Theory, Practice, or Policy?
This article has the potential to impact practice and policy by advocating for implementation of antiretroviral stewardship programs at institutions and inclusion of antiretroviral stewardship in antimicrobial stewardship standards of practice.
Introduction
Organizations such as the Joint Commission, Centers for Disease Control and Prevention, Infectious Diseases Society of America, and the Society of Healthcare Epidemiology of America provide specific guidance on antimicrobial stewardship recommendations and standards. 1 -3 While antimicrobial stewardship programs and processes are fairly well established at most institutions, they typically focus on antibiotics and antifungals. 4 This leaves antivirals without systematic evaluation by a specialist, as they are often not specifically discussed in these standards.
People living with HIV (PLWH) are often complex and at higher risk for medication errors during hospitalizations. Medication error rates in PLWH vary widely from 5% to 86% and are likely the result of antiretroviral therapy (ART) complexity and/or unfamiliarity. Medications for opportunistic infection (OI) treatment and prophylaxis are also at risk for errors. Medication errors may occur during the prescribing, dispensing, administration, or medication reconciliation process. Most medication errors in PLWH occur on admission, with more than one-third remaining uncorrected at discharge. 5
Factors contributing to inpatient ART errors include failure to complete or incomplete medication reconciliation, institutional formulary restrictions, concomitant medication changes, swallowing difficulties, and fluctuations in renal and/or hepatic function. 5 Providers without specialized HIV training may not be equipped to recognize and manage these complex situations. 6 Although detailed treatment and management guidelines 7 -9 exist, HIV pharmacotherapy is constantly evolving. People living with HIV who receive treatment by an HIV expert, including physicians and pharmacists, have better adherence, improved outcomes, decreased mortality, and lower costs. 10 -14
Antiretroviral stewardship programs (ARVSPs) have been shown to decrease medication error rates and improve other outcomes. 15 -20 This article reviews published literature on ARVSPs and provides guidance on key aspects of ARVSPs for those looking to implement programs at their institutions.
Methods
A MEDLINE search using the term “antiretroviral stewardship” was conducted by the authors. Original research articles evaluating ARVSPs in hospitalized adults with HIV (≥18 years of age) without restriction to publication date were included.
Ethical Approval and Informed Consent
Ethical approval and informed consent were not needed since this manuscript was a critical research review of previously published data.
Results
Our search returned 18 articles. Twelve articles did not meet inclusion criteria and were excluded (9 unrelated topic, 1 pediatric ambulatory clinic, 1 editorial, 1 news article). Six original research articles evaluating unique inpatient ARVSPs were included in our review. These articles were published between January 29, 2014 and January 22, 2019, and included data from September 2010 to December 2014.
A summary of published ARVSP program interventions and outcomes is presented in Table 1. All studies were quasi-experimental studies in adult PLWH prescribed ART. All programs included a prospective audit and feedback component. This was either initiated with the intervention phase or was standard of care at baseline (preintervention) and continued. They also included at least 1 additional element, which ranged from education to electronic medical record (EMR) modifications. 15 -20 Examples of EMR modifications included alterations to default doses and frequencies 10,15,19 and links to drug information resources. 18
ARVSP Interventions and Outcomes.

Abbreviations: ART, antiretroviral therapy; ARVSP, antiretroviral stewardship program; CSDDI, clinically significant drug–drug interaction; EMR, electronic medical record; ID, infectious diseases; No., number; OI, opportunistic infection.
All 6 studies evaluating medication errors as their primary outcome found a significant reduction in errors in the postimplementation phase. 15 -19 Two of these studies also evaluated error resolution and found it to be significantly better in the postimplementation phase. 17,18 Additionally, 2 of the studies conducted a logistic regression analysis and found postintervention phases were independently associated with reduced ART errors. 15,16 One study evaluated clinically significant drug–drug interactions (CSDDIs) as the primary outcome. Similarly, this study found significantly fewer CSDDIs at admission and during hospitalization in the postimplementation phase. 17 All studies concluded their ARVSP interventions were beneficial.
Discussion
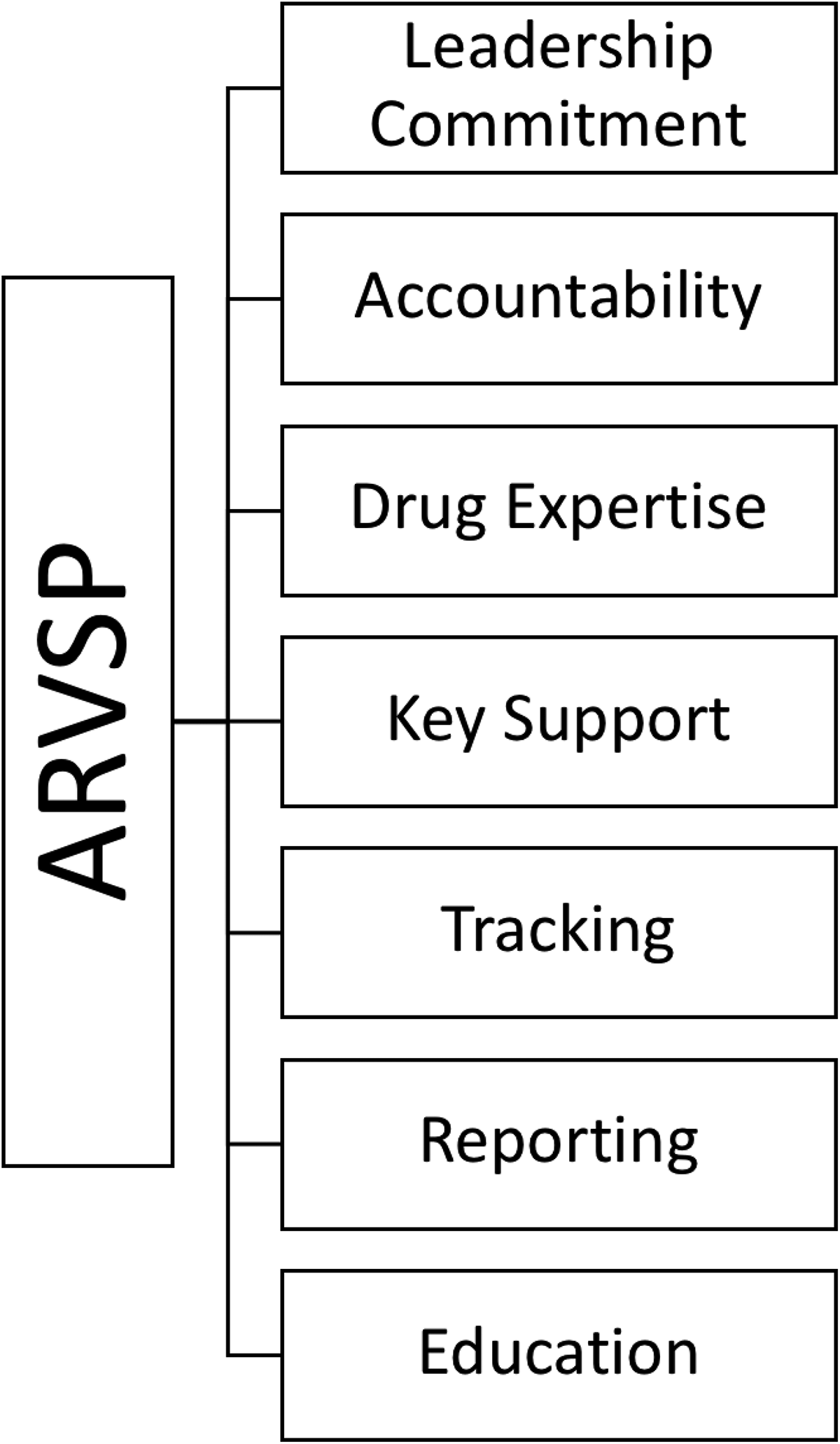
Although studies show improved outcomes with ARVSP interventions, 15 -20 there is limited guidance on standards for implementing these services. Based on clinical experience and published evidence, we adapted the core elements of antibiotic stewardship programs (ASPs) 1,2 for ARVSPs. Our proposed core elements of ARVSPs can be found in Figure 1.
While this article focuses on inpatient antiretroviral stewardship, other antiviral medications and prophylaxis for OIs may be important to consider as well. Additional examples include hepatitis C direct-acting antivirals, respiratory antivirals, and antivirals for treatment and prophylaxis of infections in transplant recipients. 21 -23 Furthermore, antiretroviral stewardship is critical in the ambulatory setting, since most ART is prescribed outpatient.
Leadership Commitment
As with any program, establishing commitment from leadership is required to ensure there are sufficient resources and support for programmatic success. Appropriate full-time equivalents (FTEs), funding, technology, and other resources cannot be secured without the backing of hospital leadership. Additionally, leadership commitment is needed for successful approval and uptake of ARVSP policies and procedures. Depending on need and resources, antiretroviral stewardship may be a separate program or incorporated into the existing ASP.
Accountability
A single leader is generally appointed and accountable for program outcomes. This could be a physician or pharmacist. Depending on resources and area of expertise, the ARVSP leader may be the same as or different from the existing ASP.
Drug Expertise
Expertise in HIV pharmacotherapy is essential because of the complexities of PLWH and ART and high rates of medication errors. While not well defined, expertise in HIV may be accomplished by greater experience in the care of PLWH, most commonly provided through formal training and/or advanced certification (eg, American Academy of HIV Medicine), both of which should be supplemented by continuing medical education. Ideally, an on-site pharmacist with expertise in HIV pharmacotherapy, in conjunction with physician support, is best suited. Postgraduate trainees, if available, should also be engaged to provide experience and overcome potential limitations. While this may not be feasible in all centers, telemedicine, similar to that used by many ASPs, may provide the necessary support for HIV expertise in resource-limited settings. 24,25
Key Support
Due to the complexities in ARVSPs, support from key members is critical to their success. Similar to ASPs, clinicians and department heads must be engaged to support the multifaceted efforts needed to improve the management of PLWH. Information technology (IT) staff are vital to providing electronic health record access across the health system and to any affiliated specialty clinics or pharmacies, developing clinical decision support systems to trigger alerts notifying ARVSPs when ART is initiated, developing prompts to alert clinicians of potential drug interactions or dosing errors. In addition, IT staff are essential in collecting and reporting data to track ARVSP outcomes and safety data to quality improvement staff and the rest of the organization. Nurses’ valuable contributions to ARVSP include performing medication reconciliations, monitoring patient’s progress and adherence, and providing education and counseling. A multidisciplinary approach to PLWH allows for improved care.
Action
A systematic approach to identifying PLWH who have been admitted to inpatient must be determined. Factors at individual institutions such as EMR systems and health IT can play a major role in facilitating or hindering this process. Generating a report or notification process based on diagnosis (International Classification of Diseases, 10th Revision code) or ART order have been common methods used to identify PLWH. These methods alone do have the possibility of missing certain populations such as individuals who are not receiving ART inpatient but who have an HIV diagnosis or individuals who have not had their diagnosis appropriately documented in their medical record. It is also important to discuss the initiation of ARVSP with various teams involved with inpatient care so that they can help identify PLWH who were not identified by other means.
Other than implementing a method of patient identification, the scope of the ARVSP must be determined. Factors such as funding, dedicated FTEs, and other time constraints can impact the scope of patients that may be included in the ARVSP. Ideally, all PLWH who are admitted inpatient should be included in the ARVSP and monitored from hospital admission through discharge. However, based on coverage availability and time constraints, ARVSP may need to be limited to subpopulations such as clinic patients for a specific institutions, specific hospital units, or review of only the initial admission.
Use of a medication checklist, such as the one included in the opinion paper by Durham and colleagues 5 from the HIV Practice and Research Network of the American College of Clinical Pharmacy, may help decrease medication errors and subsequent readmissions. Medication reconciliation and counseling should be performed on admission and discharge using a prospective audit and feedback approach. To ensure accuracy, ART and OI medications should be confirmed with the patient and/or caregiver, in addition to the ambulatory HIV provider and pharmacy. Most importantly, ART adherence should be assessed, which may be accomplished through patient discussion, reviewing prescription fill history, or evaluating virologic and immunologic laboratory tests. Prior to verifying and dispensing the prescription, the pharmacist should verify appropriate dosing, scheduling, route of administration, and formulation in relation to renal or hepatic dysfunction and food requirements as well as assess the patient’s medication administration record for potential drug–drug interactions (DDIs). These important tasks should continue to be performed throughout the hospitalization.
Formulary management presents a significant challenge with over 40 Food and Drug Administration–approved antiretroviral (ARV) medicines, some of which are individual components in a variety of formulations while others are fixed-dose combinations (FDCs) and even monoclonal antibodies. In addition, ARV medicines are expensive and may not be used as frequently as antibacterial or antifungal agents. Furthermore, treatment guidelines are frequently changing, most recently shifting away from non-nucleoside reverse transcriptase inhibitor (NNRTI)- and protease inhibitor (PI)-based regimens to where all recommended initial regimens contain an integrase strand transfer inhibitor (INSTI) plus 2 nucleoside reverse transcriptase inhibitors (NRTIs). 7 While some facilities may opt to stock some ARV medicines, outpatient providers must be included in the decision as to which ARV medications to include on formulary to avoid unnecessary delays in restarting ART upon admission. 26 In settings where particular ARV medications are not on formulary, patients should be permitted to use their own ARVs after verification and labeling. In some situations, alternative ARV formulations may be required to maintain the patient’s specific ART, such as splitting an FDC tablet into individual components per formulary interchange or using a liquid dosage form in patients needing enteral feeding. Additionally, short-term unplanned ART interruptions may be permitted due to toxicities, mechanical ventilation, surgical procedures, illnesses limiting oral intake, 7 or disrupted access. Frequent assessments should be performed to ensure ART is restarted as soon as possible. In select patients, ART initiation may be necessary while inpatient. Care should be taken to ensure patients are able to acquire these medicines and are scheduled for follow-up after discharge.
Among patients being initiated or maintained on ART, adherence is essential to achieve virologic suppression, which can be accomplished through patient education and adherence strategies. Ensuring that patients can obtain ART remains challenging, but federal, state, and prescription drug assistance programs are available to overcome financial barriers. 27 Both ART- and OI-related medication errors also frequently occur in the outpatient setting, 28 which is likely the result of increasing of polypharmacy due a longer life expectancy and higher rates of non-HIV associated comorbidities. 29 Use of the Beers Criteria and the Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions criteria have been shown to decrease polypharmacy and inappropriate prescribing in older PLWH. 30
Tracking
Medication errors and pharmacist interventions should be documented. Standardization of documentation is important not only to ensure a systematic evaluation of patients but also to allow for tracking of outcomes. An example of a standardized note template for ART evaluation is presented in Figure 2. By developing a process that is able to be monitored for outcomes, it allows for quality assurance and can inform stakeholders on the value of ARVSP. Tracking outcomes from ARVSP can also inform the institution of areas of strengths and weaknesses for HIV care.

Sample inpatient antiretroviral therapy (ART) evaluation note template.
Reporting
Reporting of ARVSP is not anticipated to be as robust as ASP reporting. Antiretroviral stewardship programs may be a component of ASPs, although this does not necessarily assume the leaders, experts, and executors of antimicrobial stewardship will need to fulfill the same roles as the HIV expert. The goals and content being reported to providers is dependent on the setting, whether inpatient or outpatient.
Antiretroviral stewardship programs in the outpatient setting should be more comprehensive than inpatient. Likely, patients admitted to the hospital will already be on ART prescribed by an outpatient provider. Thus, the focus of ARVSPs inpatient is in preventing and rectifying ART-related medication errors. While all providers manage antimicrobials daily to some degree, managing patients on ART is not a common occurrence for most inpatient providers. These providers should receive targeted, brief reporting on ARVSP initiatives and outcomes. Topics providers may find helpful could include the most common types of ART errors being seen at the specific institution (incomplete/incorrect regimen, DDIs, etc), guideline or process updates (including reason for change), any tracked outcomes (particularly after process changes or educational interventions), situations when an additional consult may be helpful or required (ie, new diagnosis, patient off therapy, and needs to restart), and who to contact with any questions (ie, HIV expert(s)). All ARVSP updates should be periodically provided to both prescribers and pharmacists to highlight both areas in need of improvement as well as successes.
Education
One of the most impactful part of any stewardship program is the education component. It is imperative that information is disseminated in an efficient and timely manner to all parties involved in the care of PLWH. Consider the following when developing ARVSP-related education.
Target audience
This ranges from the provider ordering the ART to the pharmacist reviewing the patient medication list and orders, to the nurse who interacts with the patient daily and helps administer medications, and to the social worker who may need to be involved to ensure the patient is able to obtain the medication. At times, targeted, more robust education will be necessary for specific audiences.
Mode of communication
Consider the best method to educate the intended audience. Some education can easily be incorporated in already established newsletters or regularly scheduled department meetings. Others may require a dedicated forum, such as a grand rounds presentation or independent web-based learning. When possible, a brief action plan or learning point should be included with periodic ARVSP updates communicated with appropriate staff.
Content
Educational materials should be as succinct as possible. Selected topics that may be helpful to review in order to prevent ARV-related medication errors and ensure appropriate ARV medication prescribing include: Guideline updates New policies Formulary changes How to manage patient home medication in the setting of a limited hospital formulary When it may be appropriate to hold ART Clinically significant drug–drug interactions and how to manage them Medication-specific clinical pearls Whether to restart ART in a patient who has been off their regimen When an ID consult is warranted HIV expert(s) point of contact
Follow-Up
As the goal of education is to promote positive change and help decrease ARV-related medication errors, it is important to assess the impact of the education. If appropriate change is not noticed and similar issues persist, it may be prudent to revisit the education provided and consider an alternative approach.
Education is key to bringing awareness to issues and common errors as well as providing information and strategies to impact change. Some degree of education should be a regular component of all ARVSP updates.
Conclusion
People living with HIV are at high risk of medications errors when hospitalized, 5,6 but ARV medications are not often evaluated by ASPs because they are not specifically discussed in the standards of practice. 1 -3 However, ARVSPs have been shown to decrease medication errors and improve other outcomes. 15 -20 The core elements for ARVSPs proposed in this article can be used to guide institutions and clinicians. Future organizational guidelines for antimicrobial stewardship should include official recommendations for antiretroviral stewardship.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.